 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Article
- Primary Merkel cell carcinoma of the salivary gland: a clinicopathologic study of four cases with a review of literature
- Gyuheon Choi, Joon Seon Song, Hee Jin Lee, Gi Hwan Kim, Young Ho Jung, Yoon Se Lee, Kyung-Ja Cho
- J Pathol Transl Med. 2025;59(3):171-179. Published online April 30, 2025
- DOI: https://doi.org/10.4132/jptm.2025.03.25
- 5,136 View
- 164 Download
- 1 Crossref
-
 Abstract
Abstract
 PDF
PDF - Background
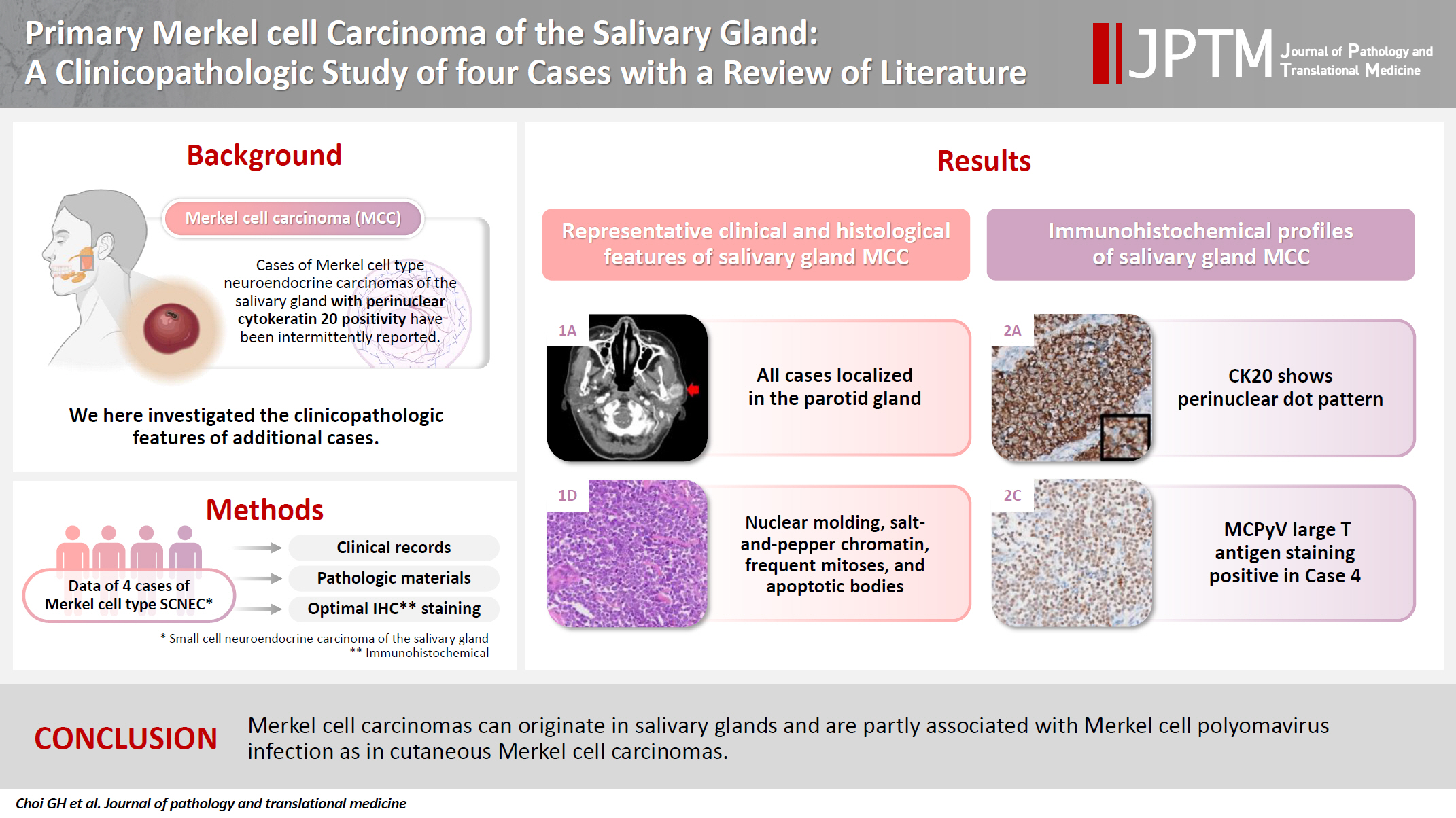
Primary Merkel cell carcinoma of the salivary gland is currently not listed in the World Health Organization classification. However, cases of Merkel cell type neuroendocrine carcinomas of the salivary gland with perinuclear cytokeratin 20 positivity have been intermittently reported. We here investigated the clinicopathologic features of additional cases.
Methods
Data of four cases of Merkel cell type small cell neuroendocrine carcinoma of the salivary gland were retrieved. To confirm the tumors’ primary nature, clinical records and pathologic materials were reviewed. Optimal immunohistochemical staining was performed to support the diagnosis.
Results
All tumors were located in the parotid gland. Possibilities of metastasis were excluded in all cases through a meticulous clinicopathological review. Tumor histology was consistent with the diagnosis of small cell neuroendocrine carcinoma. Tumors’ immunohistochemical phenotypes were consistent with Merkel cell carcinoma, including Merkel cell polyomavirus large T antigen positivity in two of the four cases.
Conclusions
Merkel cell carcinomas can originate in salivary glands and are partly associated with Merkel cell polyomavirus infection as in cutaneous Merkel cell carcinomas. -
Citations
Citations to this article as recorded by
- Parotid intranodal metastasis of Merkel cell carcinoma: a rare case report
Tong Gao, Dengshun Wang, Hongwei Yu, Yu’e Wang, Haibin Lu
BMC Oral Health.2025;[Epub] CrossRef
- Parotid intranodal metastasis of Merkel cell carcinoma: a rare case report
Brief Case Report
- A Ciliated Cyst with Müllerian Differentiation Arising in the Posterior Mediastinum
- So Jung Lee, Chung Su Hwang, Do Youn Park, Gi Young Huh, Chang Hun Lee
- Korean J Pathol. 2014;48(5):401-404. Published online October 27, 2014
- DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.5.401
- 10,388 View
- 82 Download
- 11 Crossref
-
PDF
-
Citations
Citations to this article as recorded by- Rare Posterior Mediastinal Müllerian Cyst Resected by VATS: Case Report and Literature Review
Małgorzata Edyta Wojtyś, Wiktoria Skórka, Miłosz Podsiadło, Konrad Ptaszyński, Katarzyna Rodak, Dominik Jakubowski, Tomasz Grodzki
Journal of Clinical Medicine.2026; 15(7): 2773. CrossRef - Cyst of Hattori: literature review and case presentation
R. B. Berdnikov, K. A. Andryuschenko, N. S. Zavarov, E. M. Petrunina, A. V. Bazhenov, A. S. Romakhin
PULMONOLOGIYA.2025; 35(4): 553. CrossRef - Cyst of Hattori: A Rare Cyst in the Posterior Mediastinum
Matthew D. Turner, Elicia Goodale, Barry C. Gibney, Maria Cecilia D. Reyes
International Journal of Surgical Pathology.2023; 31(4): 431. CrossRef - A large retroperitoneal Mullerian cyst: case report and review of the literature
Elena Parmentier, Jody Valk, Paul Willemsen, Caroline Mattelaer
Acta Chirurgica Belgica.2021; 121(4): 278. CrossRef - A case of resected Mullerian cyst in posterior mediastinum
Yoshiyuki Susaki, Noriyoshi Sawabata
The Journal of the Japanese Association for Chest Surgery.2020; 34(2): 137. CrossRef - Serosal Inclusion Cysts and Arteriovenous Fistulas in Paraprostatic Area of a Dog
Daisuke KOJIMA, Kyoko KOJIMA, Kazumi OTA, Yoshihiko KOJIMA
Journal of the Japan Veterinary Medical Association.2020; 73(9): 511. CrossRef - A surgical case of Mullerian cyst in the posterior mediastinum
Yusuke Kita, Yoshimasa Tokunaga, Taku Okamoto
The Journal of the Japanese Association for Chest Surgery.2019; 33(1): 68. CrossRef - CT and MRI characteristics for differentiating mediastinal Müllerian cysts from bronchogenic cysts
M. Kawaguchi, H. Kato, A. Hara, N. Suzui, H. Tomita, T. Miyazaki, H. Iwata, M. Matsuo
Clinical Radiology.2019; 74(12): 976.e19. CrossRef - A case of Mullerian cyst arising in the posterior mediastinum
Masahiro Adachi, Isao Sano, Shintaro Hashimoto, Ryoichiro Doi, Hideki Taniguchi, Kazuto Shigematsu
The Journal of the Japanese Association for Chest Surgery.2018; 32(6): 713. CrossRef - Two resected cases of Mullerian cyst in the posterior mediastinum
Shotaro Hashimoto, Masato Hisano, Masato Morimoto
The Journal of the Japanese Association for Chest Surgery.2018; 32(7): 818. CrossRef - Posterior mediastinal Müllerian cyst: a rare cause of pain in a young woman
Rebecca Weedle, Keith Conway, Igor Saftic, Alan Soo
Asian Cardiovascular and Thoracic Annals.2017; 25(6): 466. CrossRef
- Rare Posterior Mediastinal Müllerian Cyst Resected by VATS: Case Report and Literature Review
Original Article
- Composite Tumor of Adenocarcinoma and Small Cell Neuroendocrine Carcinoma of the Uterine Cervix: A Case Report.
- Hye Rim Park, Yong Woo Lee, Young Euy Park
- J Pathol Transl Med. 1990;1(1):111-120.
- 2,801 View
- 45 Download
-
Abstract
PDF
- Small cell neuroendocrine carcinoma of the uterine cervix is a distinct subtype of cervical cancer that appears analogous to oat cell carcinoma and carcinoid tumors of the lung. It has been assumed to be derived from the neural crest via argyrophilic cells in the normal endocervix. We have recently encountered a case of small cell neuroendocrine carcinoma of the uterine cervix coexisting with adenocarcinoma which was argyrophil negative. A 66-year-old multiparous woman was admitted because of vaginal bleeding for 2 months. Cervicovaginal smear revealed several scattered clusters and sheets of monotonous small cells with some peripheral palisading in the background of hemorrhage and necrosis. Radical hysterectomy specimen revealed and ulcerofungating tumor on endocervical canal which was composed of two components. Major component of the tumor was made up of monomorphic population of small oval-shaped tumor cells arranged in sheets and partly in acinar structeres or trabecular fashion. Other component was adenocarcinoma, endocervical well-differentiated type. Argyropilia was present on the Grimelius stain and immunohistochemical studies revealed diffuse positivity to neuron-specific enolase and carcinoembryonic antigen. Electron microscopic examination showed clusters of small round to oval cells, which had a few well-formed desmosomes and several membrane-bound, dense-core neurosectetory granules.
Case Reports
- Urinary Cytologic Findings of Small Cell Neuroendocrine Carcinoma: A Case Report.
- Dong Hoon Kim, Dong Wook Kang, Kyung Hee Kim, Ju Heon Kim, Mee Ja Park
- J Pathol Transl Med. 2002;13(2):78-83.
- 2,222 View
- 20 Download
-
Abstract
PDF
- We report the cytologic features of a case of primary small cell carcinoma of the urinary bladder with high grade transitional cell and signet ring cell carcinomatous components. A 64-year-old male presented with gross hematuria for one week. Computed tomography revealed an ill-defined mass in the left lateral wall of the urinary bladder. Urinary cytology showed hypercellularity with predominantly isolated single cells and clustered cells. They have scanty cytoplasm and naked hyperchromatic nuclei with finely granular nuclear chromatin and rare nucleoli. The tumor cells occurred predominantly singe cells, but a few in clusters. Nuclear molding was prominent. No glandular formation or nesting was noted. The second tumor cells had high nuclear/cytoplasmic ratio, irregular nuclear membrane, and coarse granular chromatin. The background was inflamed and necrotic. The histologic findings of transurethral resection were mainly composed of small cell carcinoma, and partly transitional cell and signet ring cell carcinomatous components. Small cell neuroendocrine carcinoma have distinctive cytologic features to make a proper diagnosis.
- Gastrointestinal Adenomatous Polyposis Associated with Small Cell Neuroendocrine Carcinoma of the Rectosigmoid: A case report.
- Wan Seop Kim, Eun Kyung Hong, Kang Sik Kim, Kwang Soo Lee, Jung Dal Lee
- Korean J Pathol. 1996;30(11):1040-1044.
- 2,114 View
- 16 Download
-
Abstract
PDF
- In adenomatous polyposis coli there are many colonic and extracolonic manifestations, and various combinations of these induce different clinical presentations and syndromes. We experienced a unique case of adenomatous polyposis of the large intestine and stomach in a 39-year-old man. In the colon, small cell neuroendocrine carcinoma rather than adenocarcinoma had developed, which did not contain adenomatous or carcinomatous foci. The adenomatous polyps in the colon were all small and sessile with no cancerous or precancerous change two years after the resection of the symptomatic gastric adenomas, even though the gastric adenomas were larger and showed dysplastic change. We think this case is another variant of adenomatous polyposis syndrome.
 First
First Prev
Prev


