 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 56(3); 2022 > Article
-
Original Article
Expression of prostate-specific membrane antigen in the neovasculature of primary tumors and lymph node metastasis of laryngeal squamous cell carcinomas -
Gamze Erkılınç,1
 , Hasan Yasan2, Yusuf Çağdaş Kumbul2, Mehmet Emre Sivrice2, Meltem Durgun1
, Hasan Yasan2, Yusuf Çağdaş Kumbul2, Mehmet Emre Sivrice2, Meltem Durgun1 -
Journal of Pathology and Translational Medicine 2022;56(3):134-143.
DOI: https://doi.org/10.4132/jptm.2022.02.22
Published online: May 3, 2022
1Department of Pathology, Süleyman Demirel Univesity, Çünür/Isparta, Turkey
2Department of Otorhinolaryngology, Süleyman Demirel Univesity, Çünür/Isparta, Turkey
- Corresponding Author: Gamze Erkılınç, MD, Department of Pathology, Süleyman Demirel Univesity, Süleyman Demirel Street, 32260, Çünür/Isparta, Turkey Tel: +90-2462113714, Fax: +90-2462112830, E-mail: gamzecirak@gmail.com
© 2022 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- Prostate-specific membrane antigen (PSMA) expression is encountered in tumor-associated neovascularization.
-
Methods
- PSMA-antibody was applied to the paraffin blocks of 51 patients who were diagnosed with squamous cell carcinoma of the larynx and underwent laryngectomy and one who underwent lymph node dissection. The percentage of vascular expression in tumoral and extratumoral stroma and lymph nodes and intensity score in tumoral epithelium were evaluated and divided into groups according to the level of PSMA expression. Final PSMA expression was determined by multiplying intensity and percentage scores.
-
Results
- The mean age was 61±10 years. Patients with perineural invasion, cartilage invasion, and local invasion exhibited higher PSMA expression scores. Age, tumor differentiation, tumor diameter, perineural invasion, tumor localization, capsular invasion, depth of invasion, surgical margin status, local invasion, nodal metastasis, TNM classification, and stage were similar in high and low PSMA expression groups. There was no PSMA expression in extratumoral vascular stroma. Significantly higher PSMA expression was observed in the vascular endothelium of metastatic lymph nodes compared with reactive lymph nodes. Patients with advanced-stage disease exhibited higher PSMA vascular expression scores compared to those with earlier stages (p<.001). PSMA expression was not correlated with overall survival, disease-specific survival, or disease-free survival (p>.05).
-
Conclusions
- Our study suggests that higher PSMA expression is associated with cartilage invasion, local invasion, and advanced-stage of disease. PSMA expression can be utilized for detection of lymph node metastasis and has some predictive role in cases of neck metastasis.
- Patients and tissue samples
- This study included 51 patients with SCCL who underwent total or partial laryngectomy and neck dissection between January 2010 and January 2020. The hematoxylin and eosin (H&E)-stained sections obtained from all the formalin-fixed paraffin blocks of the patients were re-examined, and appropriate blocks were selected from 17 patients with lymph node metastasis and 34 patients without lymph node metastasis. Neck dissection was performed in patients with clinical and/or radiologic findings suspicious for positive lymph nodes in the neck.
- All cases were histopathologically confirmed according to the 4th edition of the World Health Organization (WHO) classification of head and neck tumors [10]. The Protocol for the Examination of Specimens from Patients with Cancers of the Larynx 2017 of the College of American Pathologists was used to identify histopathologic subtype, tumor location, tumor size, tumor differentiation, tumor spread, surgical margins, lymphovascular invasion, perineural invasion, and lymphatic spread for SCCL [11]. Tumor stage was determined retrospectively for all patients according to the TNM Classification System of the American Joint Committee on Cancer [11]. Data such as clinical information, age, sex, presence of metastasis, and survival data including diseasefree survival (DFS), overall survival (OS), disease-specific survival (DSS), and recurrence were obtained from the hospital database.
- Immunohistochemistry
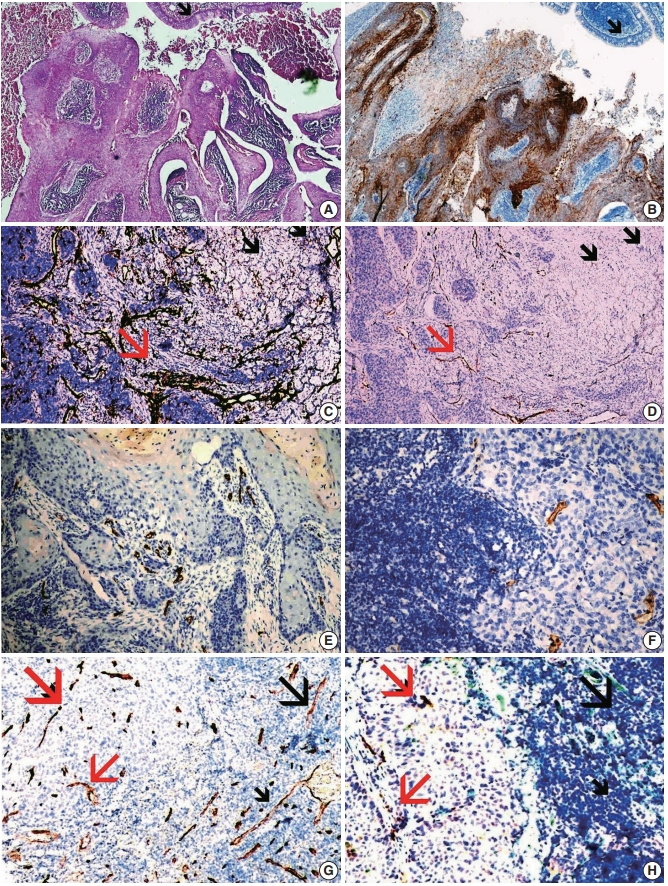
- PSMA antibodies were applied to the blocks that represented tumors, and blocks were selected from metastatic lymph nodes or tumor-negative lymph nodes in the absence of metastatic lymph nodes using an immunohistochemical method in the H&E-stained sections (Fig. 1A). PSMA antibodies (clone 3E6, isotype: IgG1, kappa, DAKO flex ready-to-use monoclonal mouse antibody (Carpinteria, CA, USA) provided in liquid form in a buffer containing stabilizing protein and 0.015 mol/L sodium azide) were prepared according to the manufacturer’s instructions as expressed in the datasheet. The tissue samples were processed together with prostate tissue samples as an antibody-positive control and a negative control in an automated immunohistochemistry device.
- Evaluation of immunohistochemical staining
- Immunohistochemically stained slides were evaluated by two pathologists who were experienced in head and neck pathology, with each being blinded to the cases. PSMA immunohistochemically stained slides were examined under a light microscope and accepted as having positive cytoplasmic staining and/or positive cytoplasmic membrane staining.
- The percentage of vascular endothelial cells that stained positive for PSMA was stratified as: 0, 0%–5%; 1, 6%–25%; 2, 26%–50%; and 3, >50%. The intensity score was stratified as: 1, weak; 2, moderate; and 3, strong. PSMA expression was scored according to the intensity of the tumor epithelium as: 1, none-weak; 2, moderate; and 3, strong. Final PSMA expression was determined by multiplying intensity and percentage scores. The cases were grouped according to stage and lymph node metastasis. The groups were compared by PSMA expression scores [12,13].
- Statistical analysis
- The normality of continuous data distribution was tested using the Kolmogorov-Smirnov test or the Shapiro-Wilk test. Continuous data were compared using the independent sample t test or the Mann-Whitney U test. Categorical data were compared using Pearson’s chi-square test. Fisher’s exact test was used when expected value problems occurred. Kaplan-Meier survival analysis was conducted to predict survival estimates according to PSMA expression score. Receiver operator curve (ROC) analysis was performed to determine the cut off value for PSMA expression in assessing the event of death during follow-up. Patients were classified into two groups according to cut off value as high and low expression of PSMA. A p-value<.05 was regarded as statistically significant. The SPSS ver. 21 software package (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
MATERIALS AND METHODS
- All but one patient were male (98%). The mean age was 61±10 years. Of the primary tumors, 37.3%, 43.1%, and 19.6% were well-differentiated, moderately differentiated, and poorly differentiated, respectively. Fifty (29.4%), 12 (23.5%), one (2%), six (11.8%), eight (15.7%), and nine (17.6%) tumors were located in the supraglottic, glottic, infraglottic, supraglottic+glottic, glottic+infraglottic, and transglottic regions, respectively. Table 1 shows the demographic data of the patients. Age was similar between the high and low vascular expression groups. Tumor differentiation was similar between the high and low vascular expression score groups. Tumor diameter and perineural invasion was similar between the groups. Supraglottic localization was more frequent in the low vascular score group compared to the high group. Transglottic localization was more frequent in the high vascular score group. Capsular invasion, depth of invasion, lymphovascular invasion, surgical margin positivity, and local spread nodal metastasis were similar between the groups. The presence of T4 tumors and stage 4 disease was more frequent in the high vascular PSMA expression group. Comparison of the high and low vascular PSMA expression groups is shown in Table 2.
- We evaluated the expression of PSMA in tumoral epithelium and divided the patients according to expression levels. Age, tumor differentiation, tumor diameter, perineural invasion, tumor localization, capsular invasion, depth of invasion, surgical margin status, local invasion, nodal metastasis, TNM classification, and stage were similar in the high and low intratumoral PSMA expression groups. PSMA expression in tumoral epithelium is shown in Table 3.
- ROC analysis revealed that PSMA was a significant marker of death. A PSMA cut off value of 3 exhibited the highest sensitivity and specificity (area under the curve, 0.705; sensitivity, 81%; specificity, 51%). Patients were divided into two groups according to PSMA expression as high (≥3) and low (<3).
- PSMA expression in the vascular epithelium of lymphatic metastasis was significantly higher compared with that in patients with tumor-negative lymph nodes (p<.001) (Table 4). Most patients with lymphatic metastasis exhibited higher primary tumoral PSMA expression. However, no significant difference was found between patients with and without lymph node metastasis in terms of PSMA expression.
- A higher vascular expression score of PSMA was observed in pT4 tumors. Similarly, higher vascular PSMA scores were observed in stage 4 tumors. No significant correlation with pN was detected for PSMA score.
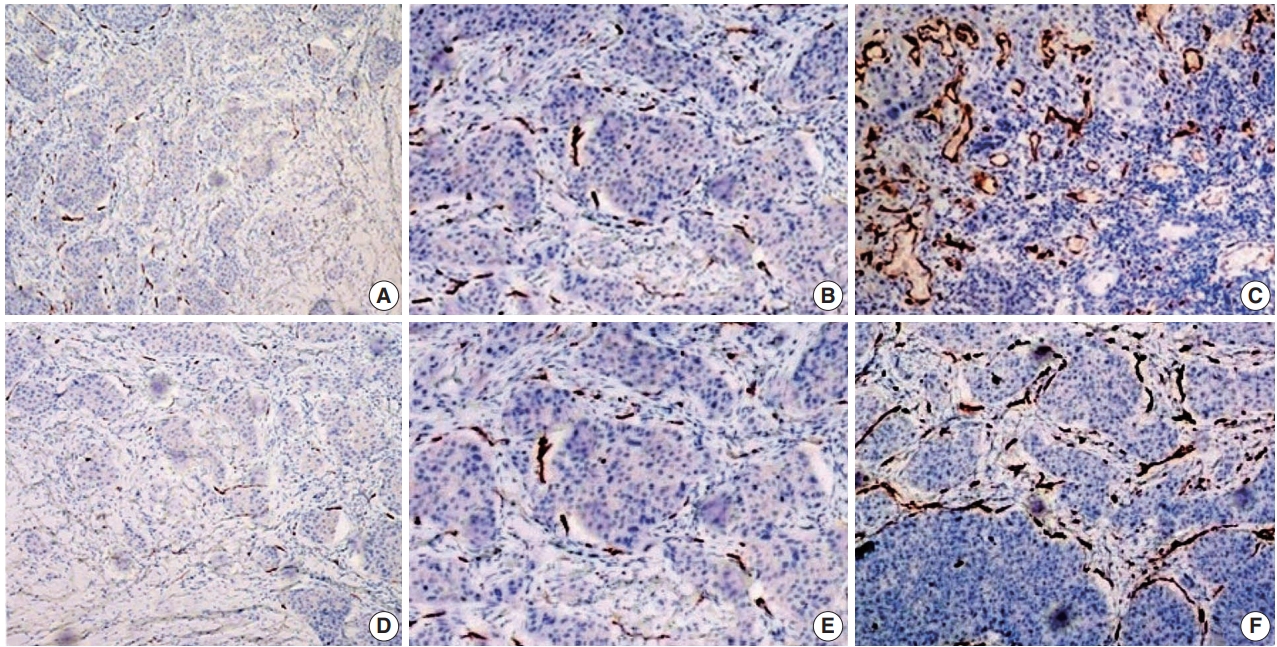
- PSMA expression in the epithelium of the primary SCCL is shown in Fig. 1B. Staining with CD34 demonstrated the difference between normal and tumoral vessels as shown in Fig. 1C. PSMA expression in the vessels of the tumoral stroma are shown on Fig. 1D. PSMA expression in the vessels of a primary tumor (Fig. 1E) and PSMA expression in the vessel cells of the metastatic focus are shown in Fig. 1F. CD31 expression in stromal vessels of the metastatic focus and non-metastatic focus of the same lymph node are shown in Fig. 1G, and PSMA expression in the stromal vessels of the metastatic focus are shown in Fig. 1H. The intratumoral vascular PSMA percentage scores are shown in Fig. 2A–C. Intratumoral PSMA intensity scores are shown in Fig. 2D–F.
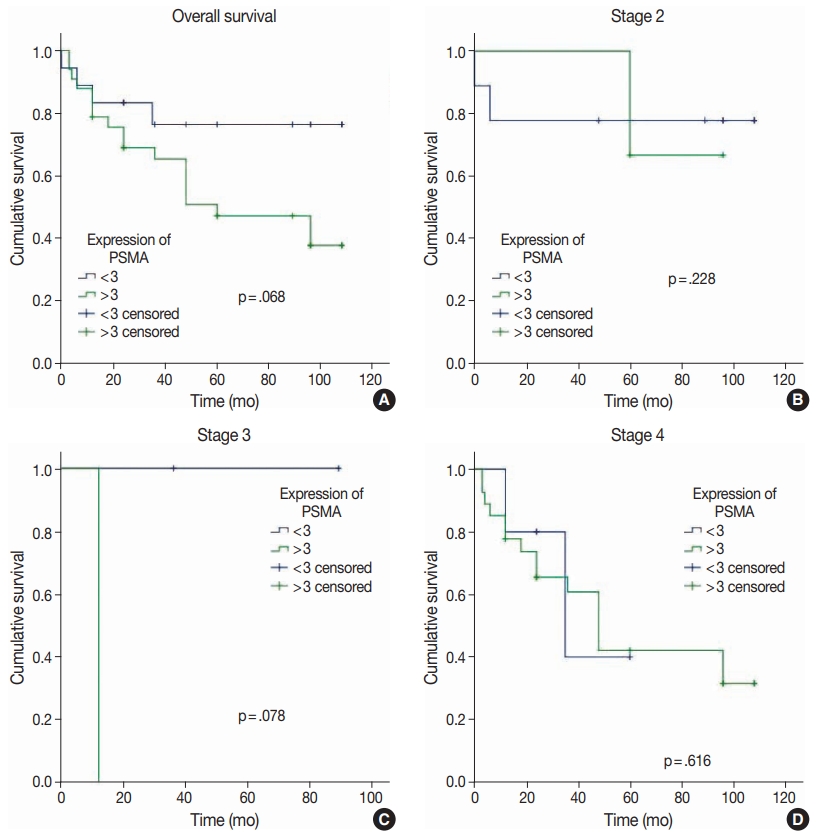
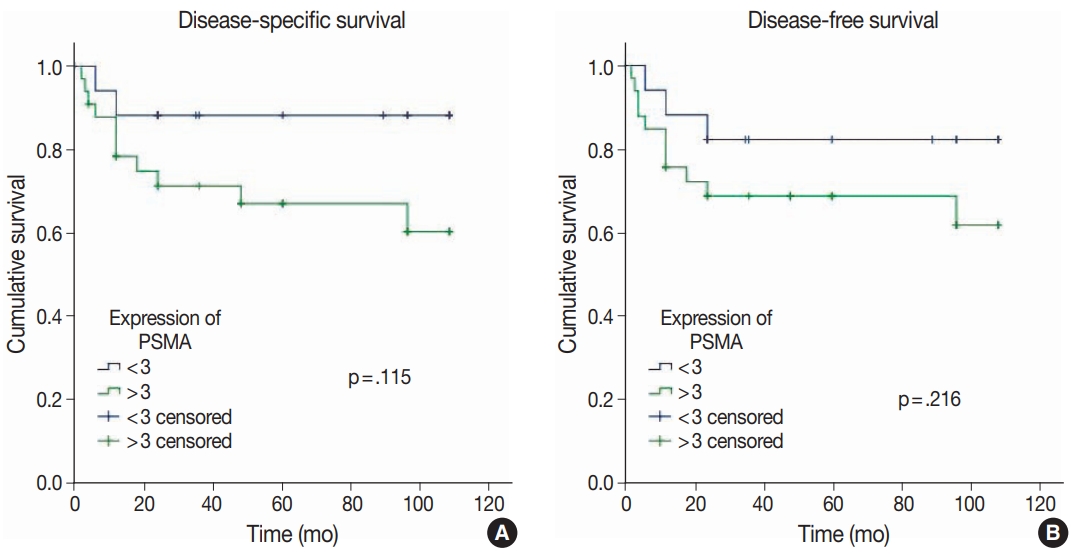
- No distant organ metastasis was detected in any of the cases. Vascular PSMA expression in metastatic lymph nodes and primary tumors was similar (p=.383). No significant correlation was detected between PSMA expression scores in the tumoral vessels and OS, DSS, and DFS (p>.05) (Figs. 3, 4).
RESULTS
- We separately analyzed the expression of PSMA in the stroma of primary tumors, metastatic lymph nodes, non-metastatic lymph nodes, vascular endothelium in the stroma of extratumoral foci, and tumoral epithelium of SCCLs. Many studies have evaluated PSMA expression in intratumoral neovascularized foci [9,14-16]. However, no study has reported PSMA expression in SCCL, and we also compared PSMA expression in metastatic lymph nodes and vascular endothelium in the primary tumoral stroma.
- Abnormal stromal cells and neovascularized dysfunctional angiogenic vessels continuously contribute to the microenvironment of the tumor. Certain cancer types that metastasize through hematogenous and lymphatic patterns were reported to be affected by tumor neovascularization [17]. The metastasis, growth, and progression of solid tumors require angiogenesis. In addition to tumoral nutrition, angiogenesis plays an important role in obtaining treatment responsiveness from chemoradiotherapy depending on the quality of the intratumoral vessels. Therefore, a balance between pro- and anti-angiogenic factors should be established [18]. Our study included patients with SCCL who underwent cervical lymph node dissection, and metastatic lymph nodes were detected in 17 of 51 patients, about one-third of the cases.
- Angiogenesis is crucial in tumor metastasis [19]. In this respect, it is proposed that antiangiogenic treatment will be of importance in treatment of tumor metastases in the future [20]. In our study, none of the cases exhibited diffuse strong staining with PSMA in the extratumoral normal vascular structures. New investigations of PSMA-ligated treatment strategies could be attempted in cases of advanced tumors when surgical treatment options are impossible.
- A proangiogenic microenvironment is considered to increase lymphatic metastatic risk. Even though the 5-year survival rate is commonly high in patients with low T-category and without metastatic lymph nodes, detection of high vascular endothelial growth factor (VEGF) expression has been interpreted to be high risk for poor prognosis and recurrence. Therefore, it is anticipated that these patient groups will benefit from targeted treatment modalities [20]. In our study, the percentage and intensity scores of PSMA expression in intratumoral vessels were significantly high in cases with advanced T-category. PSMA expression scores were 0 and 1 in vessels with a non-metastatic focus in lymph nodes that maintained normal lymph node morphology, whereas PSMA expression scores were significantly higher at scores 2 and 3 in neovascularized vessels in metastatic foci. Therefore, PSMA seems to be a new key factor in the specific target-oriented treatment of both primary tumors and lymph node metastatic foci, but further studies are necessary to confirm this hypothesis.
- A significant level of VEGF expression was encountered, whereas no expression was detected in intratumoral stromal cells in another study that investigated the relationship of VEGF expression with angiogenesis in SCCL. Those authors concluded that progression of SCC was compliant with VEGF expression [21]. By contrast, in another study, no correlation was observed between prognosis and angiogenesis in SCCL [22]. In our study, PSMA expression in tumoral vascular endothelium was associated with poor clinical parameters including cartilage invasion, local invasion, and advanced-stage disease.
- PSMA positivity was observed in 151 of 779 tumors in a study that evaluated PSMA expression in bone and soft tissue tumors in tumor-associated vascular structures. A higher concentration of PSMA expression was observed in high-grade tumors compared to intermediate and low-grade tumors. However, it was reported that false-negative expression might be present because a tissue microarray system was used in the study [23]. Similarly, in another study, it was reported that neovascular PSMA expression was significantly higher in malignant tumors of the thyroid gland compared to benign lesions, and that expression rates increased in poorly differentiated and undifferentiated tumors [24]. In our study, we identified no correlation between PSMA expression score and differentiation of SCCL.
- Our study showed that the intensity and percentage scores of PSMA expression in the vascular endothelium of primary tumor stroma were significantly higher in cases with cartilage and local tumor invasion. It was additionally noted that PSMA expression scores were significantly high with scores 2 and 3 in the intratumoral vessels of pT4 tumors. However, we found no correlation between the expression scores of PSMA in intratumoral vessels and OS, DSS, and DFS.
- Specific target-oriented molecular therapies present a crucial necessity for treatment of tumor-associated vessels [25]. Vascular PSMA expression was determined to be correlated with several cancer types with respect to clinicopathologic and prognostic features. No PSMA expression was identified in 24 of 96 patients with SCC of the oral cavity, whereas PSMA expression was observed in less and more than 50% of tumor-associated vessels in 24 and 24 cases, respectively. Therefore, high vascular expression of PSMA was correlated with poor prognosis in oral SCC [13]. Vascular PSMA expression was correlated with the Ki67 proliferation index, which has prognostic importance in breast cancer [12]. PSMA expression in the vascular endothelium was determined to be significantly correlated with TNM, the Ki67 proliferation index, tumor differentiation, and positivity of lymph node metastasis in 103 patients with hepatocellular carcinoma [25]. Similarly, PSMA expression has been evaluated in gynecologic cancers and was encountered in the neovascular foci of specific and high-grade tumors in endometrial, ovarian, and cervical SCC, while vulval SCC exhibited no such phenomenon [13].
- PSMA expression was identified in tumor-associated vessels in 46% (31/68) of patients with breast cancer and metastasis [16]. The relationship of PSMA expression with distant organ metastasis could not be analyzed in our study because no distant organ metastasis was present in any of our patients.
- Early diagnosis and treatment of tumors are important to avoid surgery with high comorbidity for patients such as laryngectomy. Researchers have found that the use of nitric oxide synthase blockers is a promising tool in the scope of antiangiogenic therapy in SCCL [26]. Similarly, PSMA can be considered a target in early-stage tumors because it exhibits specific expression in the vessels of the neoplastic foci.
- The limitation of this study was that our study was retrospective, observational, and included patients who underwent neck dissection for SCCL, limiting the number of cases. Heterogeneity of sex was another limitation, which was caused by the male dominance of larynx tumors. In our study, there was only one female patient. Therefore, the relationship between expression of PSMA and sex could not be evaluated. Our study included patients that were followed for a period between 12 and 120 months. The survival analysis revealed no difference between the groups in terms of PSMA expression. However, this might be due to the limited follow-up of the patients that were included in the study in recent years.
- Both proangiogenetic and antiangiogenetic drugs will be introduced in the near future as alternative treatment options to suppress tumor blood circulation and halt tumor progression [24]. Numerous preclinical animal studies and case reports of patients with cancer have supported the validity of antiangiogenic therapy [27-29]. The rapidly increasing amount of information on tumor angiogenesis, current information on the biologic behavior of cancer, and implementation of imaging studies to display clinical interventions and tumoral vascularity support antiangiogenic therapy as a new treatment method by facilitating its development. Novel developments will be achieved using innovative molecular analysis technologies to display neovascularization using imaging techniques such as positron emission tomography, computed tomography and magnetic resonance imaging to confirm tumor mass. We anticipate that PSMA will be used as a target of alternative or adjuvant treatment options to surgical procedures for treatment of cancer and metastases. However, this anticipation will only be realized with further prospective studies.
- PSMA expression in tumoral vascular endothelium was associated with poor clinical parameters including cartilage invasion, local invasion, and advanced stage. PSMA expression can be used for detection of lymph node metastasis. PSMA seems to be a mediator for novel diagnostic and treatment options in the targeted therapy of advanced-stage laryngeal tumors and their metastases.
DISCUSSION
Ethics Statement
The study protocol was approved by the institutional review board (258-11.09.2020). The study was designed as a retrospective study; therefore, informed consent was not obtained from the patients.
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author Contributions
Conceptualization: GE, HY, MES. Data curation: YÇK, MD, GE. Formal analysis: HY, MES. Funding acquisition: GE. Investigation and evaluation of slides: GE, MD. Methodology: GE, HY, MES, YÇK, MD. Supervision: GE. Validation: GE, HY, MES, YÇK, MD. Writing—original draft: GE, HY, MES, YÇK. Writing—review & editing: GE, HY, MES. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
This study was funded by The Coordinatorship of Scientific Research Projects Department (BAP), Süleyman Demirel University by the number of TSG-2020-8134.
| Lymph node | Score 0 | Score 1 | Score 2 | Score 3 | p-value |
|---|---|---|---|---|---|
| Reactive lymph node | 21 (61.8) | 13 (38.2) | 0 | 0 | < .001 |
| Metastatic lymph node | 0 | 2 (11.8) | 9 (52.9) | 6 (35.3) |
- 1. Nocini R, Molteni G, Mattiuzzi C, Lippi G. Updates on larynx cancer epidemiology. Chin J Cancer Res 2020; 32: 18-25. ArticlePubMedPMC
- 2. Prince A, Aguirre-Ghizo J, Genden E, Posner M, Sikora A. Head and neck squamous cell carcinoma: new translational therapies. Mt Sinai J Med 2010; 77: 684-99. ArticlePubMedPDF
- 3. Rieger J, Kaessmeyer S, Al Masri S, Hunigen H, Plendl J. Endothelial cells and angiogenesis in the horse in health and disease: a review. Anat Histol Embryol 2020; 49: 656-78. ArticlePubMedPDF
- 4. Beatrice F, Valente G, Cammarota R, et al. Laryngeal cancer and angiogenesis. Acta Otorhinolaryngol Ital 1996; 16: 355-62. PubMed
- 5. Chen X, Liang R, Zhu X. Anti-EGFR therapies in nasopharyngeal carcinoma. Biomed Pharmacother 2020; 131: 110649.ArticlePubMed
- 6. de Vries LH, Lodewijk L, Braat A, et al. (68)Ga-PSMA PET/CT in radioactive iodine-refractory differentiated thyroid cancer and first treatment results with (177)Lu-PSMA-617. EJNMMI Res 2020; 10: 18.PubMedPMCPDF
- 7. Rowe SP, Gorin MA, Pomper MG. Imaging of prostate-specific membrane antigen using [(18)F]DCFPyL. PET Clin 2017; 12: 289-96. ArticlePubMed
- 8. Bradbury R, Jiang WG, Cui YX. The clinical and therapeutic uses of MDM2 and PSMA and their potential interaction in aggressive cancers. Biomark Med 2015; 9: 1353-70. ArticlePubMed
- 9. Van de Wiele C, Sathekge M, de Spiegeleer B, et al. PSMA expression on neovasculature of solid tumors. Histol Histopathol 2020; 35: 919-27. PubMed
- 10. Gale N, Poljak M, Zidar N. Update from the 4th Edition of the World Health Organization classification of head and neck tumours: what is new in the 2017 WHO blue book for tumours of the hypopharynx, larynx, trachea and parapharyngeal space. Head Neck Pathol 2017; 11: 23-32. ArticlePubMedPMCPDF
- 11. Seethala RR, Weinreb I, Bullock MJ, et al. Protocol for the examination of specimens from patients with carcinomas of the larynx. Northfield: College of American Pathologists, 2019.
- 12. Wernicke AG, Varma S, Greenwood EA, et al. Prostate-specific membrane antigen expression in tumor-associated vasculature of breast cancers. APMIS 2014; 122: 482-9. ArticlePubMed
- 13. Wernicke AG, Kim S, Liu H, Bander NH, Pirog EC. Prostate-specific membrane antigen (PSMA) expression in the neovasculature of gynecologic malignancies: implications for PSMA-targeted therapy. Appl Immunohistochem Mol Morphol 2017; 25: 271-6. ArticlePubMed
- 14. Haffner MC, Laimer J, Chaux A, et al. High expression of prostatespecific membrane antigen in the tumor-associated neo-vasculature is associated with worse prognosis in squamous cell carcinoma of the oral cavity. Mod Pathol 2012; 25: 1079-85. ArticlePubMedPDF
- 15. Silver DA, Pellicer I, Fair WR, Heston WD, Cordon-Cardo C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin Cancer Res 1997; 3: 81-5. PubMed
- 16. Kasoha M, Unger C, Solomayer EF, et al. Prostate-specific membrane antigen (PSMA) expression in breast cancer and its metastases. Clin Exp Metastasis 2017; 34: 479-90. ArticlePubMedPDF
- 17. Lin PP. Aneuploid circulating tumor-derived endothelial cell (CTEC): a novel versatile player in tumor neovascularization and cancer metastasis. Cells 2020; 9: 1539.ArticlePubMedPMC
- 18. Butkiewicz D, Gdowicz-Klosok A, Krzesniak M, et al. Association of genetic variants in ANGPT/TEK and VEGF/VEGFR with progression and survival in head and neck squamous cell carcinoma treated with radiotherapy or radiochemotherapy. Cancers (Basel) 2020; 12: 1506.ArticlePubMedPMC
- 19. Kupisz K, Chibowski D, Klatka J, Klonowski S, Stepulak A. Tumor angiogenesis in patients with laryngeal cancer. Eur Arch Otorhinolaryngol 1999; 256: 303-5. ArticlePubMedPDF
- 20. Schluter A, Weller P, Kanaan O, et al. CD31 and VEGF are prognostic biomarkers in early-stage, but not in late-stage, laryngeal squamous cell carcinoma. BMC Cancer 2018; 18: 272.PubMedPMCPDF
- 21. Sawatsubashi M, Yamada T, Fukushima N, Mizokami H, Tokunaga O, Shin T. Association of vascular endothelial growth factor and mast cells with angiogenesis in laryngeal squamous cell carcinoma. Virchows Arch 2000; 436: 243-8. ArticlePubMedPDF
- 22. Rodrigo JP, Cabanillas R, Chiara MD, Garcia Pedrero J, Astudillo A, Suarez Nieto C. Prognostic significance of angiogenesis in surgically treated supraglottic squamous cell carcinomas of the larynx. Acta Otorrinolaringol Esp 2009; 60: 272-7. ArticlePubMed
- 23. Heitkotter B, Trautmann M, Grunewald I, et al. Expression of PSMA in tumor neovasculature of high grade sarcomas including synovial sarcoma, rhabdomyosarcoma, undifferentiated sarcoma and MPNST. Oncotarget 2017; 8: 4268-76. ArticlePubMedPMC
- 24. Heitkotter B, Steinestel K, Trautmann M, et al. Neovascular PSMA expression is a common feature in malignant neoplasms of the thyroid. Oncotarget 2018; 9: 9867-74. ArticlePubMedPMC
- 25. Jiao D, Li Y, Yang F, et al. Expression of prostate-specific membrane antigen in tumor-associated vasculature predicts poor prognosis in hepatocellular carcinoma. Clin Transl Gastroenterol 2019; 10: 1-7. ArticlePubMedPMC
- 26. Franchi A, Gallo O, Paglierani M, et al. Inducible nitric oxide synthase expression in laryngeal neoplasia: correlation with angiogenesis. Head Neck 2002; 24: 16-23. ArticlePubMed
- 27. White CW, Sondheimer HM, Crouch EC, Wilson H, Fan LL. Treatment of pulmonary hemangiomatosis with recombinant interferon alfa-2a. N Engl J Med 1989; 320: 1197-200. ArticlePubMed
- 28. Folkman J. Seminars in Medicine of the Beth Israel Hospital, Boston. Clinical applications of research on angiogenesis. N Engl J Med 1995; 333: 1757-63. ArticlePubMed
- 29. Eisen T, Boshoff C, Mak I, et al. Continuous low dose thalidomide: a phase II study in advanced melanoma, renal cell, ovarian and breast cancer. Br J Cancer 2000; 82: 812-7. ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Concomitant laryngeal squamous cell carcinoma and prostate cancer on 18F-FDG PET/CT and 18F-PSMA-1007 PET/CT
Yongzhu Pu, Ran Xie, Zhiyong Deng, Long Chen
European Journal of Nuclear Medicine and Molecular Imaging.2025;[Epub] CrossRef - A Practical Guide to the Pearls and Pitfalls of PSMA PET Imaging
Andrew F. Voter, Rudolf A. Werner, Hatice Savas, Andrei Gafita, Ashley E. Ross, Michael A. Gorin, Lilja B. Solnes, Martin G. Pomper, Steven P. Rowe, Sara Sheikhbahaei
Seminars in Nuclear Medicine.2024; 54(1): 119. CrossRef - p53 and PTEN expression evaluation with molecular evident recent criteria in laryngeal carcinoma
Ayca Tan, Gorkem Eskiizmir, Ugur Kamiloglu, Sulen Sarioglu
Medicine.2023; 102(19): e33676. CrossRef - Diagnostic, Prognostic, and Therapeutic Role for Angiogenesis Markers in Head and Neck Squamous Cell Carcinoma: A Narrative Review
Lara Alessandrini, Laura Astolfi, Antonio Daloiso, Marta Sbaraglia, Tiziana Mondello, Elisabetta Zanoletti, Leonardo Franz, Gino Marioni
International Journal of Molecular Sciences.2023; 24(13): 10733. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
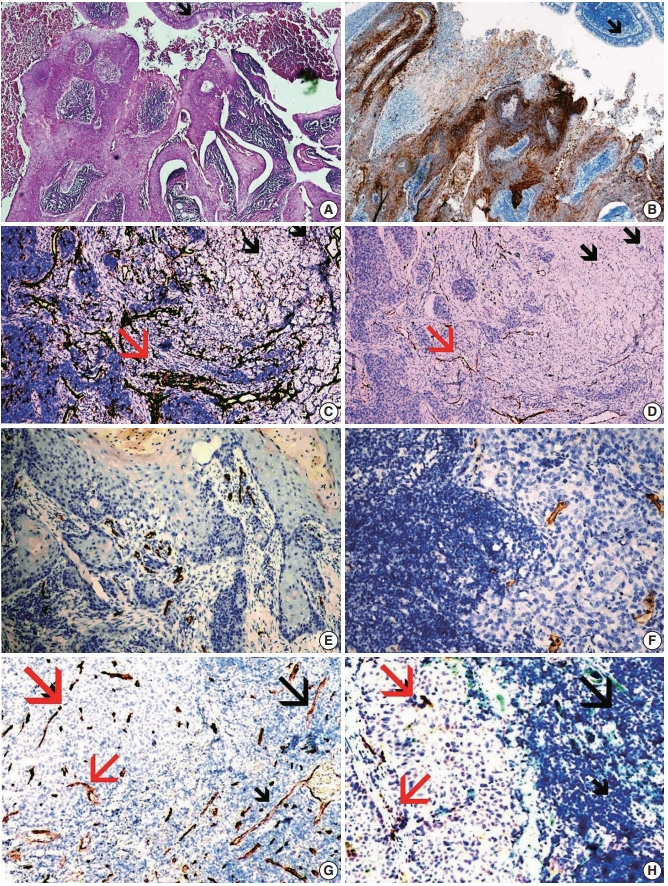
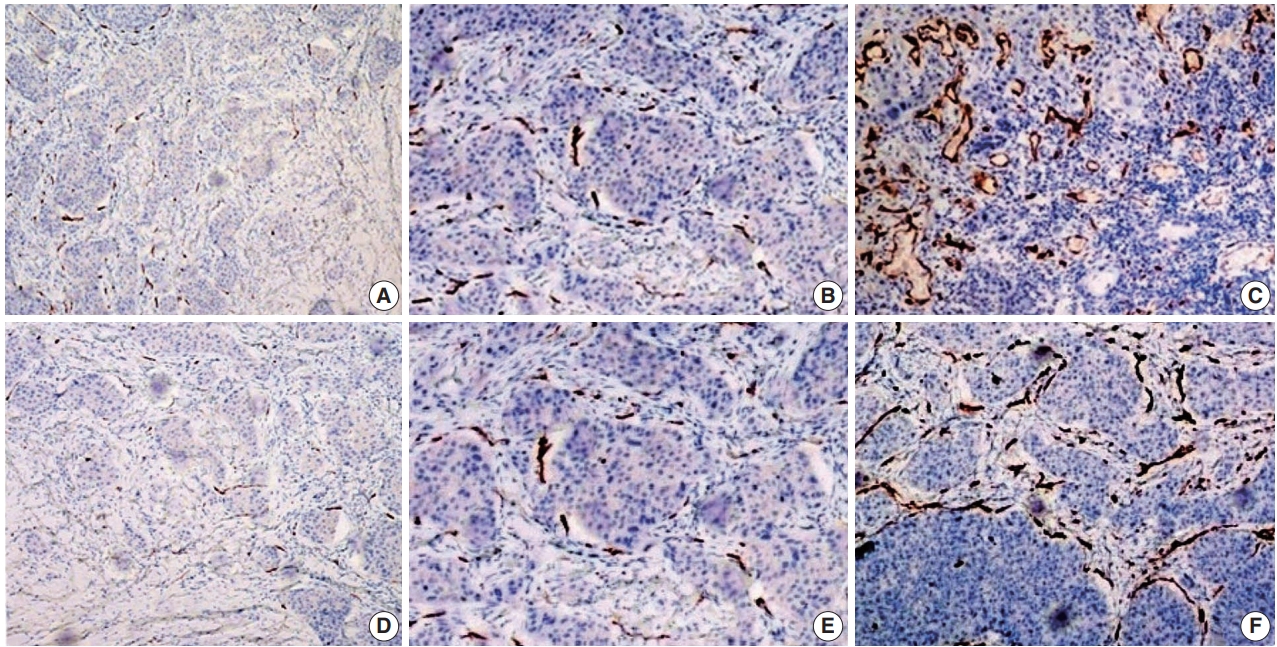
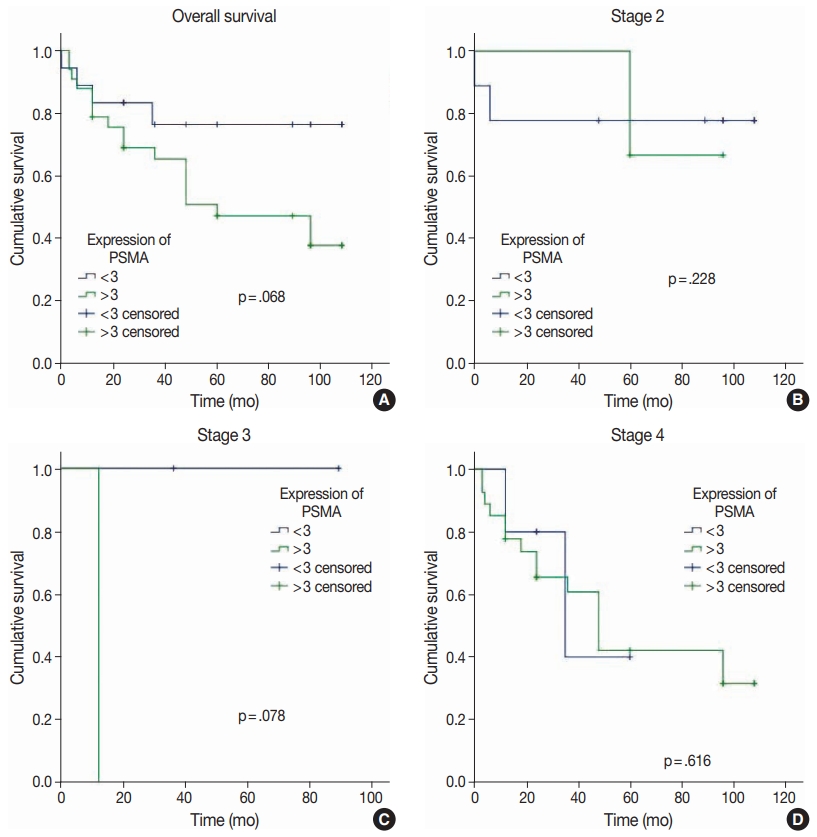
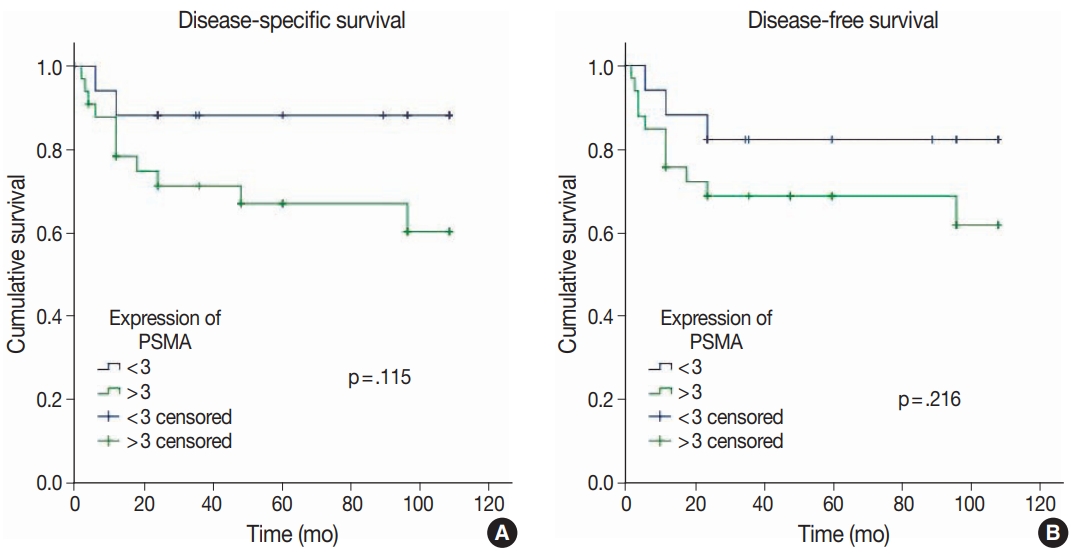




Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
| No. (%) | |
|---|---|
| Age, mean ± SD (yr) | 61 ± 10 |
| Tumor differentiation | |
| Well | 19 (37.3) |
| Moderately | 22 (43.1) |
| Poor | 10 (19.6) |
| Tumor diameter (cm), median (range) | 2.5 (0.6–8.5) |
| Perineural invasion | |
| No | 46 (90.2) |
| Yes | 5 (9.8) |
| Tumor localization | |
| Supraglottic | 15 (29.4) |
| Glottic | 12 (23.5) |
| Infraglottic | 1 (2) |
| Glottic + supraglottic | 6 (11.8) |
| Glottic + infraglottic | 8 (15.7) |
| Transglottic | 9 (17.6) |
| Capsular invasion | |
| No | 44 (86.3) |
| Yes | 7 (13.7) |
| Depth of invasion, mean ± SD, cm | 1.3 ± 0.9 |
| Lymphovascular invasion | |
| No | 42 (82.4) |
| Yes | 9 (17.6) |
| Cartilage invasion | |
| No | 19 (37.3) |
| Yes | 32 (62.7) |
| Surgical margin | |
| No | 48 (94.1) |
| Yes | 3 (5.9) |
| Soft tissue invasion | |
| No | 28 (54.9) |
| Yes | 23 (45.1) |
| T category | |
| 1 | 6 (11.8) |
| 2 | 14 (27.5) |
| 3 | 6 (11.8) |
| 4 | 25 (49) |
| N category | |
| 0 | 32 (62.7) |
| 1 | 5 (9.8) |
| 2 | 5 (9.8) |
| 3 | 9 (17.6) |
| Stage | |
| 1 | 4 (7.8) |
| 2 | 12 (23.1) |
| 3 | 3 (5.9) |
| 4 | 32 (62.7) |
| PSMA score < 3 (%) | PSMA score ≥ 3 (%) | p-value | |
|---|---|---|---|
| Age (yr) | 61 ± 12 | 60 ± 9 | .844 |
| Tumor differentiation | |||
| Well | 8 (44.4) | 11 (33.3) | .744 |
| Moderately | 6 (33.3) | 16 (48.5) | |
| Poor | 4 (22.2) | 6 (18.2) | |
| Tumor diameter (cm) | 2.5 ± 1.6 | 3 ± 1.6 | .367 |
| Perineural invasion | |||
| No | 18 (100) | 28 (84.8) | .148 |
| Yes | 0 | 5 (15.2) | |
| Tumor localization | |||
| Supraglottic | 9 (50) | 6 (18.2) | .017 |
| Glottic | 4 (22.2) | 8 (24.2) | > .99 |
| Infraglottic | 0 | 1 (3.0) | > .99 |
| Glottic + supraglottic | 3 (16.7) | 3 (9.1) | .652 |
| Glottic + infraglottic | 2 (11.1) | 6 (18.2) | .696 |
| Transglottic | 0 | 9 (27.3) | .019 |
| Capsular invasion | |||
| No | 17 (94.4) | 27 (81.8) | .398 |
| Yes | 1 (5.6) | 6 (18.2) | |
| Depth of invasion | 1.09 ± 0.9 | 1.4 ± 0.6 | .227 |
| Lymphovascular invasion | |||
| No | 16 (88.9) | 26 (78.8) | .464 |
| Yes | 2 (11.1) | 7 (21.2) | |
| Cartilage invasion | |||
| No | 12 (66.7) | 7 (21.2) | .001 |
| Yes | 6 (33.3) | 26 (78.8) | |
| Surgical margin | |||
| No | 17 (94.4) | 31 (93.9) | >.99 |
| Yes | 1 (5.6) | 2 (6.1) | |
| Soft tissue invasion | |||
| No | 13 (72.2) | 15 (45.5) | .066 |
| Yes | 5 (27.8) | 18 (54.5) | |
| Lymph node metastasis | |||
| No | 14 (77.8) | 19 (57.6) | .149 |
| Yes | 4 (22.2) | 14 (42.4) | |
| T category | |||
| 1 | 3 (16.7) | 3 (9.1) | .652 |
| 2 | 9 (50.0) | 5 (15.2) | .019 |
| 3 | 4 (22.2) | 2 (6.1) | .168 |
| 4 | 2 (11.1) | 23 (69.7) | < .001 |
| N category | |||
| 0 | 14 (77.8) | 18 (54.5) | .135 |
| 1 | 1 (5.6) | 4 (12.1) | .645 |
| 2 | 2 (11.1) | 3 (9.1) | > .99 |
| 3 | 1 (5.6) | 8 (24.2) | .134 |
| Stage | |||
| 1 | 2 (11.1) | 2 (6.1) | .607 |
| 2 | 9 (50.0) | 3 (9.1) | .001 |
| 3 | 2 (11.1) | 1 (3.0) | .282 |
| 4 | 5 (27.8) | 27 (81.8) | < .001 |
| PSMA score < 3 (%) | PSMA score ≥ 3 (%) | p-value | |
|---|---|---|---|
| Age (yr) | 61 ± 10 | 60 ± 10 | .823 |
| Tumor differentiation | |||
| Well | 18 (41.9) | 1 (12.5) | |
| Moderately | 17 (39.5) | 5 (62.5) | .210 |
| Poor | 8 (18.6) | 2 (25.0) | |
| Tumor diameter (cm) | 2.8 ± 1.7 | 2.6 ± 1.5 | .736 |
| Perineural invasion | |||
| No | 39 (90.7) | 7 (87.5) | > .99 |
| Yes | 4 (9.3) | 1 (12.5) | |
| Tumor localization | |||
| Supraglottic | 12 (27.9) | 3 (37.5) | .679 |
| Glottic | 12 (27.9) | 0 | .179 |
| Infraglottic | 1 (2.3) | 0 | > .99 |
| Glottic + supraglottic | 5 (11.6) | 1 (12.5) | > .99 |
| Glottic + infraglottic | 5 (11.6) | 3 (37.5) | .099 |
| Transglottic | 8 (18.6) | 1 (12.5) | > .99 |
| Capsular invasion | |||
| No | 36 (83.7) | 8 (100) | .579 |
| Yes | 7 (16.3) | 0 | |
| Depth of invasion | 1.3 ± 0.9 | 1.3 ± 0.9 | .997 |
| Lymphovascular invasion | |||
| No | 35 (81.4) | 7 (87.5) | > .99 |
| Yes | 8 (18.6) | 1 (12.5) | |
| Cartilage invasion | |||
| No | 15 (34.9) | 4 (50.0) | .450 |
| Yes | 28 (65.1) | 4 (50.0) | |
| Surgical margin | |||
| No | 41 (95.3) | 31 (93.9) | > .99 |
| Yes | 2 (4.7) | 2 (6.1) | |
| Soft tissue invasion | |||
| No | 24 (55.8) | 7 (87.5) | .407 |
| Yes | 19 (44.2) | 1 (12.5) | |
| Lymph node metastasis | |||
| No | 27 (62.8) | 6 (75.0) | .696 |
| Yes | 16 (37.2) | 2 (25.0) | |
| T category | |||
| 1 | 6 (14.0) | 0 | .572 |
| 2 | 12 (27.9) | 2 (25.0) | > .99 |
| 3 | 5 (11.6) | 1 (12.5) | > .99 |
| 4 | 20 (46.5) | 5 (62.5) | .465 |
| N category | |||
| 0 | 26 (60.5) | 6 (75.0) | .694 |
| 1 | 3 (7.0) | 2 (25.0) | .170 |
| 2 | 5 (11.6) | 0 | .580 |
| 3 | 9 (20.9) | 0 | .322 |
| Stage | |||
| 1 | 4 (9.3) | 0 | > .99 |
| 2 | 10 (23.3) | 2 (25.0) | > .99 |
| 3 | 2 (4.7) | 1 (12.5) | .407 |
| 4 | 27 (62.8) | 5 (62.5) | > .99 |
| Lymph node | Score 0 | Score 1 | Score 2 | Score 3 | p-value |
|---|---|---|---|---|---|
| Reactive lymph node | 21 (61.8) | 13 (38.2) | 0 | 0 | < .001 |
| Metastatic lymph node | 0 | 2 (11.8) | 9 (52.9) | 6 (35.3) |
SD, standard deviation; T, tumor; N, node.
Values are presented as mean ± SD or number (%). PSMA, prostate-specific membrane antigen; T, tumor; N, node; SD, standard deviation.
Values are presented as mean ± SD or number (%). PSMA, prostate-specific membrane antigen; T, tumor; N, node; SD, standard deviation.
Values are presented as number (%).

