 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(6); 2014 > Article
-
Brief Case Report
Lymphoepithelioma-like Carcinoma of the Renal Pelvis: A Case Report and Review of the Literature - Hyein Ahn, Jongmin Sim, Hyunsung Kim, Kijong Yi, Hulin Han, Yumin Chung, Abdul Rehman, Seung Sam Paik
-
Korean Journal of Pathology 2014;48(6):458-461.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.6.458
Published online: December 31, 2014
Department of Pathology, Hanyang University College of Medicine, Seoul, Korea
- Corresponding Author: Seung Sam Paik, M.D. Department of Pathology, Hanyang University College of Medicine, 222 Wangsimni-ro, Seongdong-gu, Seoul 133-791, Korea Tel: +82-2-2290-8252, Fax: +82-2-2296-7502, E-mail: sspaik@hanyang.ac.kr
• Received: May 7, 2014 • Revised: June 2, 2014 • Accepted: June 17, 2014
© The Korean Society of Medical Education. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
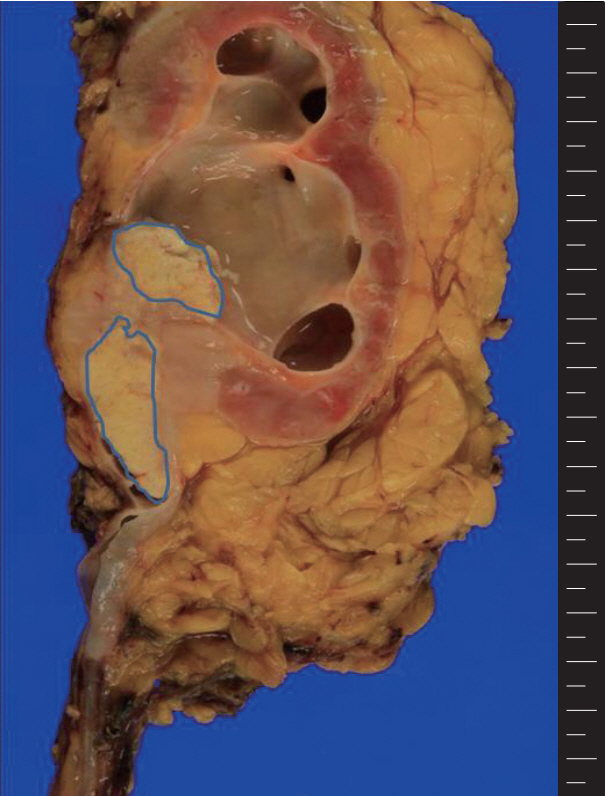
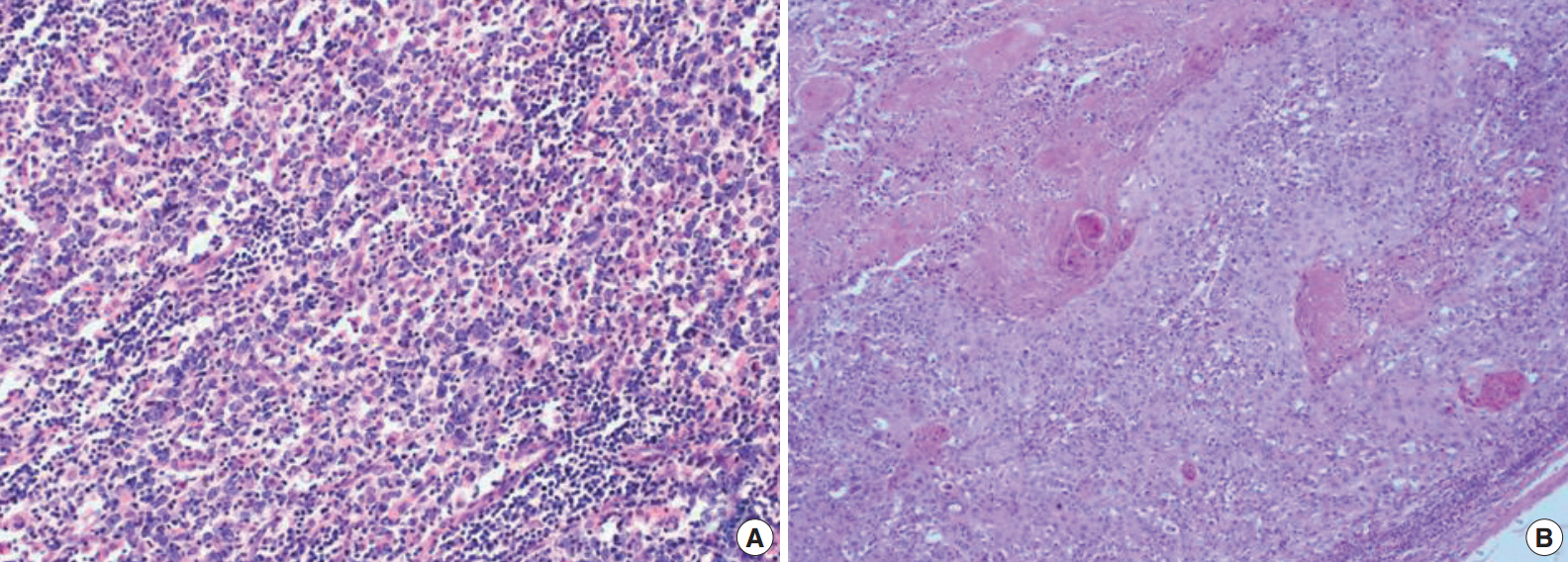
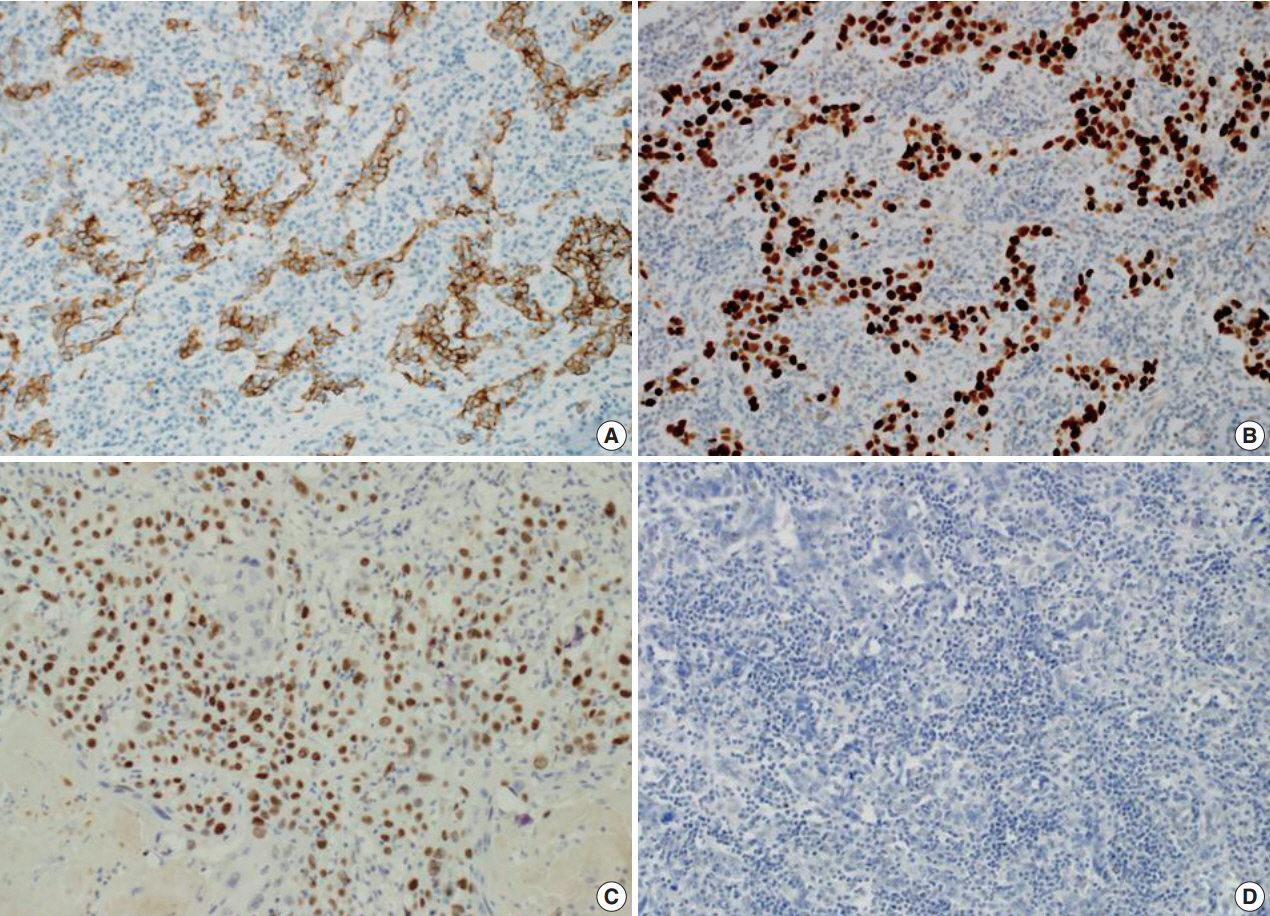
Figure & Data
References
Citations
Citations to this article as recorded by 
- Analysis of genetic profiling, pathomics signature, and prognostic features of primary lymphoepithelioma‐like carcinoma of the renal pelvis
Bo Fan, Yuanbin Huang, Hongshuo Zhang, Tingyu Chen, Shenghua Tao, Xiaogang Wang, Shuang Wen, Honglong Wang, Zhe Lin, Tianqing Liu, Hongxian Zhang, Tao He, Xiancheng Li
Molecular Oncology.2022; 16(20): 3666. CrossRef - Lymphoepithelioma-like carcinoma of the upper urinary tract: A systematic review of case reports
Shi-Cong Lai, Samuel Seery, Wei Zhang, Ming Liu, Guan Zhang, Jian-Ye Wang
World Journal of Clinical Cases.2020; 8(4): 771. CrossRef - Rare primary lymphoepithelioma-like carcinoma of the renal pelvis
Shi-Cong Lai, Samuel Seery, Tong-Xiang Diao, Jian-Ye Wang, Ming Liu
World Journal of Clinical Cases.2020; 8(9): 1752. CrossRef - Eight-year follow-up of locally advanced lymphoepithelioma-like carcinoma at upper urinary tract: A case report
Che H Yang, Wei C Weng, Yi S Lin, Li H Huang, Chin H Lu, Chao Y Hsu, Yen C Ou, Min C Tung
World Journal of Clinical Cases.2020; 8(19): 4505. CrossRef - Lymphoepithelioma-like, a variant of urothelial carcinoma of the urinary bladder: a case report and systematic review for optimal treatment modality for disease-free survival
Andy W. Yang, Aydin Pooli, Subodh M. Lele, Ina W. Kim, Judson D. Davies, Chad A. LaGrange
BMC Urology.2017;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
- Related articles
-
- Primary Merkel cell carcinoma of the salivary gland: a clinicopathologic study of four cases with a review of literature
- Metastatic choroidal melanoma in the breast: a case report and review of the literature
- Hepatic carcinoma expressing inhibin: case report of a proposed novel entity and review of the literature
Lymphoepithelioma-like Carcinoma of the Renal Pelvis: A Case Report and Review of the Literature



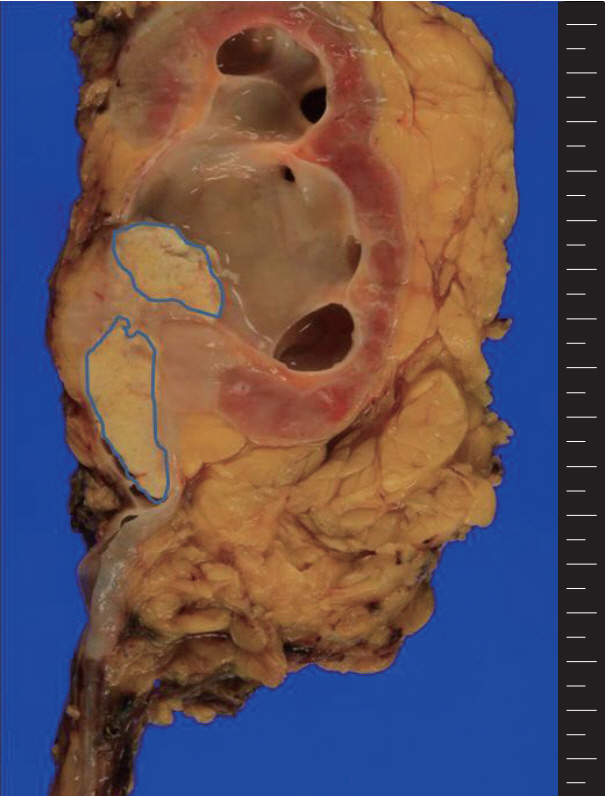
Fig. 1. A grayish white tumor is present in the renal pelvis with extension into the adjacent parenchyma and hilar fat tissue. The central whitish lesion reveals squamous cell carcinoma (blue color) and the peripheral solid portion reveal lymphoepithelioma-like carcinoma.
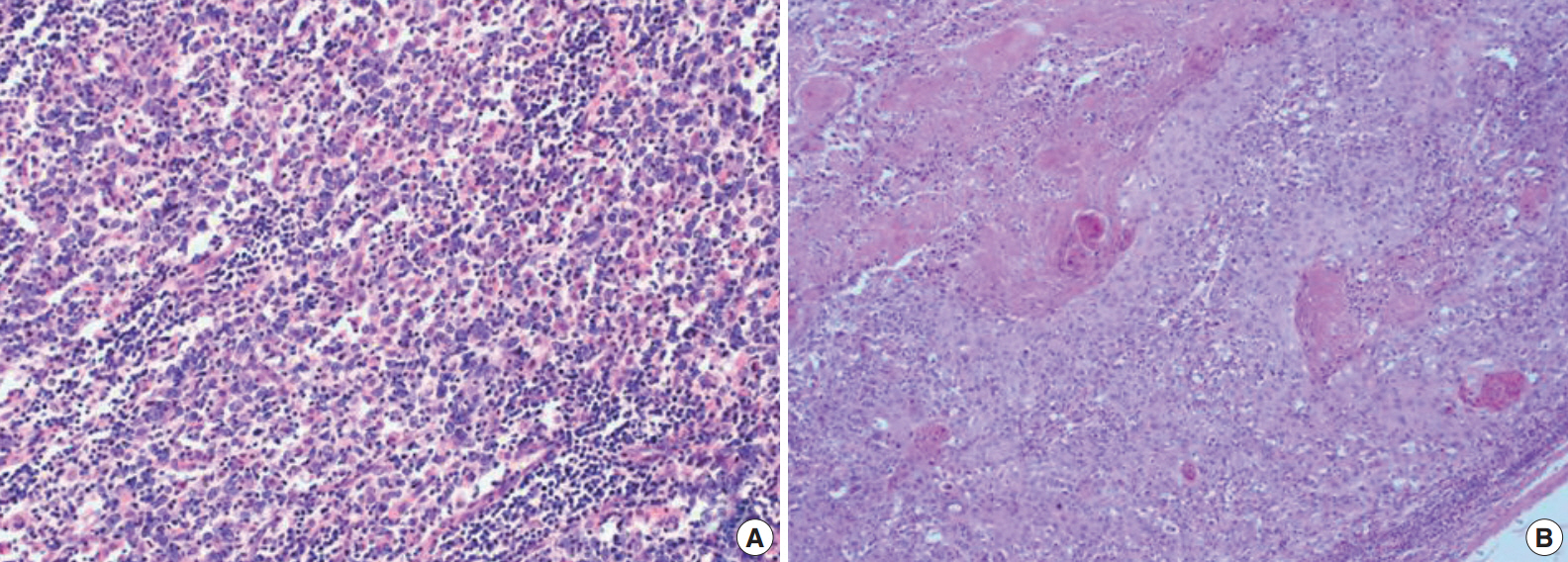
Fig. 2. The tumor shows syncytial clusters of large polygonal tumor cells with a background of dense lymphoid stroma (A) and squamous cell carcinoma component with exuberant keratin formation (B).
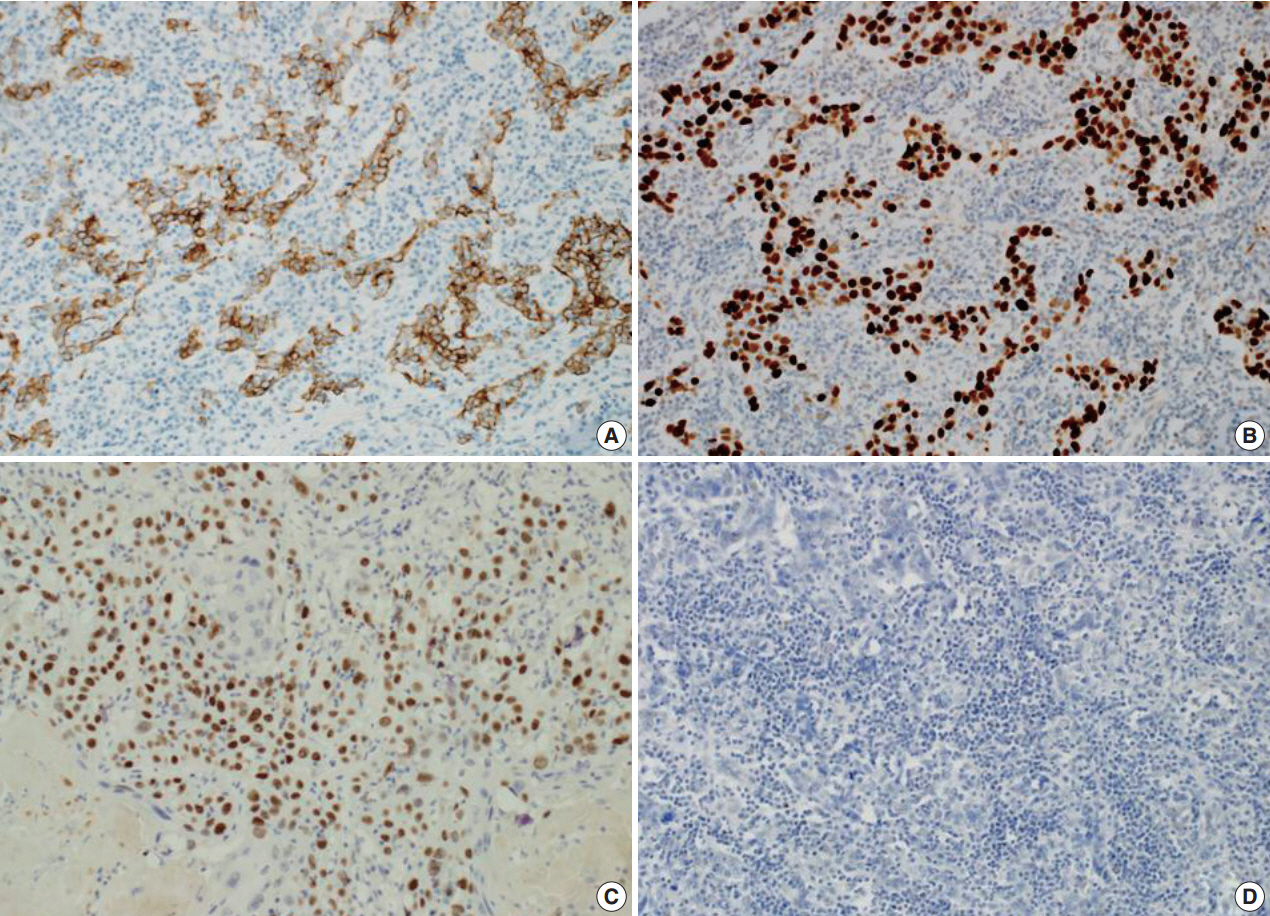
Fig. 3. The tumor cells of lymphoepithelioma-like carcinoma are positive for cytokeratin (A) and p53 (B). The tumor cells of squamous cell carcinoma are positive for p63 (C). The tumor cells of lymphoepithelioma-like carcinoma are negative for Epstein-Barr virus–encoded RNA by in situ hybridization (D).
Fig. 1.
Fig. 2.
Fig. 3.
Lymphoepithelioma-like Carcinoma of the Renal Pelvis: A Case Report and Review of the Literature
| Case No. | Sex/Age (yr) | Symptom | HC | Stage | EBV status | Tx | F/U | Outcome | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 1 | F/75 | Hematuria | Pure | T1N1M0 | Negative | NU | 36 mo | NED | Haga et al. [1] |
| 2 | F/75 | Hematuria | Predominant | T3N1M0 | Not tested | NU | 6 mo | NED | Modi et al. [2] |
| 3 | Unknown | Unknown | Unknown | Unknown | Unknown | Unknown | Unknown | Unknown | Tamas et al. [3] |
| 4 | F/75 | Hematuria | Unknown | T3N0M0 | Negative | RN | 6 mo | NED | Yamada et al. [4] |
| 5 | F/72 | Unknown | Predominant | T3 | Negative | RN | 3 mo | DWD | Perez-Montiel et al. [5] |
| 6 | M/68 | Unknown | Focal | T3 | Negative | RN | 12 mo | DWD | Perez-Montiel et al. [5] |
| 7 | F/79 | Hematuria | Unknown | T3N0M0 | Negative | NU | 6 mo | NED | Cohen et al. [6] |
| 8 | M/70 | Hematuria | Pure | Unknown | Negative | RN+RT | 6 yr | NED | Fukunaga and Ushigome [7] |
| 9 | F/70 | Hematuria | Unknown | T2N0M0 | Negative | NU | 24 mo | NED | Hahm et al. [8] |
| 10 | F/65 | Hematuria | Predominant | T3N0M0 | Negative | RN | 6 mo | NED | Present case |
Table 1. The clinicopathological characteristics of reported lymphoepithelioma-like carcinoma of the renal pelvis
HC, histological classification; EBV, Epstein-Barr virus; Tx, treatment; F/U, follow-up; F, female; NU, nephroureterectomy; NED, no evidence of disease; RN, radical nephrectomy; DWD, died with disease; M, male; RT, radiation therapy.

