 E-submission
E-submission
Current issue
- Page Path
- HOME > Articles and issues > Current issue
- Volume 60(4); July 2026
-


Review Articles
- Angiomatoid fibrous histiocytoma: a review
- Alexander N. Perez, Phyu P. Aung
- J Pathol Transl Med. 2026;60(4):371-378. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.06.05
- 754 View
- 31 Download
-
 Abstract
Abstract
 PDF
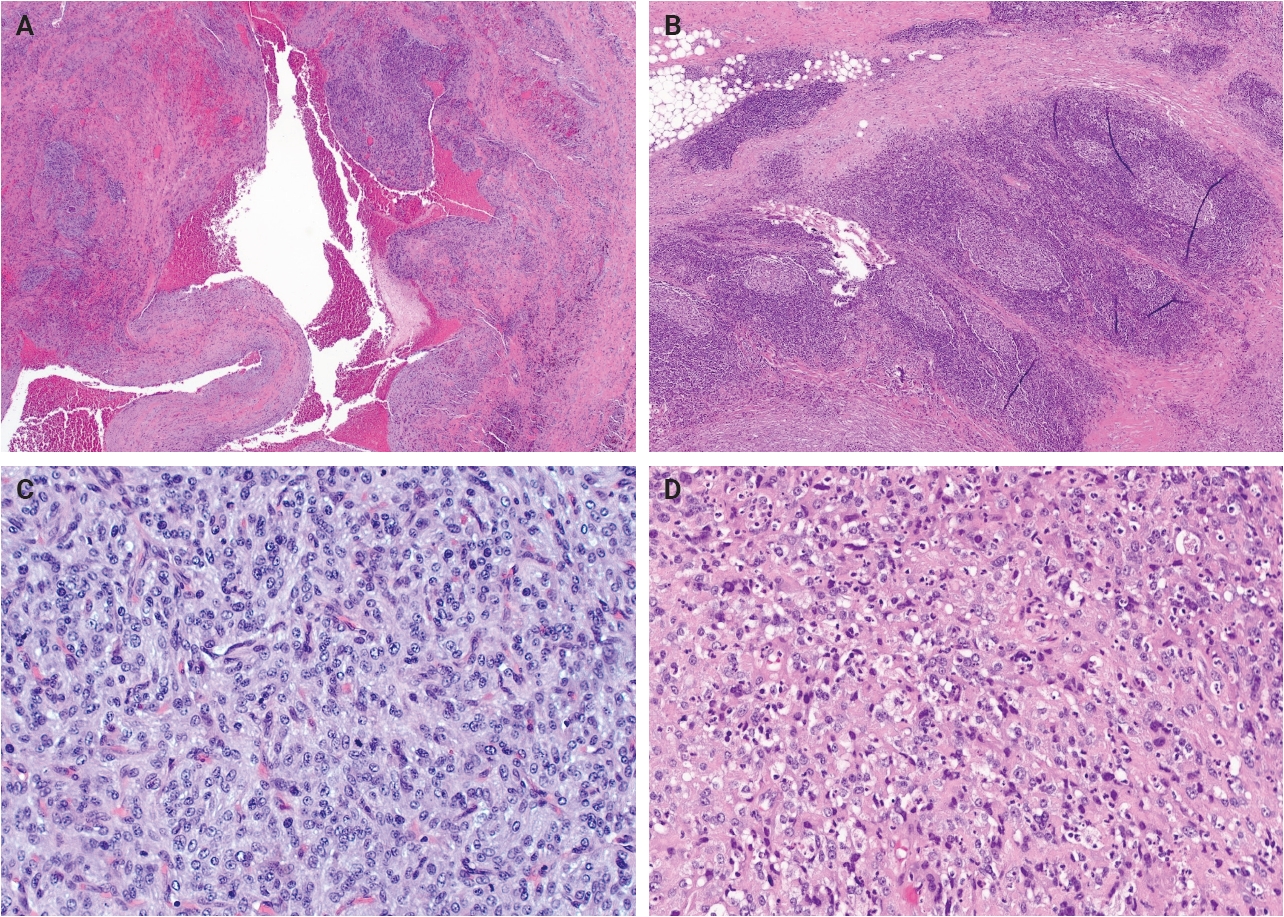
PDF - Angiomatoid fibrous histiocytoma is a rare mesenchymal neoplasm of uncertain cell lineage with indeterminate behavior, hallmarked by EWSR1 translocations. This tumor typically arises in the subcutaneous or deep soft tissues and is composed of bland to mildly atypical histiocytoid cells with frequent intralesional hemorrhagic pseudocystic spaces. It affects both children and adults, without a significant sex predilection. Histologically, the tumor may be mistaken for a lymph node given the apparent predilection for node-bearing sites as well as the brisk lymphoid cuff featuring germinal centers. Surgical excision is often curative, with local recurrence occurring occasionally and metastasis only very rarely. A possible relationship to molecularly related entities arising primarily within the thoracic cavity and intracranial compartment has been proposed, although this association remains incompletely understood.
- Ganglioglioma and gangliocytoma: a review for pathologists
- Gianfranco E. Umeres-Francia, Melissa Mejia-Bautista, Pouya Jamshidi, Jared T. Ahrendsen
- J Pathol Transl Med. 2026;60(4):379-387. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.06.06
- 694 View
- 24 Download
-
Abstract
PDF
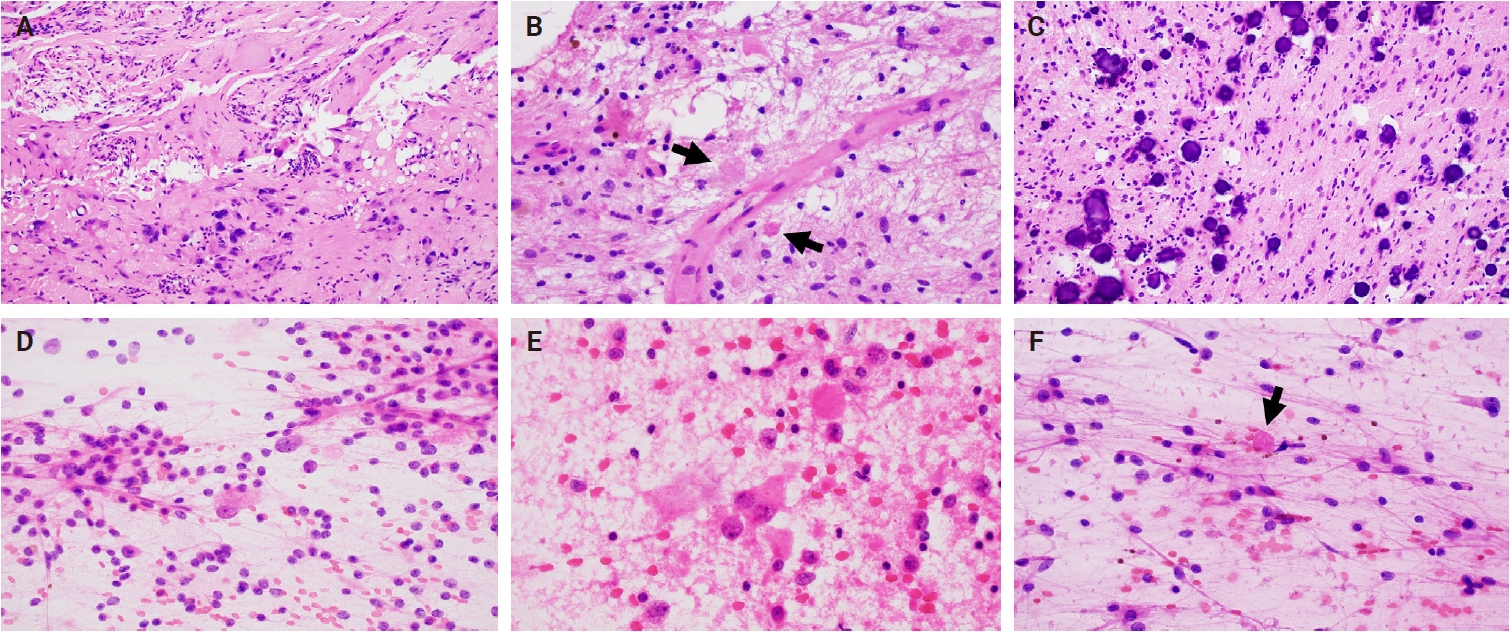
- Ganglioglioma and gangliocytoma are rare, predominantly low-grade neuroepithelial tumors that commonly present with epilepsy in children and young adults. Advances in molecular profiling have improved understanding of their pathogenesis, highlighting key roles for the mitogen-activated protein kinase/ERK signaling pathway. Diagnosis relies on a combination of clinical, radiologic, and histopathologic features, with complete surgical resection offering the best clinical outcomes. This review summarizes current knowledge on their epidemiology, etiology, clinical presentation, imaging characteristics, pathology, treatment strategies, and prognosis.
- Lymphomatoid papulosis: a practical review for pathologists
- Mario L. Marques-Piubelli, Carlos A. Torres-Cabala, Roberto N. Miranda
- J Pathol Transl Med. 2026;60(4):388-397. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.06.09
- 833 View
- 32 Download
-
Abstract
PDF
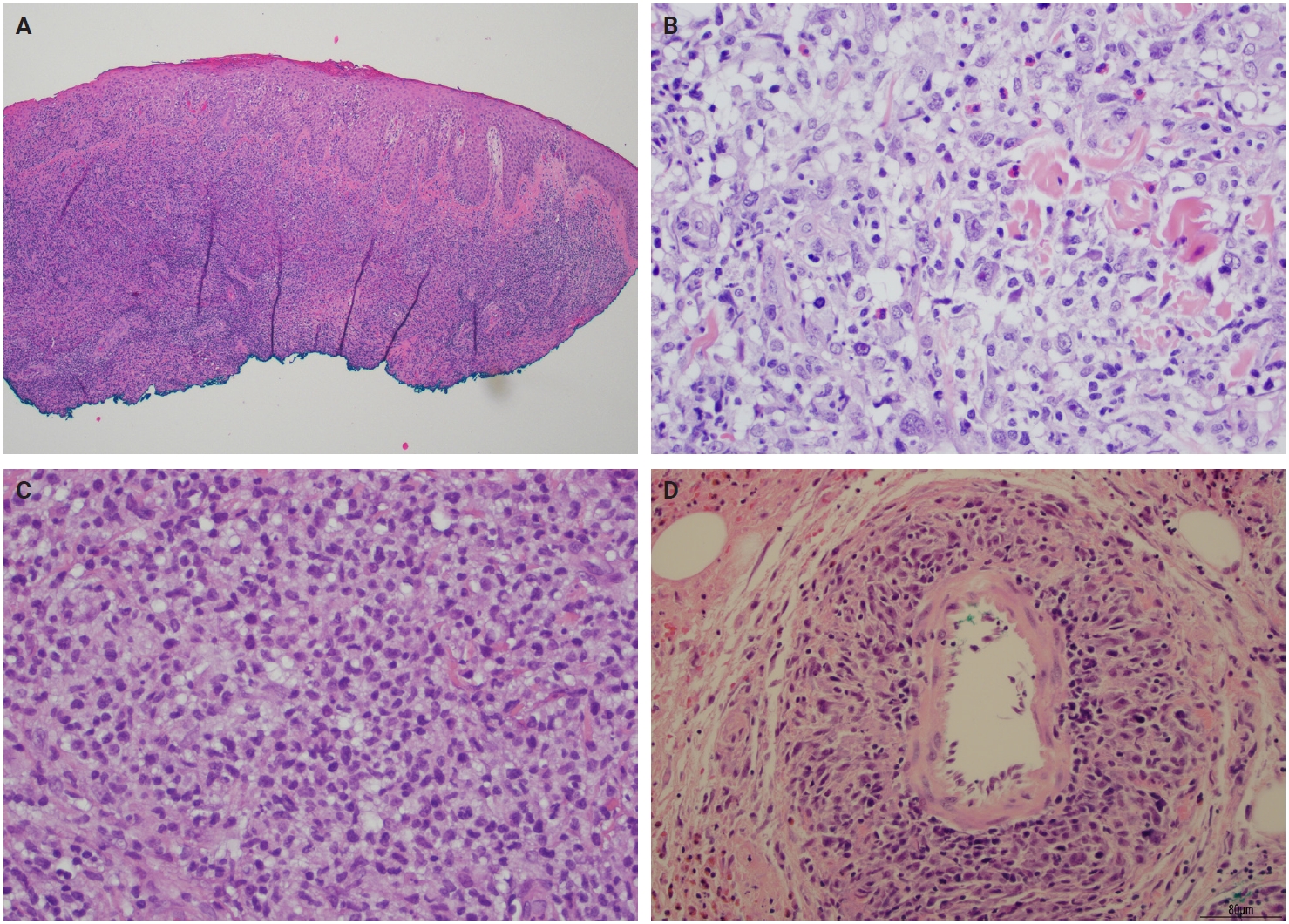
- Lymphomatoid papulosis (LyP) is a primary cutaneous CD30+ lymphoproliferative disorder characterized by a chronic and self-healing recurrent cluster of erythematous papules or nodules on the skin of the trunk and/or extremities. The disease has an indolent clinical course with spontaneous regression or waxing and waning clinical evolution. The histopathologic spectrum of LyP is vast and may show few to numerous atypical cells immersed in a mild to intense inflammatory background. The backbone for the diagnosis is the positivity for CD30, which is one of the criteria to define this group of lymphoproliferative disorders. The association of these different histological and immunophenotypical findings is used to subclassify this disease in different subtypes from A to E, associated with DUSP22/IRF4 rearrangement, and other rare forms. Although this differentiation is important to raise awareness of different differential diagnosis, it does not impact the prognosis or change the treatment, which is usually centered in symptom relief and faster regression. In this review, we aim to summarize the most updated information of the clinical, histopathological, and molecular characteristics of LyP and provide a practical assessment for the diagnostic features that could help with the main differential diagnosis.
Original Articles
- A single-institution demographic study of pathologically proven renal disease in kidney transplant recipients over the last 33 years
- Hyejin Noh, Jiyeon Kim, Yeong Jin Choi
- J Pathol Transl Med. 2026;60(4):398-412. Published online May 26, 2026
- DOI: https://doi.org/10.4132/jptm.2026.03.28
- 1,292 View
- 21 Download
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Background
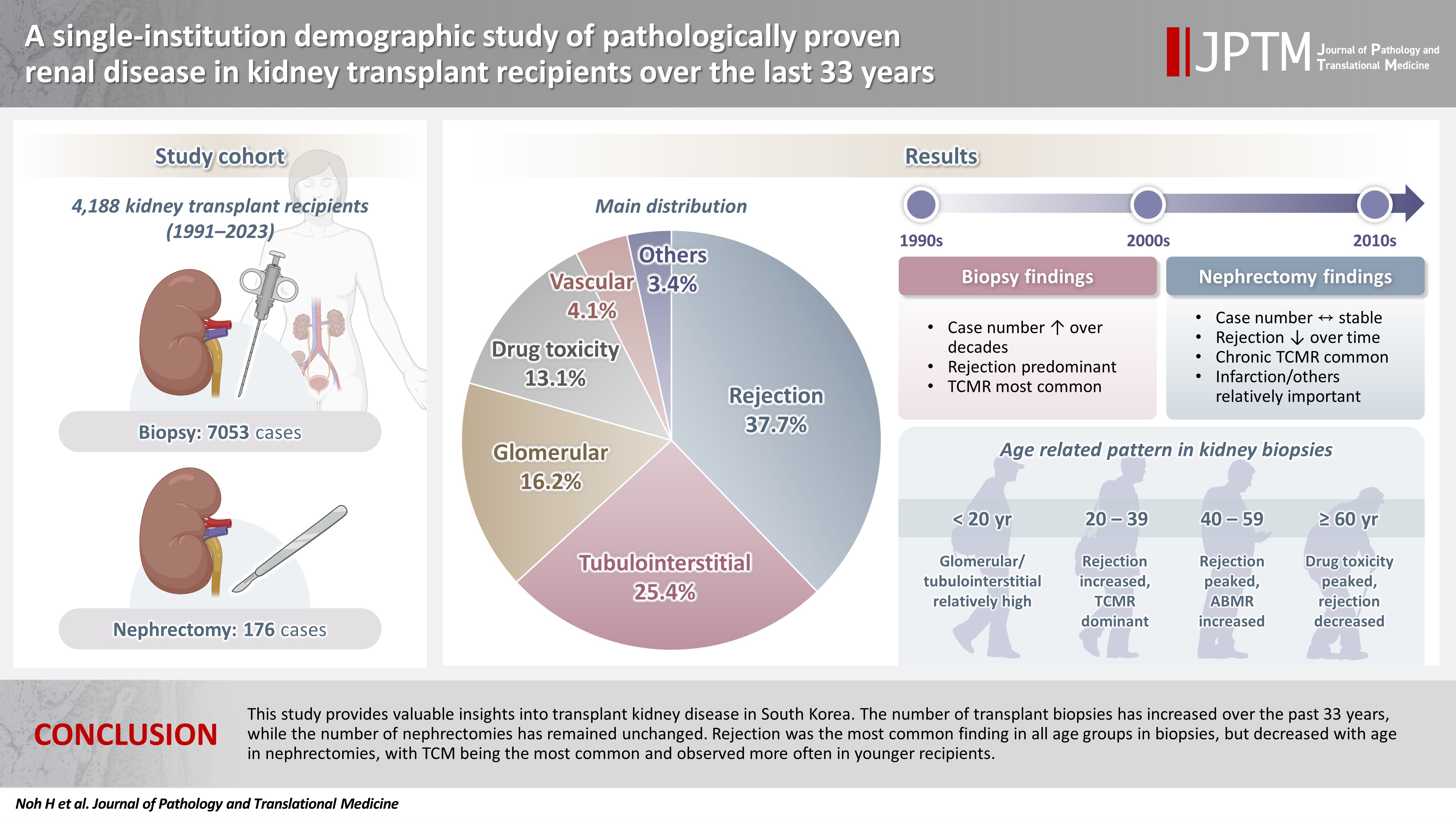
While the number of kidney transplants for end-stage renal disease (ESRD) is increasing, studies examining the long-term demographic analyses based on pathological diagnosis of transplant kidney remain limited. Methods: We conducted a retrospective analysis of 4,188 transplant recipients who underwent either biopsy or nephrectomy from 1991 to 2023 at Seoul St. Mary’s Hospital. Results: Among 7,229 pathologically confirmed cases, rejection was the most prevalent (37.7%), followed by tubulointerstitial (25.4%), glomerular, drug toxicity, and vascular diseases. In 7,053 transplant biopsies, rejection was predominant across all age groups, with T-cell mediated (TCM) category being the most common (60.1%), followed by antibody-mediated and mixed. Drug toxicity increased with age (p = .047), while glomerular and tubulointerstitial diseases were highest in recipients under 20 (p < .001). Among glomerular diseases, IgA-related glomerulonephritis (45.2%) was the most common. In 176 transplant nephrectomies, the most common diagnosis was rejection (33.5%), followed by renal infarction (19.9%), tubulointerstitial, vascular, glomerular disease, and drug toxicity. “Others” included infarction, ESRD, and lymphangiectasia, which increased with age (p = .011). In nephrectomy cases, rejection decreased over time, with chronic TCM rejection (40.7%) being the most frequent. Conclusions: This study provides valuable insights into transplant kidney disease in South Korea. The number of transplant biopsies has increased over the past 33 years, while the number of nephrectomies has remained unchanged. Rejection was the most common finding in all age groups in biopsies, but decreased with age in nephrectomies, with TCM being the most common and observed more often in younger recipients.
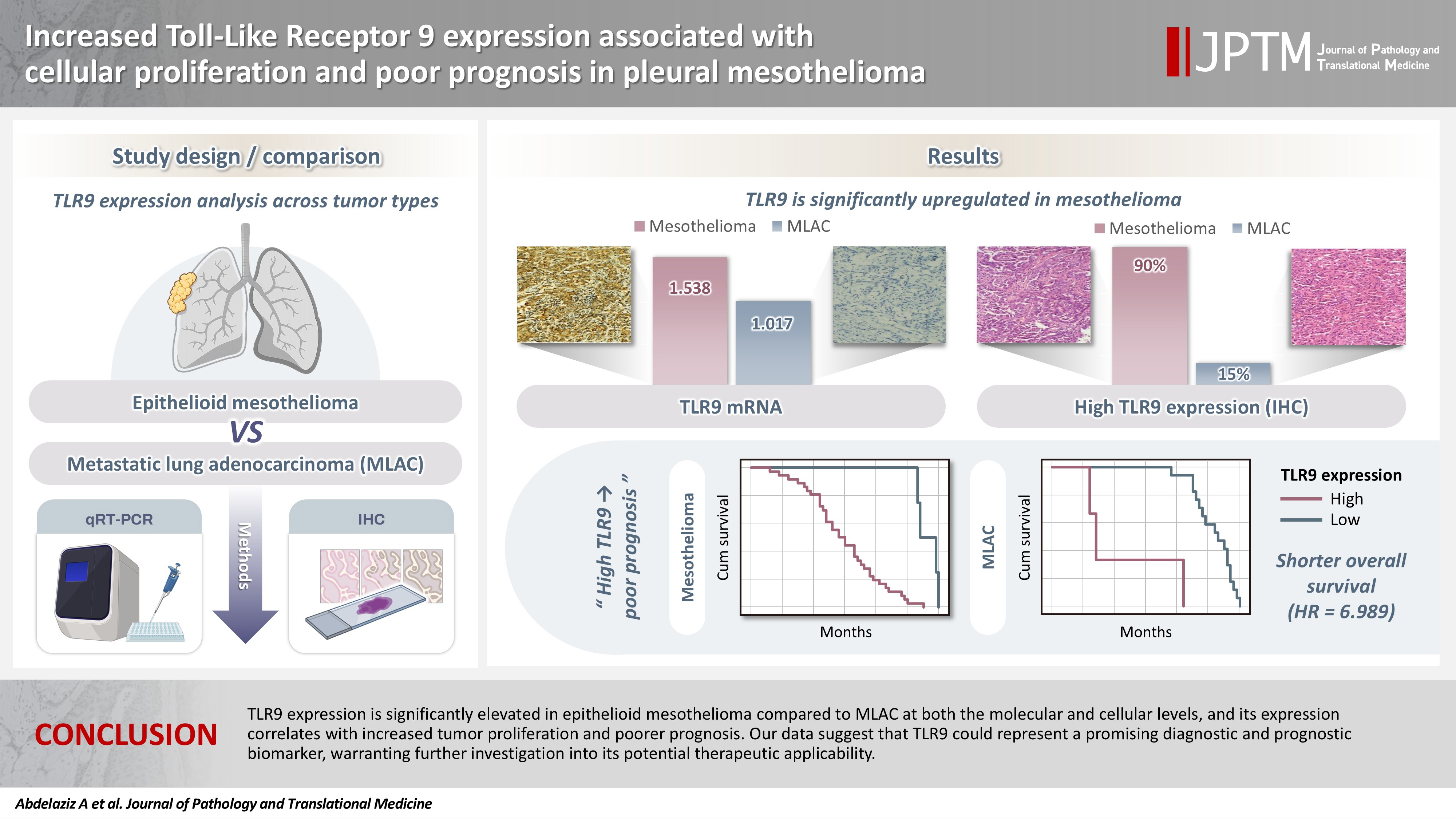
- Increased Toll-like receptor 9 expression associated with cellular proliferation and poor prognosis in pleural mesothelioma
- Ali Omar Abdelaziz, Dina Moustafa Thabit, Rehab Mohamed Kamal, Hend Moness, Rasha Fouad Ahmed, Mariana Fathy Gayyed, Fatma El Zahraa Ammar Mohamed
- J Pathol Transl Med. 2026;60(4):413-421. Published online May 26, 2026
- DOI: https://doi.org/10.4132/jptm.2026.04.01
- 1,040 View
- 24 Download
-
Abstract
PDFSupplementary Material
- Background
Pleural mesothelioma is an aggressive malignancy with a poor prognosis. The epithelioid subtype is the most common and can be challenging to distinguish from metastatic lung adenocarcinoma (MLAC). The role of Toll-like receptor 9 (TLR9) in the progression of pleural mesothelioma remains unclear. Methods: A total of 30 pleural biopsy specimens were collected, comprising 10 cases of pleural epithelioid mesothelioma and 20 cases of MLAC. The mRNA expression levels of TLR9 and proliferating cell nuclear antigen (PCNA) were quantified. In addition, sixty archived formalin-fixed, paraffin-embedded tissue blocks (40 epithelioid mesothelioma and 20 MLAC) were analyzed via immunohistochemistry using an anti-TLR9 antibody in relation to various clinicopathological parameters. Results: TLR9 expression was significantly higher in epithelioid mesothelioma cases than in MLAC cases (p < .001), with mean values of 1.54 ± 0.09 and 1.02 ± 0.08, respectively. A significant positive correlation was observed between TLR9 and PCNA expression levels specifically in the epithelioid mesothelioma cohort (p < .001, r = 0.8). Furthermore, immunohistochemical analysis confirmed that high TLR9 immunoexpression was significantly more prevalent in epithelioid mesothelioma (36/40 cases; 90%) than in MLAC (3/20 cases; 15%) (p < .001). Notably, elevated TLR9 expression was associated with a significantly shorter overall survival (p = .001). Conclusions: In conclusion, TLR9 expression is significantly elevated in epithelioid mesothelioma compared to MLAC at both the molecular and cellular levels, and its expression correlates with increased tumor proliferation and poorer prognosis. Our data suggest that TLR9 could represent a promising diagnostic and prognostic biomarker, warranting further investigation into its potential therapeutic applicability.
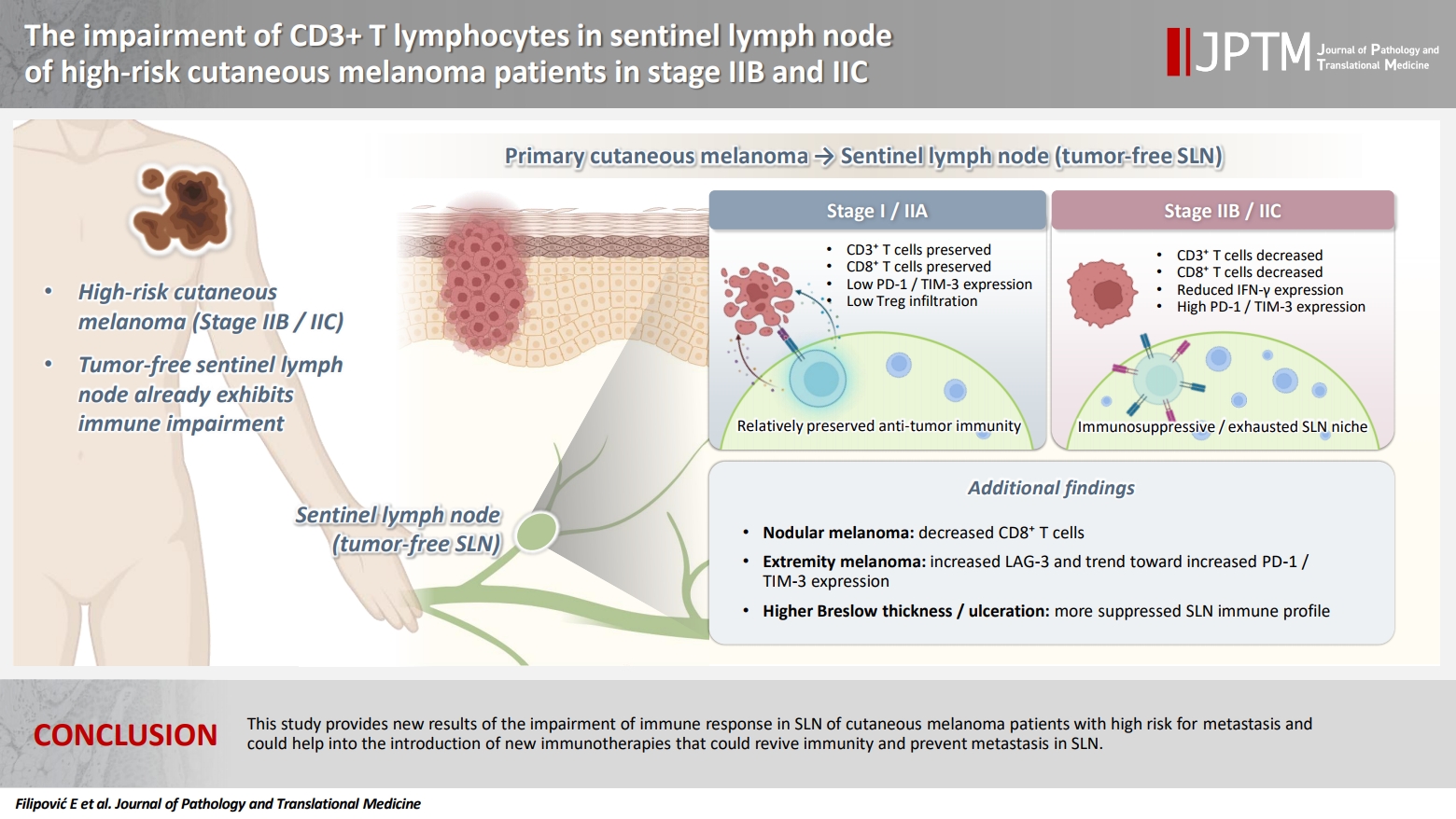
- The impairment of CD3+ T lymphocytes in sentinel lymph node of high-risk cutaneous melanoma patients in stage IIB and IIC
- Emilija Filipović, Katarina Mirjačić Martinović, Ognjen Živković, Nataša Medić Milijić, Ana Lazarević, Zoran Bukumirić, Marko Jevrić, Milan Žegarac
- J Pathol Transl Med. 2026;60(4):422-435. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.04.02
- 554 View
- 17 Download
-
Abstract
PDF
- Background
The sentinel lymph node (SLN) in melanoma is almost always the first site of metastasis and its histopathological assessment is essential for the determination of staging and clinical outcome. Furthermore, this procedure offers the investigation of the early immune response in SLN as melanoma-derived factors suppress the immunity in an early stage that may facilitate metastasis. A better understanding of the immunological changes in SLN may help in the therapeutic stimulation of melanoma immunity to prevent tumor metastasis. Methods: SLN tissues without malignant cells from 74 cutaneous melanoma patients (stage I and II) were analyzed. By flow cytometry, we measured the percentage of natural killer cells, CD3+ T lymphocytes, and their expression of interferon-γ (IFN-γ) and inhibitory immune checkpoint molecules (ICMs), and the percentage of CD4+Foxp3+ regulatory T cells (Tregs). Results: Melanoma patients with worse prognosis, in stage IIB–C, had decreased percentage of total CD3+ and CD3+CD8+ T lymphocytes, trend of IFN-γ decrease, increased inhibitory programmed cell death 1 and T cell immunoglobulin and mucin-domain containing 3 ICMs, and higher percentage of Tregs in their SLNs compared with stage I-IIA patients. Furthermore, patients with nodular melanoma had decreased CD3+CD8+ cells compared with patients with superficial spreading melanoma and together with patients with localization of primary tumor on extremities had an increase in the expression of analyzed ICMs. Conclusions: This study provides new results of the impairment of immune response in SLN of cutaneous melanoma patients with high risk for metastasis and could help in the introduction of new immunotherapies that could restore immunity and prevent metastasis in SLN.
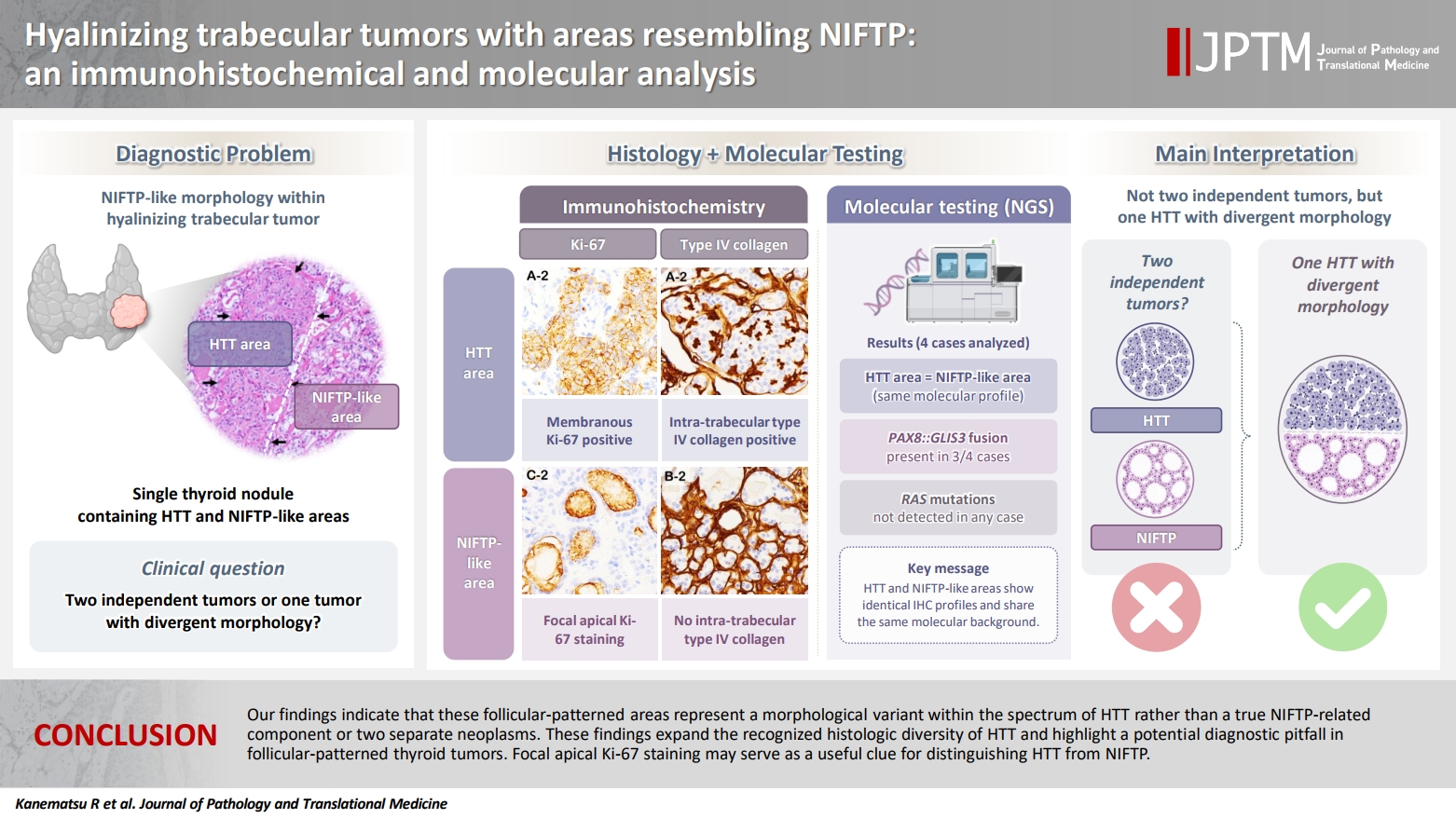
- Hyalinizing trabecular tumors with areas resembling noninvasive follicular thyroid neoplasm with papillary‑like nuclear features: an immunohistochemical and molecular analysis
- Risa Kanematsu, Mitsuyoshi Hirokawa, Ayana Suzuki, Miyoko Higuchi, Satomi Usuki, Hiroshi Kamma, Takashi Akamizu
- J Pathol Transl Med. 2026;60(4):436-443. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.06.07
- 762 View
- 9 Download
-
Abstract
PDF
- Background
The coexistence of hyalinizing trabecular tumor (HTT) and areas with a morphology of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) within a single thyroid nodule has not been previously reported. We aimed to determine whether such tumors represent two independent neoplasms or a single tumor exhibiting divergent morphology. Methods: Ten tumors containing both HTT and NIFTP-like areas were examined. The term “NIFTP-like” was used strictly as a descriptive morphological designation for areas that fulfill the histologic criteria of NIFTP. Immunohistochemical analyses of Ki-67 (MIB-1) and type IV collagen and targeted molecular testing were performed. Ten NIFTPs, 10 follicular adenomas, and three HTTs were used as controls. Results: HTT components consistently showed characteristic membranous Ki-67 staining and intra-trabecular type IV collagen deposition, whereas NIFTP-like areas lacked these features, except for focal apical Ki-67 staining. Intranuclear cytoplasmic inclusions in HTT were positive for type IV collagen. NIFTPs showed neither membranous Ki-67 nor intra-trabecular type IV collagen. Molecular analysis demonstrated identical profiles between HTT components and NIFTP-like areas: three tumors harbored PAX8::GLIS3 fusions, and none showed RAS mutations. Pure HTT controls exhibited the same pattern. Conclusions: Our findings indicate that these follicular-patterned areas represent a morphological variant within the spectrum of HTT rather than a true NIFTP-related component or two separate neoplasms. These findings expand the recognized histologic diversity of HTT and highlight a potential diagnostic pitfall in follicular-patterned thyroid tumors. Focal apical Ki-67 staining may serve as a useful clue for distinguishing HTT from NIFTP.
Case Studies
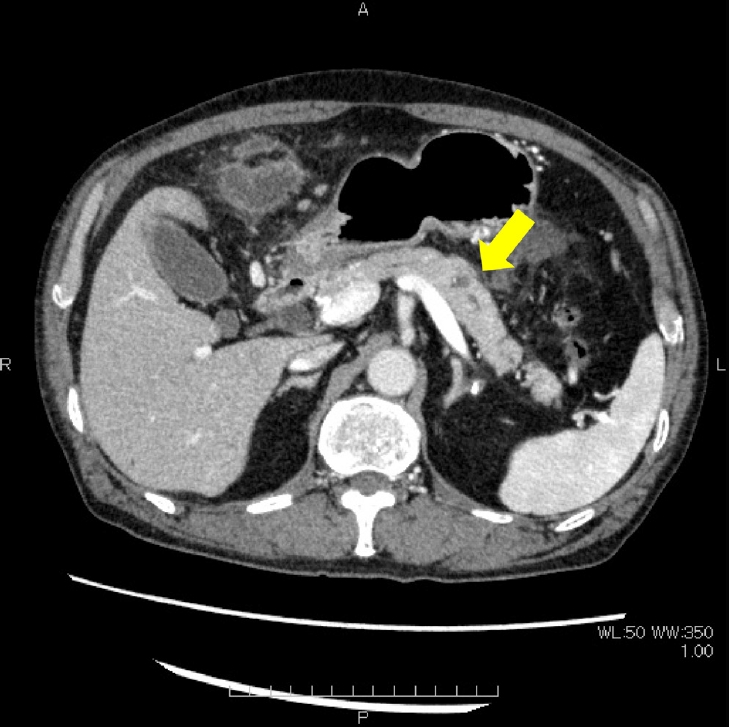
- Non-keratinizing immature squamous metaplasia in the pancreas mimicking malignancy: a diagnostic pitfall in cytology
- Hiroko Hayashi, Tomoaki Kubo, Takuya Hara, Saeko Jinnai, Keisuke Iwasaki
- J Pathol Transl Med. 2026;60(4):444-450. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.02.19
- 489 View
- 14 Download
-
Abstract
PDF
- This report describes a challenging case in which atypical immature squamous metaplasia was misinterpreted as malignancy. A 69-year-old man presented with abdominal pain and loss of appetite. Imaging revealed mild pancreatic duct dilation, parenchymal enlargement, and increased fat attenuation in the transverse mesocolon. Endoscopic ultrasound revealed a hypoechoic lesion in the pancreatic body. The serum amylase level was markedly elevated (1,785 U/L), consistent with acute pancreatitis. Repeated pancreatic juice cytology examinations demonstrated atypical epithelial clusters, which raised concerns about possible pancreatic ductal adenocarcinoma. Therefore, distal pancreatectomy with splenectomy and transverse colon resection were performed. However, histopathological examination revealed only atypical immature squamous metaplasia. Retrospective review of the cytological specimens showed overlapping cell clusters with coarse chromatin, prominent nucleoli, nuclear pleomorphism, and peripheral dissociation in a neutrophilic background with focal hemorrhagic necrosis. Although rarely encountered, squamous metaplastic cells can appear in pancreatic cytology and represent a potential pitfall by mimicking adenocarcinoma.
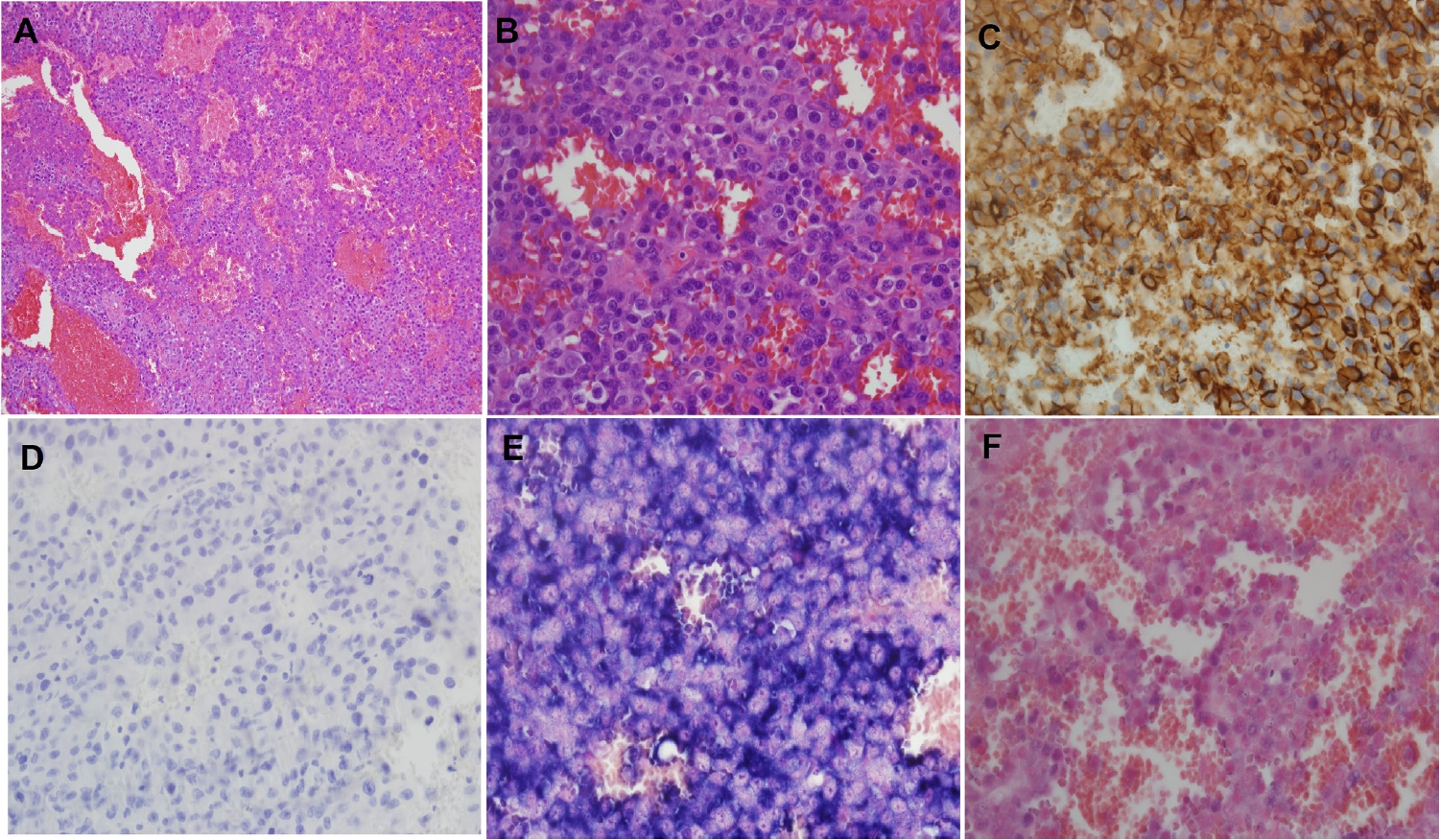
- Phenotypic plasticity in plasma cell myeloma: a CD138-negative case with a rare BRAF G469R mutation
- Sun-Ju Oh, So-Hak Chung
- J Pathol Transl Med. 2026;60(4):451-455. Published online April 22, 2026
- DOI: https://doi.org/10.4132/jptm.2026.02.02
- 1,561 View
- 65 Download
-
Abstract
PDF
- CD138-negative plasma cell myeloma harboring a BRAF G469R mutation is described in a 76-year-old male presenting with multiple osteolytic lesions. Histologically, the lesion exhibited epithelioid to plasmacytoid morphology with prominent mitotic activity and vascular-like spaces. Immunophenotyping demonstrated strong vimentin and CD31 expression but absence of CD138 and other endothelial markers. Light-chain in situ hybridization confirmed a clonal κ-restricted plasma cell population. Bone marrow examination revealed near-complete replacement by atypical plasma cells, retaining CD138 negativity and demonstrating focal CD20 positivity, indicative of intratumoral heterogeneity. Next-generation sequencing identified a rare BRAF G469R variant. The patient exhibited poor response to bortezomib, lenalidomide, and dexamethasone therapy, necessitating a switch to carfilzomib-based treatment. This case underscores the diagnostic challenges of CD138-negative myeloma and highlights the importance of integrating morphology, immunophenotyping, and molecular profiling to inform accurate diagnosis and guide therapeutic strategies.
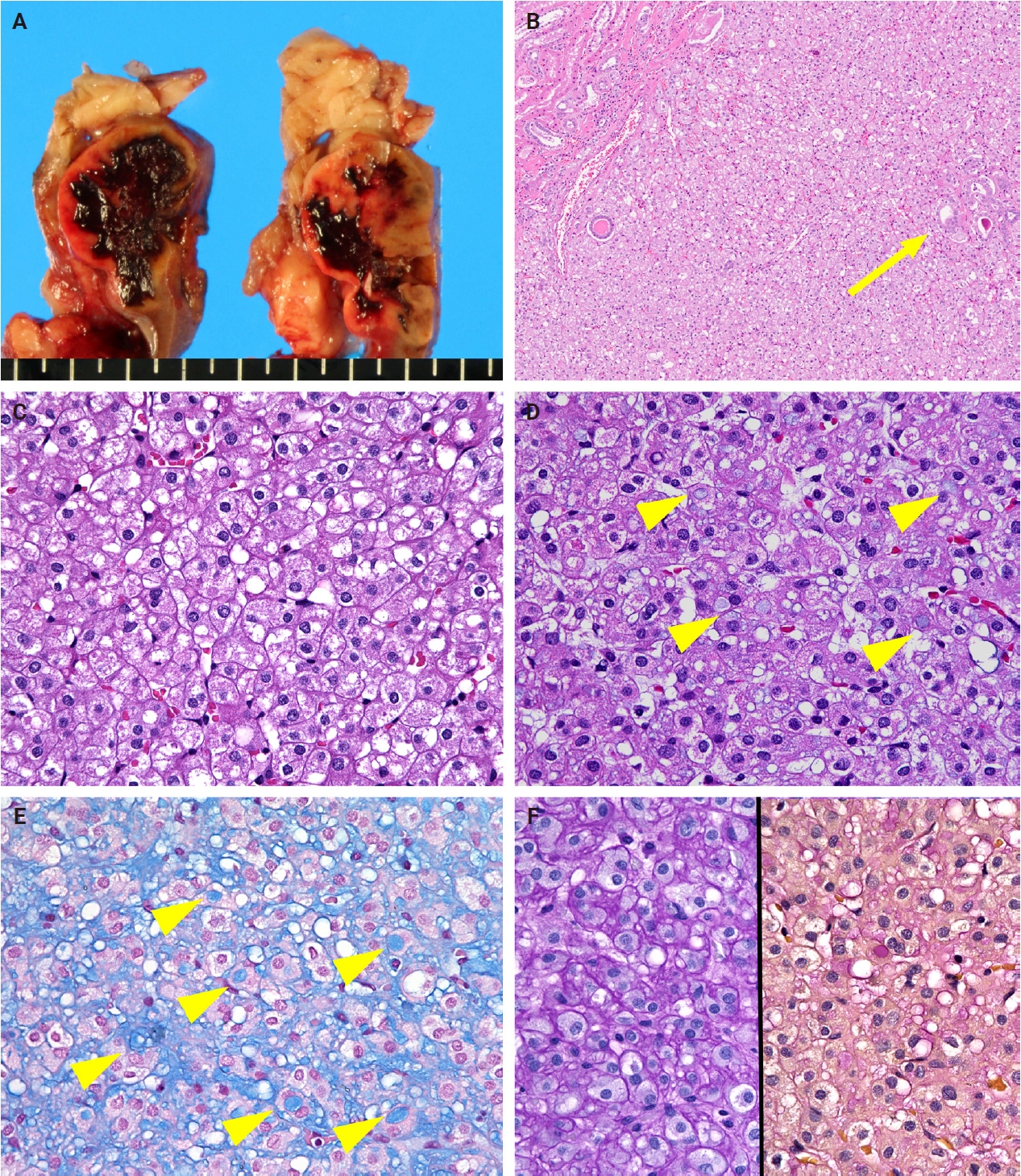
- SDH-deficient renal cell carcinoma with intracytoplasmic mucinous material: a case report and literature review
- Ryosuke Yoshioka, Kosuke Miyai, Kimi Kato, Keiichi Ito, Kimiya Sato, Susumu Matsukuma
- J Pathol Transl Med. 2026;60(4):456-461. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.04.23
- 566 View
- 16 Download
-
Abstract
PDF
- Succinate dehydrogenase (SDH)–deficient renal cell carcinoma (RCC) is a rare, molecularly defined neoplasm. We report a 45-year-old man with a right renal mass treated by nephrectomy. Grossly, a 38-mm gray-white-to-brown solid cystic tumor was observed in the lower pole of the kidney. Microscopically, the tumor consisted of sheets and nested proliferation of eosinophilic cells with low-grade nuclei and bubbly or flocculent cytoplasm. No sarcomatoid or rhabdoid features were observed. Abundant extracellular and focal intracytoplasmic mucinous material was observed in the tumor, which was positive for Alcian blue and mucicarmine staining, but negative for periodic acid–Schiff staining. Immunohistochemistry showed complete loss of succinate dehydrogenase subunit B in tumor cells. These findings supported the diagnosis of RCC consistent with SDH-deficient RCC. This case expands the morphological spectrum of SDH-deficient RCC and highlights the diagnostic pitfalls of renal tumors with mucinous material.
 First
First Prev
Prev


