E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 59(6); 2025 > Article
-
Case Study
Diagnostic challenge in Burkitt lymphoma of the mandible initially misdiagnosed as osteomyelitis: a case report -
Jiwon Do1,2
 , Jin-Young Choi1,2
, Jin-Young Choi1,2 -
Journal of Pathology and Translational Medicine 2025;59(6):460-466.
DOI: https://doi.org/10.4132/jptm.2025.09.18
Published online: November 14, 2025
1Department of Oral and Maxillofacial Surgery, Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
2Department of Oral and Maxillofacial Surgery, Seoul National University Dental Hospital, Seoul, Korea
- Corresponding Author Jin-Young Choi, DDS, MD, Department of Oral and Maxillofacial Surgery, School of Dentistry and Dental Research Institute, Seoul National University, 101 Daehak-ro, Jongno-gu, Seoul 03080, Korea Tel: +82-2-6256-3129, Fax: +82-2-6256-3110, E-mail: jinychoi@snu.ac.kr
© The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,567 Views
- 114 Download
Abstract
- Burkitt lymphoma (BL) is a highly aggressive B-cell neoplasm that rarely involves the mandible in elderly without apparent immunodeficiency. We report a case of a 72-year-old male who presented with persistent mandibular pain following extraction of tooth #46. Initial imaging findings were consistent with incipient osteomyelitis, and the patient was treated with antibiotics. Despite treatment, pain persisted, and follow-up imaging revealed swelling and diffusion restriction in the lateral pterygoid muscle without evidence of a distinct mass. Biopsy revealed BL confirmed by immunohistochemistry: CD10+, BCL6+, c-MYC+, Ki-67 >95%, and negative for BCL2, MUM-1, and Epstein-Barr virus. Although c-MYC immunopositivity was demonstrated, fluorescence in situ hybridization for rearrangement could not be performed due to limited tissue, representing a diagnostic limitation. Notably, the patient had no trismus despite deep muscle involvement, but complained of facial paresthesia and showed remote swelling in the scapular area during hospitalization. Systemic staging with imaging, cerebrospinal fluid cytology, and imaging revealed disseminated nodal and extranodal involvement including the central nervous system, corresponding to stage IV disease by Lugano classification. This case highlights the diagnostic challenge of distinguishing lymphoma from osteomyelitis and underscores the importance of considering malignancy in cases of refractory mandibular inflammation with atypical features.
- Burkitt lymphoma (BL) is an aggressive B-cell non-Hodgkin lymphoma characterized by a high proliferative index and frequent MYC gene rearrangements [1-5]. While the disease most commonly involves abdominal organs such as the ileocecal region and mesentery, extramedullary involvement of the head and neck region may occur, particularly in immunocompromised individuals or in endemic forms [1,5,6]. Although up to 10%–15% of BL cases show head and neck involvement [7], sporadic BL involving the mandible in elderly patients remains exceedingly rare [8] and poses a significant diagnostic challenge. Mandibular BL is often radiographically and clinically indistinguishable from chronic osteomyelitis or odontogenic infections, particularly in the absence of overt mass formation or systemic symptoms, leading to potential diagnostic delay.
- Here, we report a rare case of sporadic, Epstein-Barr virus (EBV)–negative BL involving the right mandible in a 72-year-old patient who presented with persistent mandibular pain and was initially diagnosed and treated as osteomyelitis. The disease progressed despite appropriate antimicrobial therapy, and the correct diagnosis was ultimately confirmed by biopsy and immunohistochemical analysis. This case highlights the need for heightened suspicion of malignancy when clinical and radiographic findings are atypical or refractory to conventional treatment.
INTRODUCTION
- A 72-year-old man presented with persistent pain in the right mandibular molar region. He initially underwent root canal treatment of mandibular right first molar (#46, FDI system) at a local dental clinic; however, symptoms persisted, ultimately necessitating extraction of the involved tooth. Despite this, his discomfort continued, prompting referral to our institution for further evaluation. The patient was otherwise in good general health, with no history of immunodeficiency, and had only well-controlled hypertension and hyperlipidemia.
- Initial panoramic view and non-contrast computed tomography (CT) of the mandible showed thickening of the lamina dura and irregular residual alveolar crest at the #46 extraction site (Fig. 1). Based on the clinical presentation and radiologic findings, the patient was diagnosed with incipient osteomyelitis of the right mandibular body, and oral antibiotic therapy was initiated.
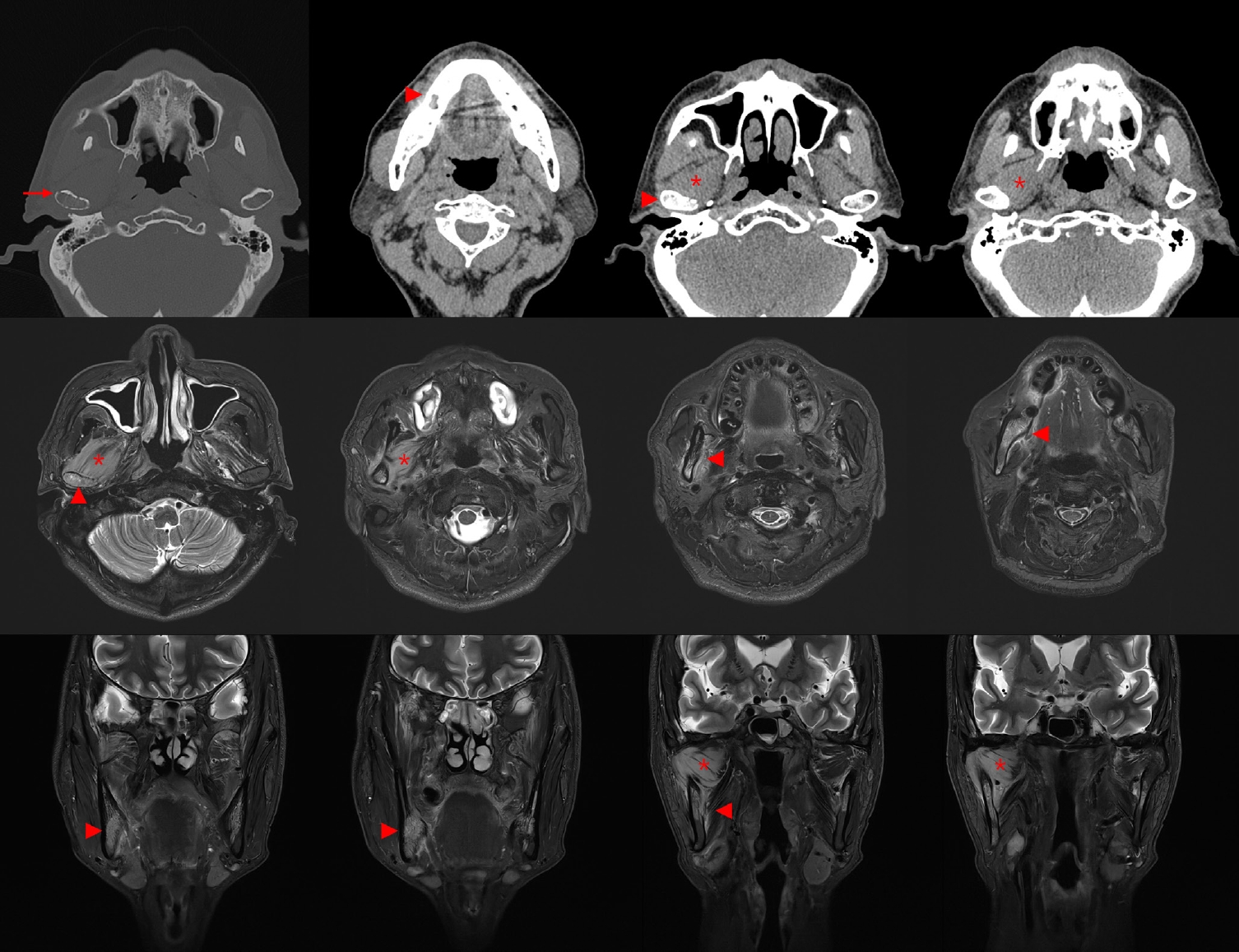
- One month later, follow-up CT revealed cortical erosion of the right mandibular condyle, increased bone marrow attenuation, and swelling of the right lateral pterygoid muscle. Magnetic resonance imaging further showed diffuse hyperintensity of the mandibular body marrow and perimandibular soft tissues on T2-weighted images, with extension to the mandibular foramen and condyle. Marked swelling and diffusion restriction of the lateral pterygoid muscle were also noted, suggestive of progressive inflammation (Fig. 2).
- Histopathologic examination of the mandibular biopsy demonstrated diffuse infiltration of medium-sized atypical lymphoid cells with round nuclei, fine chromatin, and frequent mitotic figures. Immunohistochemically, the neoplastic cells were diffusely positive for CD10, BCL6, and c-MYC (homogeneously >90%), with nearly 100% Ki-67 proliferation index. They were negative for BCL2, MUM-1, and EBV. Focal cytoplasmic positivity for CD3 was observed but, in the absence of other T-cell markers, was regarded as nonspecific (Fig. 3).
- Subsequent systemic work-up revealed widespread disease. Fluorodeoxyglucose positron emission tomography (FDG-PET) demonstrated probable lymphoma involvement of lymph nodes above and below the diaphragm, bones, nasopharynx, tonsil, stomach, subcutaneous tissue and muscles, and lung (Fig. 4A). Cerebrospinal fluid cytospin was positive for malignant lymphoid cells, confirming central nervous system dissemination. In addition, orbit and head CT revealed a suspicious expansile soft tissue lesion in the right ethmoid sinus, together with mild bilateral maxillary sinus mucosal thickening.
- Collectively, these findings were diagnostic of BL. Systemic staging with FDG-PET, cerebrospinal fluid cytology, and CT imaging revealed disseminated nodal and extranodal involvement including the central nervous system, corresponding to stage IV disease by Lugano classification. Given the widespread disease and central nervous system involvement, the therapeutic approach was palliative rather than curative. The patient presented with B symptoms, including weight loss and febrile sense, and was initiated on systemic chemotherapy with R-EPOCH (rituximab, etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin). Intrathecal methotrexate (IT-MTX) was administered for central nervous system prophylaxis and treatment, and he is currently undergoing the fourth cycle of R-EPOCH with IT-MTX. Thus far, the patient has tolerated therapy well without treatment-related complications, and follow-up imaging demonstrated marked improvement of the lesions (Fig. 4B).
CASE REPORT
- BL is an aggressive B-cell neoplasm with distinct epidemiologic variants. Endemic BL, strongly associated with EBV, typically presents in the jaw and facial bones of children, whereas sporadic BL more commonly involves intra-abdominal organs in younger patients [1-5]. Jaw involvement in elderly individuals without apparent immunodeficiency is rare, and very few cases of sporadic, EBV-negative BL of the mandible have been reported in this age group [8-12].
- In the present case, the initial clinical and radiologic findings closely resembled osteomyelitis. Osteomyelitis of the jaw is typically characterized by localized pain, sclerosis of trabecular bone, periosteal reaction, sequestrum formation, and sinus tract development [13,14]. In contrast, malignant bone lesions—including primary bone lymphomas—more often demonstrate rapidly progressive, ill-defined osteolysis, cortical destruction, and associated soft tissue masses [15]. Our patient initially showed lamina dura thickening and subtle marrow signal change, mimicking early infection, but atypical features emerged over time. These included persistent inflammatory marker elevation despite antibiotics, perineural symptoms such as facial paresthesia, and deep muscle involvement without abscess or trismus, all of which raised suspicion for malignancy.
- When lymphoma involves the maxillofacial skeleton, imaging often reveals diffuse marrow replacement, cortical thinning or destruction, and soft tissue extension without abscess formation [16,17]. Reports have shown that such presentations are frequently mistaken for odontogenic infection or osteomyelitis, leading to delayed diagnosis [11,18,19]. This case underscores the diagnostic dilemma posed by primary bone lymphomas mimicking inflammatory disease and emphasizes the importance of early biopsy when conventional treatment fails.
- In the present case, the differential diagnosis included diffuse large B-cell lymphoma (DLBCL), high-grade B-cell lymphoma (HGBCL), and BL. DLBCL was considered less likely because the tumor cells in our case were morphologically monotonous and of medium size, lacking the pleomorphism typically seen in DLBCL. Moreover, the proliferation index approached 100%, which is unusually high for DLBCL. HGBCL, particularly the double-hit or triple-hit subtype, may resemble BL; however, these entities generally harbor MYC rearrangements in combination with BCL2 and/or BCL6 translocations. In contrast, our case showed the classic immunophenotypic profile of BL, with diffuse CD10, and BCL6 positivity, nearly 100% Ki-67, and negativity for BCL2 and MUM-1. Although molecular confirmation of MYC rearrangement could not be performed due to limited tissue, the combination of morphology, immunophenotype, and clinical presentation was most consistent with BL rather than DLBCL or HGBCL [6,20-22].
- This study has limitations. The biopsy specimen was obtained by curettage at the dental hospital, and the slides were subsequently referred to the medical hospital for diagnostic consultation. Because only limited tissue was available and evaluation relied on a restricted number of slides, additional molecular studies such as fluorescence in situ hybridization for MYC rearrangement could not be performed. Furthermore, as the patient has already initiated systemic chemotherapy, retrospective molecular testing is not feasible. Although the morphology and immunophenotypic profile were highly characteristic of BL, the absence of molecular confirmation represents a diagnostic limitation.
- In conclusion, this case illustrates the diagnostic challenge of distinguishing BL from osteomyelitis in the mandible of an elderly patient. Subtle radiographic changes, lack of a distinct mass, and initial resemblance to infection delayed recognition of the malignancy. However, persistent symptoms, rising inflammatory markers despite antibiotics, and atypical features such as perineural involvement should prompt early biopsy to exclude lymphoma. Clinicians should maintain a broad differential diagnosis for refractory mandibular inflammatory lesions, as timely recognition of BL is essential for initiating appropriate therapy in this aggressive disease.
DISCUSSION
Ethics Statement
Formal written informed consent was not required with a waiver by the Institutional Review Board of Seoul National University Dental Hospital (IRB No. ERI25038).
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author Contributions
Conceptualization: JYC. Investigation: JD. Writing—original draft: JD. Writing—review & editing: JD, JYC. Supervision: JYC. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.




- 1. Lopez C, Burkhardt B, Chan JK, et al. Burkitt lymphoma. Nat Rev Dis Primers 2022; 8: 78.ArticlePubMed
- 2. Dalla-Favera R, Bregni M, Erikson J, Patterson D, Gallo RC, Croce CM. Human c-myc onc gene is located on the region of chromosome 8 that is translocated in Burkitt lymphoma cells. Proc Natl Acad Sci U S A 1982; 79: 7824-7. ArticlePubMedPMC
- 3. Boerma EG, Siebert R, Kluin PM, Baudis M. Translocations involving 8q24 in Burkitt lymphoma and other malignant lymphomas: a historical review of cytogenetics in the light of todays knowledge. Leukemia 2009; 23: 225-34. ArticlePubMedPDF
- 4. Dalla-Favera R, Lombardi L, Pelicci PG, Lanfrancone L, Cesarman E, Neri A. Mechanism of activation and biological role of the c-myc oncogene in B-cell lymphomagenesis. Ann N Y Acad Sci 1987; 511: 207-18. ArticlePubMed
- 5. Molyneux EM, Rochford R, Griffin B, et al. Burkitt's lymphoma. Lancet 2012; 379: 1234-44. ArticlePubMed
- 6. Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia 2022; 36: 1720-48. ArticlePubMedPMC
- 7. Kuo CY, Shih CP, Cheng LH, et al. Head and neck lymphomas: review of 151 cases. J Med Sci 2020; 40: 215-23. Article
- 8. Dunleavy K, Little RF, Wilson WH. Update on Burkitt lymphoma. Hematol Oncol Clin North Am 2016; 30: 1333-43. ArticlePubMed
- 9. Munekata T, Asaka T, Sakata KI, et al. Challenging differentiation of oral malignant lymphoma from osteomyelitis of the jawbone: a case report. Mol Clin Oncol 2025; 22: 54.ArticlePubMedPMC
- 10. Bugshan A, Kassolis J, Basile J. Primary diffuse large B-cell lymphoma of the mandible: case report and review of the literature. Case Rep Oncol 2015; 8: 451-5. ArticlePubMedPMCPDF
- 11. Adalja D, Tagliaferri A, Rezkalla A, Taha B. Diffuse B-cell lymphoma of the mandible disguised as acute osteomyelitis. Eur J Case Rep Intern Med 2024; 11: 004243.ArticlePubMedPMCPDF
- 12. Kuo YS, Wu YH, Sun A, Chiang CP. Burkitt's lymphoma of the mandible. J Dent Sci 2017; 12: 421-3. ArticlePubMedPMC
- 13. Baur DA, Altay MA, Flores-Hidalgo A, Ort Y, Quereshy FA. Chronic osteomyelitis of the mandible: diagnosis and management: an institution's experience over 7 years. J Oral Maxillofac Surg 2015; 73: 655-65. ArticlePubMed
- 14. Schuknecht B, Valavanis A. Osteomyelitis of the mandible. Neuroimaging Clin N Am 2003; 13: 605-18. ArticlePubMed
- 15. Musbah T, Omami G. Ill-defined lytic mandibular lesion. J Am Dent Assoc 2020; 151: 692-5. ArticlePubMed
- 16. Krishnan A, Shirkhoda A, Tehranzadeh J, Armin AR, Irwin R, Les K. Primary bone lymphoma: radiographic-MR imaging correlation. Radiographics 2003; 23: 1371-83. ArticlePubMed
- 17. Imaizumi A, Kuribayashi A, Watanabe H, et al. Non-Hodgkin lymphoma involving the mandible: imaging findings. Oral Surg Oral Med Oral Pathol Oral Radiol 2012; 113: e33-9. ArticlePubMed
- 18. Catania R, Belloni E, Preda L, Bortolotto C, Scagnelli P, Calliada F. Odontogenic-like pain in partial edentulism: an unusual presentation of diffuse large B-cell lymphoma of the mandible. Indian J Radiol Imaging 2021; 31: 1053-6. ArticlePubMedPMC
- 19. Mika J, Schleicher I, Gerlach U, Adler CP, Uhl M, Knoeller SM. Primary bone lymphomas thought to be osteomyelitis urgently demand a rapid diagnosis in bone pathology. Anticancer Res 2012; 32: 4905-12. PubMed
- 20. Zhao XF, Hassan A, Perry A, Ning Y, Stass SA, Dehner LP. C-MYC rearrangements are frequent in aggressive mature B-Cell lymphoma with atypical morphology. Int J Clin Exp Pathol 2008; 1: 65-74. PubMedPMC
- 21. Harlendea NJ, Harlendo K. Ki-67 as a marker to differentiate Burkitt lymphoma and diffuse large B-cell lymphoma: a literature review. Cureus 2024; 16: e72190.ArticlePubMedPMC
- 22. Scott DW, King RL, Staiger AM, et al. High-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements with diffuse large B-cell lymphoma morphology. Blood 2018; 131: 2060-4. ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-