 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 57(2); 2023 > Article
-
Original Article
Postmortem lung and heart examination of COVID-19 patients in a case series from Jordan -
Maram Abdaljaleel1,2
 , Isra Tawalbeh3, Malik Sallam1,2,4, Amjad Bani Hani5, Imad M. Al-Abdallat1,2, Baheth Al Omari1,2, Sahar Al-Mustafa1,2, Hasan Abder-Rahman1,2, Adnan Said Abbas3, Mahmoud Zureigat3, Mousa A. Al-Abbadi1,2
, Isra Tawalbeh3, Malik Sallam1,2,4, Amjad Bani Hani5, Imad M. Al-Abdallat1,2, Baheth Al Omari1,2, Sahar Al-Mustafa1,2, Hasan Abder-Rahman1,2, Adnan Said Abbas3, Mahmoud Zureigat3, Mousa A. Al-Abbadi1,2 -
Journal of Pathology and Translational Medicine 2023;57(2):102-112.
DOI: https://doi.org/10.4132/jptm.2023.01.30
Published online: March 14, 2023
1Department of Pathology, Microbiology and Forensic Medicine, School of Medicine, The University of Jordan, Amman, Jordan
2Department of Clinical Laboratories and Forensic Medicine, Jordan University Hospital, Amman, Jordan
3Department of Forensic Pathology, Ministry of Health, Amman, Jordan
4Department of Translational Medicine, Faculty of Medicine, Lund University, Malmö, Sweden
5Department of General Surgery, School of Medicine, The University of Jordan, Amman, Jordan
- Corresponding Author: Malik Sallam, MD, PhD, Department of Clinical Laboratories and Forensic Medicine, Jordan University Hospital, Queen Rania Al-Abdullah Street-Aljubeiha/ P.O. Box 13046, Amman, Jordan Tel: +962-6-5353666 (ext. 2811), E-mail: malik.sallam@ju.edu.jo
© 2023The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 7,809 Views
- 171 Download
- 1 Crossref
Abstract
-
Background
- Coronavirus disease 2019 (COVID-19) has emerged as a pandemic for more than 2 years. Autopsy examination is an invaluable tool to understand the pathogenesis of emerging infections and their consequent mortalities. The aim of the current study was to present the lung and heart pathological findings of COVID-19–positive autopsies performed in Jordan.
-
Methods
- The study involved medicolegal cases, where the cause of death was unclear and autopsy examination was mandated by law. We included the clinical and pathologic findings of routine gross and microscopic examination of cases that were positive for COVID-19 at time of death. Testing for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was confirmed through molecular detection by real-time polymerase chain reaction, serologic testing for IgM and electron microscope examination of lung samples.
-
Results
- Seventeen autopsies were included, with male predominance (76.5%), Jordanians (70.6%), and 50 years as the mean age at time of death. Nine out of 16 cases (56.3%) had co-morbidities, with one case lacking such data. Histologic examination of lung tissue revealed diffuse alveolar damage in 13/17 cases (76.5%), and pulmonary microthrombi in 8/17 cases (47.1%). Microscopic cardiac findings were scarcely detected. Two patients died as a direct result of acute cardiac disease with limited pulmonary findings.
-
Conclusions
- The detection of SARS-CoV-2 in postmortem examination can be an incidental or contributory finding which highlights the value of autopsy examination to determine the exact cause of death in controversial cases.
- Study design
- The current study was based on conducting a serial postmortem examination in COVID-19–positive patients at time of death among medicolegal cases in which autopsies are mandatory by Jordanian law to determine the cause of death. Testing for SARS-CoV-2 for all cases of death was mandatory by law before burial in Jordan. Autopsies were conducted at Jordan University Hospital (JUH) and Zarqa Hospital. Forensic gross assessment was done for specimens from the lungs, heart, among other organs. Postmortem specimens were tested for SARS-CoV-2 by qPCR, serologic testing, or both. The final confirmation of SARS-CoV-2 detection in autopsies was done through examining lung specimens under EM, which was conducted at the Department of Pathology, Microbiology and Forensic Medicine at the School of Medicine, University of Jordan.
- Testing for COVID-19
- The postmortem detection of SARS-CoV-2 was based on three approaches as follows: (1) qPCR of nasopharyngeal swabs, with RNA purification using the automated Zybio Nucleic Acid Isolation System EXM3000 (Zybio, Chongqing, China), with reverse-transcriptase qPCR being done using SARS-CoV-2 Nucleic Acid Detection Kit (Zybio) targeting three genomic regions (Envelope, ORF1ab, and Nucleocapsid) with interpretation according to manufacturer’s instructions; (2) serologic testing to detect IgM/IgG; (3) EM examination of autopsies with lung tissue.
- Initially, all cases were identified through either a positive qPCR testing result or serologic testing, while EM examination was conducted among all cases.
- Autopsy examination
- Autopsies carried out on COVID-19–positive dead bodies were done by authority of the District Attorney since all cases were labeled as medicolegal cases. Such cases are considered medicolegal due to the sudden and unexpected death with no clear causes, with consent to conduct autopsy examination being waived in such cases. Most included autopsies were limited to the chest and abdomen, but some cases were examined fully according to the circumstances of their death. Personal protective equipment was used among all staff members. The procedures involved the minimum needed number of staff. Full external inspection of the body as it was received was conducted initially, followed by midline chest and abdomen incision with extraction of the lungs and heart with full inspection and documentation by “inspection report and photographing of all positive findings.” Tissue sampling was limited to the lungs and heart.
- Histopathologic examination
- Tissue specimens were fixed in 10% formalin for 72 hours, dehydrated by ethanol, and cleared twice by xylene, then embedded in paraffin, and sectioned as 5 μm sections. The prepared sections were dried and stained by hematoxylin and eosin full final histopathologic examination, which was conducted by the first authors and the senior author (M.A. and M.A.A.-A.), who are consultant histopathologists at JUH.
- The differentiation between “death from COVID-19” vs. “death with SARS-CoV-2 infection” was based on the presence of DAD in the former group in contrast to its total absence in the later group.
- EM examination
- The procedure of EM was adopted from a previous publication by Shatarat et al. [32]. Briefly, the extracted tissues from autopsies were fixed for one hour in buffered 1%–2% osmium tetroxide followed by gradual dehydration in ethanol/propylene oxide and embedding in epoxy resin media mixture. The U7 ultra-cut was used to obtain sections with a range of 70–90 nm, followed by mounting on 200 mesh copper grids, and contrasted with uranyl acetate and lead citrate [32]. The FEI Morgagni Transmission Electron Microscope was used for image acquisition and analysis.
- Criteria for identification of “death from COVID-19” vs. “death with SARS-CoV-2 infection”
- As previously stated, we used histopathologic findings as the sole criterion to define death from COVID-19 if DAD was found while its absence, was used to denote death with SARS-CoV-2 infection.
- Statistical analysis
- Based on the small sample size, two-sided Fisher exact test was used to investigate categorical variables, while assessment of the association between age as a continuous variable with dichotomous categorical variables was done using the Mann-Whitney U test. Statistical analysis was done using IBM SPSS Statistics for Windows ver. 22.0 (IBM Corp., Armonk, NY, USA).
MATERIALS AND METHODS
- Characteristics of the included cases
- The study cohort comprised 17 individuals who were positive for COVID-19 at postmortem SARS-CoV-2 assessment by qPCR testing of nasopharyngeal swabs (n = 4), serologic testing for SARS-CoV-2 IgM (n=3) or confirmed by both methods (n=10). Two individuals were diagnosed with COVID-19 by qPCR several days prior to death (5 days and 12 days antemortem), whereas the remaining cases had positive test results within 24 hours from being declared dead. The majority of cases were males (76.5%), Jordanians (70.6%), and the average age at time of death was 50 years (Table 1).
- The majority of cases were declared dead at home (n = 11, 64.7%). Eight cases were diagnosed during the first COVID-19 wave in Jordan, while the remaining nine cases were diagnosed during the second wave of COVID-19 in the country.
- The most frequent co-morbidities in the study cohort were hypertension and obesity (n = 5 for both). Previous emergency department visits were recorded for eight cases (four of which were for respiratory symptoms including shortness of breath and cough).
- Four cases died with SARS-CoV-2 infection compared to 13 dying from COVID-19
- Evidence of the presence of SARS-CoV-2 with the absence of DAD was found in four cases (23.5%). Based on that, the case series was divided into two groups “death with SARS-CoV-2 infection” vs. “death from COVID-19.” In the former group, two cases were presumptively diagnosed with pneumonia at death, one with ACS and the last case was diagnosed with subdural and subarachnoid hemorrhage. For the “death from COVID-19” group, six were diagnosed with pneumonia, four were diagnosed with pulmonary embolism, and three were diagnosed with acute coronary syndrome. The mean age of individuals within the “death with SARS-CoV-2 infection” was younger than the mean age of those within the “death from COVID-19” group (39 years vs. 54 years, p=.078, Mann-Whitney U test).
- Absence of co-morbidities was recorded among all cases in the “death with SARS-CoV-2 infection” (0/4) in contrast to (9/11, 81.8%) having at least one co-morbid condition in the “death from COVID-19” group with missing data in two cases (p=.011, Fisher exact test).
- Autopsy findings from lung tissues
- Gross examination of the lungs in the study cohort revealed the common occurrence of congestion and edema followed by hepatization of lungs (Table 2).
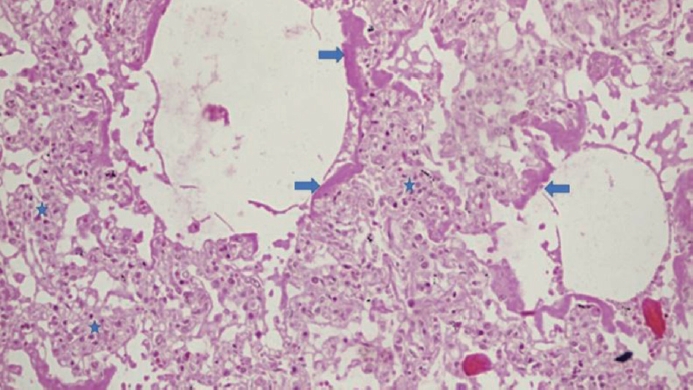
- On histopathologic examination, DAD was detected in 13/17 cases (76.5%), which was sub-classified into exudative DAD (n = 5), proliferative DAD (n= 7), and a single case of evolving fibrosing DAD. All cases with exudative DAD showed hyaline membrane formation, denudation and/or necrosis of type 1 pneumocytes (Fig. 1).
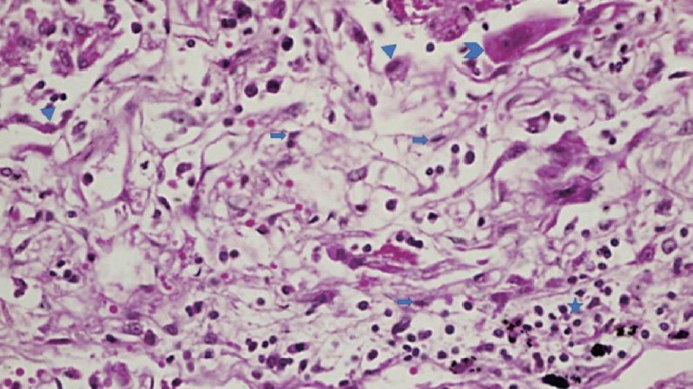
- Variable degrees of hyaline membrane organization and type II pneumocytes hyperplasia were noted in the seven proliferative DAD cases (Fig. 2).
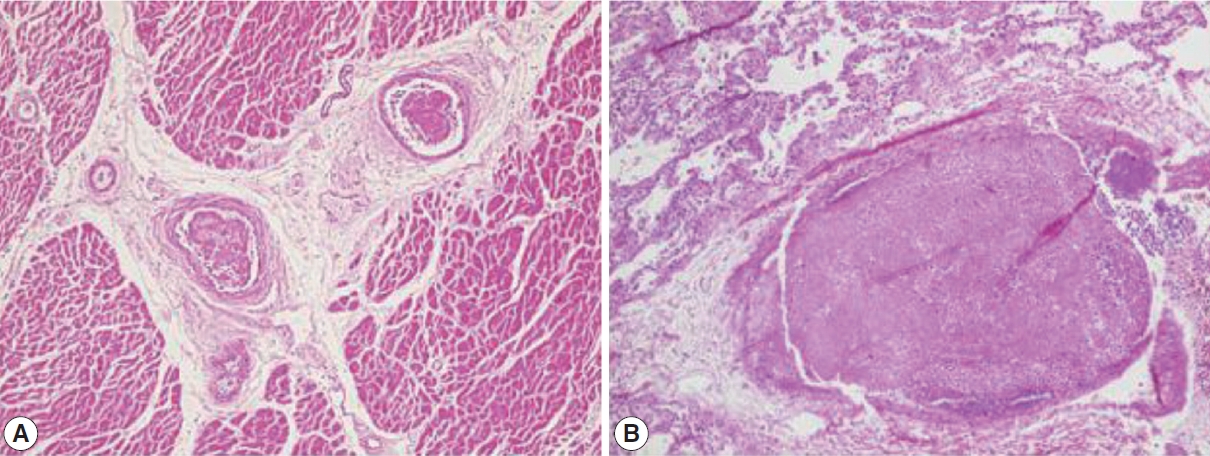
- A majority of cases displayed evidence of interstitial and intraalveolar edema (64.7%), lymphocytic infiltration of the alveoli (64.7%), and pulmonary capillaries congestion (100%). Microthrombi were found in eight cases (47%), of which two cases showed no DAD, two cases displayed exudative DAD, and four cases showed proliferative DAD. Emphysematous changes were noted in eight cases (Table 2, Fig. 3).
- In the absence of co-morbidities, no specific histologic changes were noticed in alveoli (n=4), compared to the presence of lymphocytic infiltration in 8/9 of the cases with co-morbidities (p= .011, Fisher exact test). All cases in the “died with COVID-19” group lacked alveolar changes by definition (n=4), compared to 11/13 with lymphocytic infiltration in the “died from COVID-19” group (p=.006, Fisher exact test).
- Autopsy findings from heart tissues
- Gross examination of the heart in this case series revealed the relatively high prevalence of atherosclerotic changes in coronary arteries (n = 8, 47.1%). Histopathologic changes were scarcely detected. Fibrosis in intima and thickening of media were detected in a single case, while myocardial cell necrosis was found in another single case (Table 2).
- EM findings
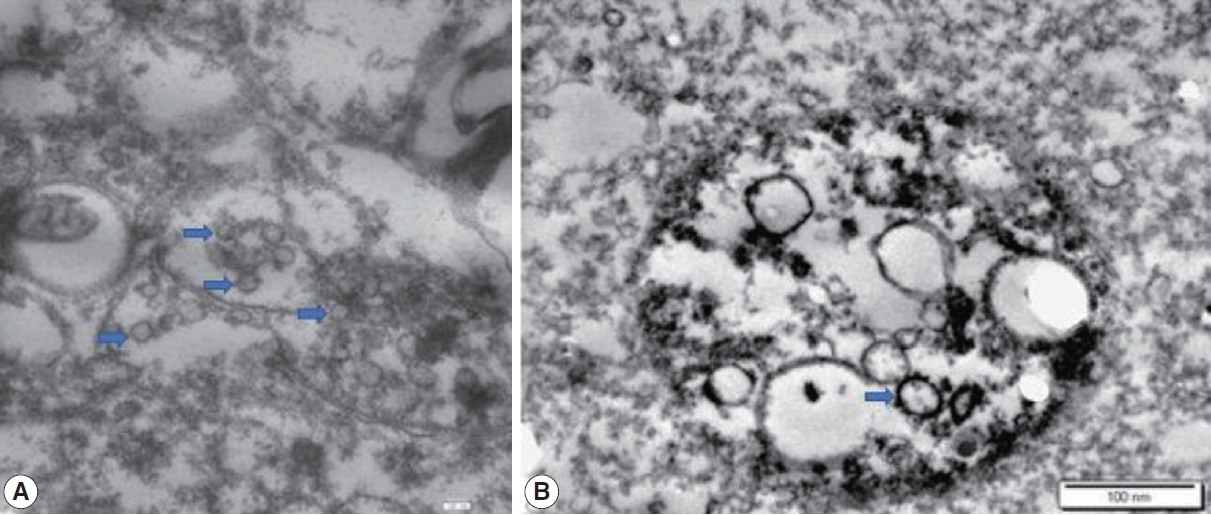
- All cases were examined using EM, and spherical structures with surface spikes were found in all cases (n=17, 100%) (Fig. 4).
RESULTS
- This study represents the first description of autopsy findings from individuals positive for COVID-19 in Jordan, and Arab countries to the best of our knowledge. Previously, a majority of autopsy case series in the context of COVID-19 were mostly conducted in the United States, Europe, and China [21]. Such a study appears of prime importance in the Middle East region for a number of reasons. First, challenges were posed to forensic pathologists considering the controversies around the Islamic burial rituals and handling of corpses if autopsies revealed the presence of SARS-CoV-2 [33,34]. This is particularly relevant considering the evidence suggesting the presence of replicative SARS-CoV-2 a few days postmortem as shown in the study by Grassi et al. [35] that involved 29 autopsies examined in Italy. Our findings confirmed the presence of the virus in all cases included in this study. The diagnosis of COVID-19 in this case series was established by postmortem molecular or serologic testing for SARS-CoV-2 even in the absence of typical clinical presentation of COVID-19 at time of death. Second, this study is important in Jordan considering the previous evidence of high prevalence of embracing conspiratorial beliefs towards emerging virus infections that could entail irrational COVID denialism [36]. The findings of this study add an explicit proof of the presence of the virus among autopsies that tested positive for the virus through direct EM visualization. The confirmation of coronavirus presence by EM examination added further proof of virus presence in all included cases despite the variability in laboratory testing approach initially used in this case series (qPCR vs. serologic testing).
- Macroscopic and microscopic findings in the majority of cases (13/17, 76.5%) in this study were consistent with previous literature suggesting the crucial role of DAD as the hallmark of acute respiratory distress syndrome complicating COVID-19 infections [37-39]. The predominance of proliferative DAD in this case series indicates the late presentation of a substantial number of cases with subsequent ominous outcome. The wide prevalence of DAD as the predominant feature in lung parenchyma among COVID-19–positive autopsies was reported previously in various reports from the United States [40,41], Germany [30,42], Spain [43], Italy [44], and China [45]. An early case series from Switzerland that involved 21 autopsies examined following COVID-19–related mortalities revealed that the major cause of death was respiratory insufficiency due to exudative DAD and massive capillary congestion [46]. In addition, the Swiss case series reported the detection of microthrombi despite the intake of anticoagulation prior to death [46].
- The role of coagulopathy in the pathophysiology of COVID-19 was manifested by the frequent detection of microthrombi in lungs (8/17, 47.1%) in the study cohort. Likewise, and indicative of the central role of thrombotic microangiopathy in critical cases of COVID-19, a study from Iran reported the presence of thrombotic microangiopathy in 60% of 31 lung biopsies from patients who passed away due to COVID-19 [47]. Additional reports on autopsy findings amid COVID-19 pandemic found a high incidence of thromboembolic events suggesting its role in the fatal outcome of COVID-19 [39,48]. A recent comprehensive review for autoptic investigations from of 749 COVID-19 mortalities in 14 studies revealed the presence of pulmonary embolism-related findings in 30% of cases, with venous thromboembolic events as the cause of death 25% of the cases [49]. An early Austrian study involving 11 autopsies showed that thrombosis in small pulmonary arteries was a fundamental finding resulting in mortality due to COVID-19 [50].
- The frequency of co-morbidities was high in this case series among mortalities that were linked directly to SARS-CoV-2 infection in contrast to its total absence among those who died with the disease. Conditions like hypertension, obesity, and type 2 diabetes mellitus were previously linked to excess mortality among SARS-CoV-2 infected patients [51]. In line with this observation, co-morbidities in this cohort were linked to death from COVID-19 rather than death with the virus.
- A novel finding of this study was the observation that four out of 17 individuals died without significant histopathologic pulmonary changes. This observation was made despite the presence of SARS-CoV-2 as evidenced by qPCR, serology, and EM findings. One important parameter in the assessment of infectious disease is the CFR, which is defined as “the proportion of individuals diagnosed with a disease who die from that disease” [3]. The aspects of bias in the efforts to estimate COVID-19 CFR appear to cause an underestimation through time lags in reporting of death, and overestimation through underreporting of asymptomatic and mild cases [5]. Another important cause of bias, which was noticed in this study, is the overestimation of fatalities due to COVID-19. This can happen as a result of reporting any death with a positive SARS-CoV-2 testing result as a COVID-19 case, even in the absence of sufficient evidence that the individual died as a result of virus infection, which might be present as an incidental finding [52]. Such a scenario can frequently occur in the course of COVID-19 epidemic waves with a high proportion of asymptomatic cases/mild disease [16]. Hence, subclinical cases are rarely tested and consequently are missed.
- In this study, even with a small sample size, the proportion of death with SARS-CoV-2 infection appears relatively high 4/17 (23.5%). In line with this finding, a study from Italy reported on the causes of death among nine cases that tested positive for COVID-19 at time of death, with five cases dying as a result of carbon monoxide poisoning in a nursing home (death with SARS-CoV-2 infection) [11]. In an earlier study from Germany, Edler et al. [42] found a similar observation; however, at a much smaller scale with only 5% out of 80 autopsies that were labeled as “non-COVID-19 deaths.”
- It is important to note that the incidental finding of SARS-CoV-2 in autopsies can be higher in outbreak situation. The current study took place during the first and second waves of COVID-19 in Jordan, with more than several thousand of newly diagnosed cases at waves’ peaks [53]. Several differential diagnoses should be considered in outbreak setting with community spread of SARS-CoV-2, including other viral infections, previously undiagnosed heart disease, and drug toxicity among other conditions [54]. Despite the absence of DAD in four cases, the role of SARS-CoV-2 in mortality cannot be ruled out, particularly in the cases with ACS and this issue could be viewed as a caveat in our stratification approach. This is evidenced by the previous studies linking COVID-19 with direct cardiac damage and indirect involvement through the thrombotic complications [55]. However, we are inclined to believe that the cases in the “death with SARS-CoV-2 infection” group did not pass away due to SARS-CoV-2 complications since the subjects in this group lacked co-morbidities and were younger compared to those with histopathologic evidence of death due to the infection.
- Finally, the findings in this case series should be interpreted in light of several limitations that included: (1) the small sample size, which was mostly related to restriction of autopsy examination to medicolegal cases; (2) potential selection bias since all deaths were considered as medicolegal cases; (3) missing of full clinical history data in a few cases, including the history of COVID-19 vaccine uptake among the four cases included following the start of vaccination campaign in Jordan, besides the lack of data on microbiologic testing to rule out bacterial superinfections; (4) the approach used to stratify the cases into “died of COVID-19” vs. “died with SARS-CoV-2 infection” depended on the detection of DAD solely. Thus, future studies should benefit from a refined approach of classification including consideration of detailed medical records from the included cases, as well as the full utility of postmortem radiology, besides toxicologic investigations [20]; and finally (5) virtual autopsy (virtopsy) was not conducted in this study and should be considered in the future studies considering its promising role for postmortem investigation in the context of resolving disputed cases of COVID-19 deaths.
- To conclude, in this case series, we described the histopathologic findings of COVID-19–related mortalities and explored the distinction between death due to COVID-19 as opposed to dying with SARS-CoV-2 infection. This disparity might be supported by the younger age and absence of co-morbidities in the “died with COVID-19” group; however, this observation is pending further evidence from studies with larger samples. Besides DAD as the primary histopathologic finding among the “death from COVID-19” group, microthrombi were frequently detected. This microthrombi can be indicative of a hypercoagulability state. Such a state appears to play a prominent role in the pathophysiology of severe and critical cases of COVID-19, which can be implicated in the mortality from the disease.
DISCUSSION
Ethics Statement
This study was approved by the Institutional Review Board of Jordan University Hospital (JUH–IRB, decision No. 78/2021, reference No. 10/2021/5885, issued on 14 March 2021). The written informed consent from the next of kin was waived based on the medico-legal status of the cases.
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author contributions
Conceptualization: MA, MAAA. Data curation: MA, IT, MS, ABH, IMAA, BAO, SAM, HAR, ASA, MZ, MAAA. Formal analysis: MA, MS. Funding acquisition: MA. Investigation: MA, IT, MS, ABH, IMAA, BAO, SAM, HAR, ASA, MZ, MAAA. Methodology: MA, IT, MS, ABH, IMAA, BAO, SAM, HAR, ASA, MZ, MAAA. Project administration: MA. Resources: MA, IT, MS, ABH, IMAA, BAO, SAM, HAR, ASA, MZ, MAAA. Supervision: MA, MAAA. Validation: MA, MS. Visualization: MA, MS. Writing— original draft preparation: MA, MS. Writing—review & editing: MA, IT, MS, ABH, IMAA, BAO, SAM, HAR, ASA, MZ, MAAA. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
This research was funded by Deanship of Scientific Research at the University of Jordan, grant number: 498/2021/19; (24/2020–2021), granted on 21 April 2021.
| Variable | No. (%) |
|---|---|
| Mean age (range, yr) | 50 (27–77) |
| Sex | |
| Male | 13 (76.5) |
| Female | 4 (23.5) |
| Nationality | |
| Jordanian | 12 (70.6) |
| Non-Jordanian | 5 (29.4) |
| Co-morbidity | |
| Obesity | 5 (29.4) |
| Hypertension | 5 (29.4) |
| Type 2 DM | 3 (17.6) |
| Obstructive sleep apnea | 2 (11.8) |
| Allergy | 1 (5.9) |
| Cerebrovascular accident | 1 (5.9) |
| Depression on treatment | 1 (5.9) |
| Medically free | 4 (23.5) |
| Information is not available | 1 (5.9) |
| Pronounced cause of deatha | |
| Pneumonia | 7 (41.2) |
| Pulmonary embolism | 4 (23.5) |
| Coronary artery thrombus | 4 (23.5) |
| Multiorgan failure | 1 (5.9) |
| Intracranial hemorrhage | 1 (5.9) |
- 1. Gallo LG, Oliveira AF, Abrahao AA, et al. Ten epidemiological parameters of COVID-19: use of rapid literature review to inform predictive models during the pandemic. Front Public Health 2020; 8: 598547.ArticlePubMedPMC
- 2. Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020; 323: 1775-6. ArticlePubMed
- 3. World Health Organization. Estimating mortality from COVID-19: scientific brief [Internet]. Geneva: World Health Oragnization, 2020 [cited 2022 Oct 29]. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci-Brief-Mortality-2020.1.
- 4. Schwab N, Nienhold R, Henkel M, et al. COVID-19 autopsies reveal underreporting of SARS-CoV-2 infection and scarcity of co-infections. Front Med (Lausanne) 2022; 9: 868954.ArticlePubMedPMC
- 5. Grande E, Fedeli U, Pappagallo M, et al. Variation in cause-specific mortality rates in Italy during the first wave of the COVID-19 pandemic: a study based on nationwide data. Int J Environ Res Public Health 2022; 19: 805.ArticlePubMedPMC
- 6. Sessa F, Bertozzi G, Cipolloni L, et al. Clinical-forensic autopsy findings to defeat COVID-19 disease: a literature review. J Clin Med 2020; 9: 2026.ArticlePubMedPMC
- 7. Maiese A, Manetti AC, La Russa R, et al. Autopsy findings in COVID-19-related deaths: a literature review. Forensic Sci Med Pathol 2021; 17: 279-96. ArticlePubMedPDF
- 8. Kim MY, Cheong H, Kim HS; Working Group for Standard Autopsy Guideline for COVID-19 from the Korean Society for Legal Medicine. Proposal of the autopsy guideline for infectious diseases: preparation for the post-COVID-19 era (abridged translation). J Korean Med Sci 2020; 35: e310. ArticlePubMedPMCPDF
- 9. Salerno M, Sessa F, Piscopo A, et al. No autopsies on COVID-19 deaths: a missed opportunity and the lockdown of science. J Clin Med 2020; 9: 1472.ArticlePubMedPMC
- 10. Filograna L, Manenti G, Grassi S, et al. Virtual autopsy in SARS-CoV-2 breakthrough infection: a case report. Forensic Imaging 2022; 30: 200520.ArticlePMC
- 11. De-Giorgio F, Grassi VM, Bergamin E, et al. Dying “from” or “with” COVID-19 during the pandemic: medico-legal issues according to a population perspective. Int J Environ Res Public Health 2021; 18: 8851.ArticlePubMedPMC
- 12. Esposito M, Salerno M, Scoto E, Di Nunno N, Sessa F. The impact of the COVID-19 pandemic on the practice of forensic medicine: an overview. Healthcare (Basel) 2022; 10: 319.ArticlePubMedPMC
- 13. Filograna L, Manenti G, Arena V, et al. Claimed medical malpractice in fatal SARS-CoV-2 infections: the importance of combining ante- and post-mortem radiological data and autopsy findings for correct forensic analysis. Forensic Imaging 2021; 25: 200454.ArticlePMC
- 14. Rakislova N, Marimon L, Ismail MR, et al. Minimally invasive autopsy practice in COVID-19 cases: biosafety and findings. Pathogens 2021; 10: 412.ArticlePubMedPMC
- 15. Harapan H, Itoh N, Yufika A, et al. Coronavirus disease 2019 (COVID-19): a literature review. J Infect Public Health 2020; 13: 667-73. ArticlePubMedPMC
- 16. Sah P, Fitzpatrick MC, Zimmer CF, et al. Asymptomatic SARS-CoV-2 infection: a systematic review and meta-analysis. Proc Natl Acad Sci U S A 2021; 118: e2109229118. ArticlePubMedPMC
- 17. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA 2020; 324: 782-93. ArticlePubMed
- 18. Grippo F, Navarra S, Orsi C, et al. The role of COVID-19 in the death of SARS-CoV-2-positive patients: a study based on death certificates. J Clin Med 2020; 9: 3459.ArticlePubMedPMC
- 19. Slater TA, Straw S, Drozd M, Kamalathasan S, Cowley A, Witte KK. Dying ‘due to’ or ‘with’ COVID-19: a cause of death analysis in hospitalised patients. Clin Med (Lond) 2020; 20: e189-90. ArticlePubMedPMC
- 20. Giorgetti A, Orazietti V, Busardo FP, Pirani F, Giorgetti R. Died with or died of? Development and testing of a SARS CoV-2 significance score to assess the role of COVID-19 in the deaths of affected patients. Diagnostics (Basel) 2021; 11: 190.ArticlePubMedPMC
- 21. Sperhake JP. Autopsies of COVID-19 deceased? Absolutely! Leg Med (Tokyo) 2020; 47: 101769.ArticlePubMedPMC
- 22. Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020; 181: 271-80. ArticlePubMedPMC
- 23. Gupta A, Madhavan MV, Sehgal K, et al. Extrapulmonary manifestations of COVID-19. Nat Med 2020; 26: 1017-32. PubMedPDF
- 24. Abou-Ismail MY, Diamond A, Kapoor S, Arafah Y, Nayak L. The hypercoagulable state in COVID-19: Incidence, pathophysiology, and management. Thromb Res 2020; 194: 101-15. ArticlePubMedPMC
- 25. Nishiga M, Wang DW, Han Y, Lewis DB, Wu JC. COVID-19 and cardiovascular disease: from basic mechanisms to clinical perspectives. Nat Rev Cardiol 2020; 17: 543-58. ArticlePubMedPMCPDF
- 26. Bohn MK, Mancini N, Loh TP, et al. IFCC interim guidelines on molecular testing of SARS-CoV-2 infection. Clin Chem Lab Med 2020; 58: 1993-2000. ArticlePubMed
- 27. Pan Y, Li X, Yang G, et al. Serological immunochromatographic approach in diagnosis with SARS-CoV-2 infected COVID-19 patients. J Infect 2020; 81: e28-32. Article
- 28. Brahim Belhaouari D, Fontanini A, Baudoin JP, et al. The strengths of scanning electron microscopy in deciphering SARS-CoV-2 infectious cycle. Front Microbiol 2020; 11: 2014.PubMedPMC
- 29. Hanley B, Lucas SB, Youd E, Swift B, Osborn M. Autopsy in suspected COVID-19 cases. J Clin Pathol 2020; 73: 239-42. ArticlePubMed
- 30. Schaller T, Hirschbuhl K, Burkhardt K, et al. Postmortem examination of patients with COVID-19. JAMA 2020; 323: 2518-20. ArticlePubMedPMC
- 31. Satturwar S, Fowkes M, Farver C, et al. Postmortem findings associated with SARS-CoV-2: systematic review and meta-analysis. Am J Surg Pathol 2021; 45: 587-603. PubMedPMC
- 32. Shatarat A, Alzghoul L, Al-Qattan D, Elbeltagy M. Anatomical and ultrastructural sex differences in mean diameter and thickness of myelinated axons in adult rat corpus callosum. Int J Morphol 2020; 38: 505-12. Article
- 33. Nurhayati N, Purnama TB. Funeral processes during the COVID-19 pandemic: perceptions among Islamic religious leaders in Indonesia. J Relig Health 2021; 60: 3418-33. ArticlePubMedPMCPDF
- 34. Al-Dawoody A, Finegan O. COVID-19 and Islamic burial laws: safeguarding dignity of the dead [Internet]. Geneva: International Committee of the Red Cross, 2020 [cited 2020 Apr 30]. Available from: https://blogs.icrc.org/law-and-policy/2020/04/30/covid-19-islamic-burial-laws/.
- 35. Grassi S, Arena V, Cattani P, et al. SARS-CoV-2 viral load and replication in postmortem examinations. Int J Legal Med 2022; 136: 935-9. ArticlePubMedPMCPDF
- 36. Sallam M, Dababseh D, Yaseen A, et al. COVID-19 misinformation: mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS One 2020; 15: e0243264. ArticlePubMedPMC
- 37. Youd E, Moore L. COVID-19 autopsy in people who died in community settings: the first series. J Clin Pathol 2020; 73: 840-4. ArticlePubMed
- 38. Elezkurtaj S, Greuel S, Ihlow J, et al. Causes of death and comorbidities in hospitalized patients with COVID-19. Sci Rep 2021; 11: 4263.ArticlePubMedPMCPDF
- 39. Remmelink M, De Mendonca R, D’Haene N, et al. Unspecific postmortem findings despite multiorgan viral spread in COVID-19 patients. Crit Care 2020; 24: 495.ArticlePubMedPMCPDF
- 40. Bradley BT, Maioli H, Johnston R, et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: a case series. Lancet 2020; 396: 320-32. ArticlePubMedPMC
- 41. Barton LM, Duval EJ, Stroberg E, Ghosh S, Mukhopadhyay S. COVID-19 autopsies, Oklahoma, USA. Am J Clin Pathol 2020; 153: 725-33. ArticlePubMedPDF
- 42. Edler C, Schroder AS, Aepfelbacher M, et al. Dying with SARS-CoV-2 infection-an autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int J Legal Med 2020; 134: 1275-84. ArticlePubMedPMCPDF
- 43. The COVID-19 Autopsy. The first COVID-19 autopsy in Spain performed during the early stages of the pandemic. Rev Esp Patol 2020; 53: 182-7. ArticlePubMedPMC
- 44. Carsana L, Sonzogni A, Nasr A, et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: a two-centre descriptive study. Lancet Infect Dis 2020; 20: 1135-40. ArticlePubMedPMC
- 45. Ding Y, Wang H, Shen H, et al. The clinical pathology of severe acute respiratory syndrome (SARS): a report from China. J Pathol 2003; 200: 282-9. ArticlePubMedPMC
- 46. Menter T, Haslbauer JD, Nienhold R, et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020; 77: 198-209. ArticlePubMedPMCPDF
- 47. Sadegh Beigee F, Pourabdollah Toutkaboni M, Khalili N, et al. Diffuse alveolar damage and thrombotic microangiopathy are the main histopathological findings in lung tissue biopsy samples of COVID-19 patients. Pathol Res Pract 2020; 216: 153228.ArticlePubMedPMC
- 48. Caramaschi S, Kapp ME, Miller SE, et al. Histopathological findings and clinicopathologic correlation in COVID-19: a systematic review. Mod Pathol 2021; 34: 1614-33. ArticlePubMedPMCPDF
- 49. Zuin M, Engelen MM, Bilato C, et al. Prevalence of acute pulmonary embolism at autopsy in patients with COVID-19. Am J Cardiol 2022; 171: 159-64. ArticlePubMedPMC
- 50. Lax SF, Skok K, Zechner P, et al. Pulmonary arterial thrombosis in COVID-19 with fatal outcome: results from a prospective, single-center, clinicopathologic case series. Ann Intern Med 2020; 173: 350-61. PubMed
- 51. Bhaskaran K, Bacon S, Evans SJ, et al. Factors associated with deaths due to COVID-19 versus other causes: population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet Reg Health Eur 2021; 6: 100109.PubMedPMC
- 52. Niforatos JD, Melnick ER, Faust JS. Covid-19 fatality is likely overestimated. BMJ 2020; 368: m1113.ArticlePubMed
- 53. Sallam M, Mahafzah A. Molecular analysis of SARS-CoV-2 genetic lineages in Jordan: tracking the introduction and spread of COVID-19 UK variant of concern at a country level. Pathogens 2021; 10: 302.ArticlePubMedPMC
- 54. Geller RL, Aungst JL, Newton-Levinson A, et al. Is it COVID-19? The value of medicolegal autopsies during the first year of the COVID-19 pandemic. Forensic Sci Int 2022; 330: 111106.ArticlePubMed
- 55. Schoene D, Schnekenberg LG, Pallesen LP, et al. Pathophysiology of cardiac injury in COVID-19 patients with acute ischaemic stroke: what do we know so far?: a review of the current literature. Life (Basel) 2022; 12: 75.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Massive Splenic Infarction Following COVID-19 Infection, with Histopathological Observations, and Review of the Literature
Yousef Samir Amr, Aseel Qassem Al-Omari, Mousa Husein Saadeh, Samir Sami Amr
Open Journal of Pathology.2025; 15(02): 69. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
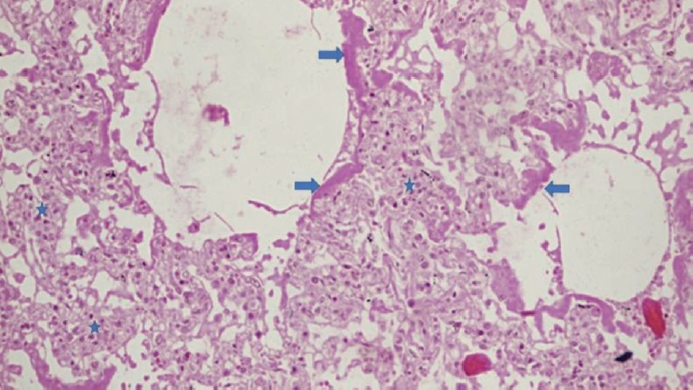
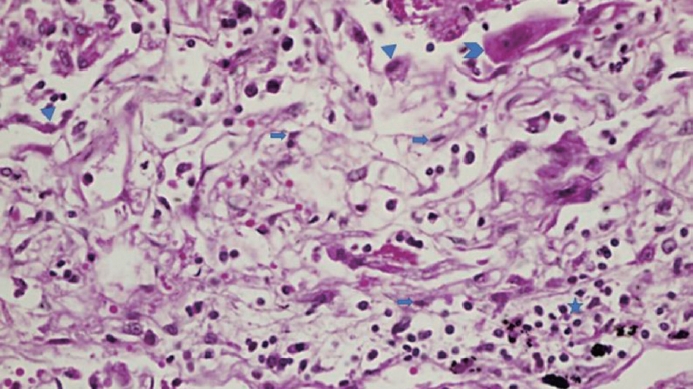
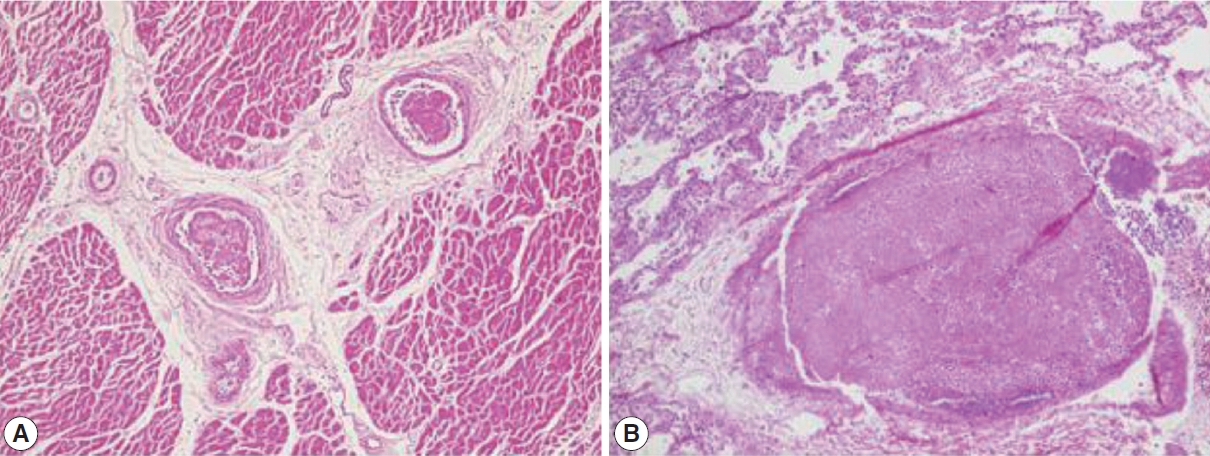
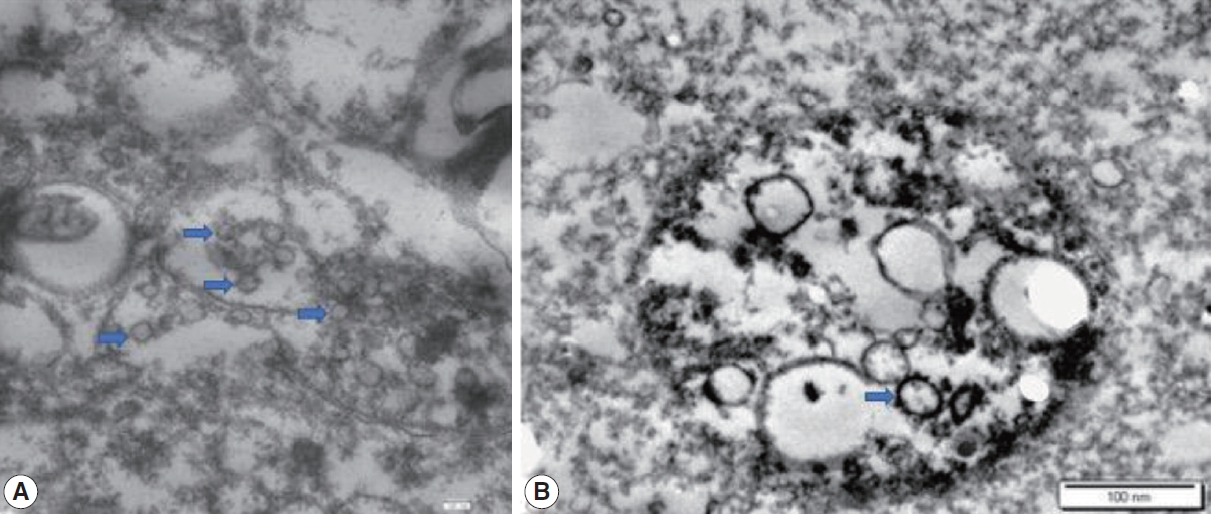




Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
| Variable | No. (%) |
|---|---|
| Mean age (range, yr) | 50 (27–77) |
| Sex | |
| Male | 13 (76.5) |
| Female | 4 (23.5) |
| Nationality | |
| Jordanian | 12 (70.6) |
| Non-Jordanian | 5 (29.4) |
| Co-morbidity | |
| Obesity | 5 (29.4) |
| Hypertension | 5 (29.4) |
| Type 2 DM | 3 (17.6) |
| Obstructive sleep apnea | 2 (11.8) |
| Allergy | 1 (5.9) |
| Cerebrovascular accident | 1 (5.9) |
| Depression on treatment | 1 (5.9) |
| Medically free | 4 (23.5) |
| Information is not available | 1 (5.9) |
| Pronounced cause of death |
|
| Pneumonia | 7 (41.2) |
| Pulmonary embolism | 4 (23.5) |
| Coronary artery thrombus | 4 (23.5) |
| Multiorgan failure | 1 (5.9) |
| Intracranial hemorrhage | 1 (5.9) |
| Finding | Total cases (n = 17) | Died of COVID-19(n = 13) | Died with SARS-CoV-2 infection (n = 4) | ||
|---|---|---|---|---|---|
| Lung | |||||
| Gross | |||||
| Congestion and edema | 12 (70.6) | 10 (76.9) | 2 (50.0) | ||
| Hepatization | 10 (58.8) | 7 (53.8) | 3 (75.0) | ||
| Hemorrhage | 10 (58.8) | 9 (69.2) | 1 (25.0) | ||
| Vascular thrombosis | 3 (17.6) | 3 (23.1) | 0 | ||
| Pleural adhesions | 3 (17.6) | 3 (23.1) | 0 | ||
| Saddle pulmonary embolism | 2 (11.8) | 2 (15.4) | 0 | ||
| Pleural effusion | 1 (5.9) | 1 (7.7) | 0 | ||
| Histopathologic | |||||
| Alveolar congestion only | 4 (23.5) | 0 | 4 (100) | ||
| Exudative diffuse alveolar damage | 5 (29.4) | 5 (38.5) | 0 | ||
| Proliferative diffuse alveolar damage | 7 (41.2) | 7 (53.8) | 0 | ||
| Early fibrosing diffuse alveolar damage | 1 (5.9) | 1 (7.7) | 0 | ||
| Specific microscopic findings | |||||
| Hyaline membranes with type I pneumocytes necrosis or denudation | 5 (29.4) | 5 (38.5) | 0 | ||
| Organizing or remnants of hyaline membrane and type II pneumocytes hyperplasia | 7 (41.2) | 7 (53.8) | 0 | ||
| Early and focal fibrosis | 1 (5.9) | 1 (7.7) | 0 | ||
| Diffuse collagenous fibrosis | 0 | 0 | 0 | ||
| Interstitial and intra-alveolar edema | 17 (100) | 13 (100) | 4 (100) | ||
| Microscopic honeycomb-like change | 0 | 0 | 0 | ||
| Collapsed alveoli | 0 | 0 | 0 | ||
| Lymphocytic infiltration | 11 (64.7) | 11 (84.6) | 0 | ||
| Traction bronchiectasis | 0 | 0 | 0 | ||
| Pneumocytes | |||||
| No change | 4 (23.5) | 0 | 4 (100) | ||
| Denudation and necrosis of type I pneumocytes | 4 (23.5) | 4 (30.8) | 0 | ||
| Proliferation of type II pneumocyte | 3 (17.6) | 3 (23.1) | 0 | ||
| Denudation and necrosis of type I pneumocytes and proliferation of type II pneumocyte | 6 (35.3) | 6 (46.2) | 0 | ||
| Necrosis of endothelial cells | |||||
| No | 16 (94.1) | 12 (92.3) | 4 (100) | ||
| Yes | 1 (5.9) | 1 (7.7) | 0 | ||
| Neutrophil aggregation | |||||
| No | 16 (94.1) | 12 (92.3) | 4 (100) | ||
| Yes | 1 (5.9) | 1 (7.7) | 0 | ||
| Microthrombi | |||||
| Absent | 9 (52.9) | 6 (46.2) | 3 (75.0) | ||
| Present | 8 (47.1) | 7 (53.8) | 1 (25.0) | ||
| Hemorrhage | |||||
| Absent | 5 (29.4) | 3 (23.1) | 2 (50.0) | ||
| Present | 12 (70.6) | 10 (76.9) | 2 (50.0) | ||
| Pulmonary capillary congestion | |||||
| Absent | 0 | 0 | 0 | ||
| Present | 17 (100) | 13 (100) | 4 (100) | ||
| Reactive pneumocytes and syncytial cells | |||||
| Absent | 7 (41.2) | 4 (30.8) | 3 (75.0) | ||
| Present | 10 (58.8) | 9 (69.2) | 1 (25.0) | ||
| Focal emphysema | |||||
| Absent | 9 (52.9) | 7 (53.8) | 2 (50.0) | ||
| Present | 8 (47.1) | 6 (46.2) | 2 (50.0) | ||
| Vasculitis | |||||
| Absent | 17 (100) | 13 (100) | 4 (100) | ||
| Present | 0 | 0 | 0 | ||
| Heart | |||||
| Gross | |||||
| No significant changes | 5 (29.4) | 4 (30.8) | 1 (25.0) | ||
| Coronary arteries atherosclerosis | 8 (47.1) | 6 (46.2) | 2 (50.0) | ||
| Cardiac hypertrophy | 3 (17.6) | 1 (7.7) | 2 (50.0) | ||
| Cardiomegaly | 3 (17.6) | 1 (7.7) | 2 (50.0) | ||
| Acute thrombus | 2 (11.8) | 0 | 2 (50.0) | ||
| Fibrosis | 1 (5.9) | 1 (7.7) | 0 | ||
| Specific microscopic findings | |||||
| Fibrosis in intima | |||||
| Absent | 16 (94.1) | 12 (92.3) | 4 (100) | ||
| Present | 1 (5.9) | 1 (7.7) | 0 | ||
| Thickening of media | |||||
| Absent | 16 (94.1) | 12 (92.3) | 4 (100) | ||
| Present | 1 (5.9) | 1 (7.7) | 0 | ||
| Myocardial hypertrophy | |||||
| Absent | 17 (100) | 13 (100) | 4 (100) | ||
| Present | 0 | 0 | 0 | ||
| Senile amyloidosis | |||||
| Absent | 17 (100) | 13 (100) | 4 (100) | ||
| Present | 0 | 0 | 0 | ||
| Myocardial cell necrosis | |||||
| Absent | 16 (94.1) | 12 (92.3) | 4 (100) | ||
| Present | 1 (5.9) | 1 (7.7) | 0 | ||
DM, diabetes mellitus. Pronounced cause of death: before autopsy examination.
Values are presented as number (%). COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.

