 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(2); 2014 > Article
-
Brief Case Report
Adenocarcinoma Arising in Gastric Duplication Cyst - Hyo Jeong Kang, Se Jin Jang, Young Soo Park
-
Korean Journal of Pathology 2014;48(2):159-161.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.2.159
Published online: April 28, 2014
Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- Corresponding Author: Young Soo Park, M.D. Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea. Tel: +82-2-3010-5608, Fax: +82-2-472-7898, youngspark@amc.seoul.kr
• Received: April 16, 2013 • Revised: June 16, 2013 • Accepted: June 18, 2013
© 2014 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
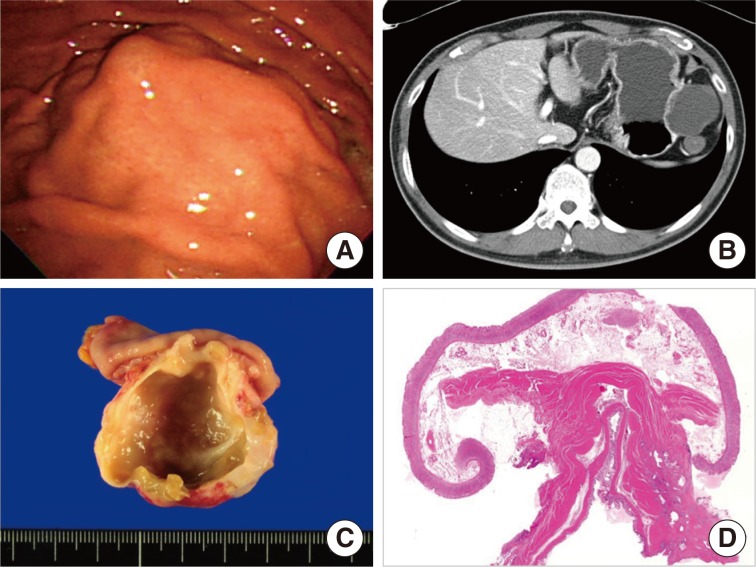
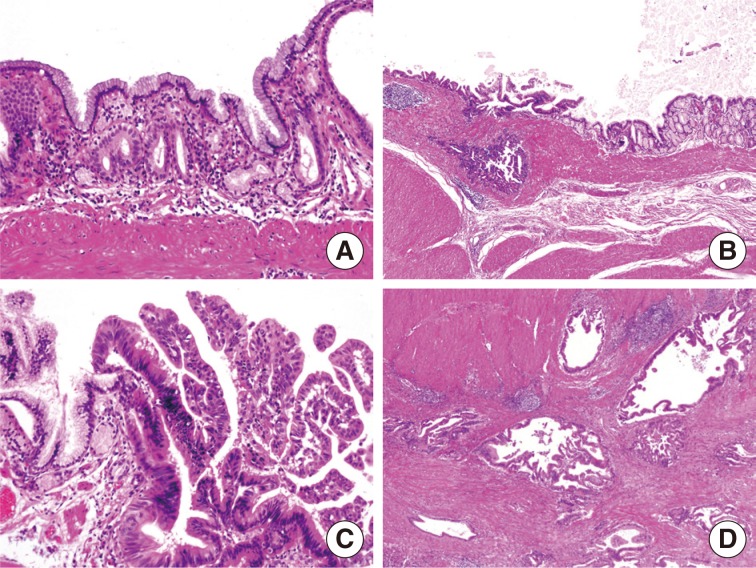
- A 56-year-old man was admitted to Asan Medical Center with a gastric submucosal lesion that was detected by esophagogastroduodenoscopy during a regular check-up (Fig. 1A). The overlying gastric mucosa was normal except for a slight elevation, and no associated symptoms were present. His medical and family histories were unremarkable. A complete blood count and serum chemistry tests were normal. A computerized tomography (CT) scan revealed a 5.5-cm low attenuating cystic mass located in the submucosal layer along the greater curvature of the body (Fig. 1B). The radiologic differential diagnoses were cystic degeneration of the neurogenic tumor, gastrointestinal stromal tumor (GIST), and gastric duplication cyst. The patient underwent a wedge resection to remove the lesion, and an unilocular cystic mass measuring 5.5×3.5×2.5 cm was identified in the proper muscle layer with smooth and intact overlying gastric mucosa. Thick, yellowish fluid filled the cyst and there were no connections between the cyst and the lumen of the stomach. The cystic wall had a regionally thickened portion (0.6 cm) and its cut surface was firm and granular (Fig. 1C). Microscopically, the cystic wall was comprised of all of the layers of the stomach wall (from the mucosa to the muscularis propria). The proper muscle layer of the cyst merged into the proper muscle layer of the stomach, sharing a common wall (Fig. 1D). The lining epithelial cells of the cyst were columnar and mucus-secreting cells resembling foveolar cells (Fig. 2A). There were multiple foci of high grade dysplasia (Fig. 2B, C) and adenocarcinoma showing invasion to the proper muscle layer of the cyst was observed (Fig. 2D). The histological features of the carcinoma resembled conventional adenocarcinomas commonly observed in the gastrointestinal tract. The carcinoma did not extend beyond the cyst wall, and neither the proper muscle nor the subserosal layer of the surrounding normal stomach harbored any tumor cells. The overlying gastric mucosa was normal and the resection margins were clear. Three regional lymph nodes were harvested during the wedge resection, which showed no metastasis.
CASE REPORT
- Gastric duplication is an extremely rare congenital anomaly in adults. It usually presents as a saccular or elongated cystic mass attached to the stomach. This is surrounded by at least one coat of smooth muscle, usually fusing the muscularis propria of the cyst and the stomach. The cyst is lined by typical gastric mucosa, often accompanied by patches of ectopic intestinal, colonic, respiratory epithelium, or pancreatic tissue. The presence of pancreatic tissue or gastric mucosa leads to complications such as peptic ulcers or acute pancreatitis. Most of the gastric duplications are located in the greater curvature, because gastric duplications usually originate dorsal to the primitive intestine.6
- Although gastric duplication is usually found as an asymptomatic mass, there can be symptoms associated with complications, such as pain, obstruction, ulceration, and hemorrhage. The malignant transformation of gastric duplications is very rare and only nine cases have been reported in the literature. Eight out of these nine cases presented with clinical symptoms such as abdominal pain, vomiting, and weight loss. However, our patient was asymptomatic and the lesion was detected during a regular check-up. The most common histologic type of malignancy arising in gastric duplications was adenocarcinoma (seven cases), but squamous cell carcinoma (one case) and neuroendocrine carcinoma (one case) were also reported.1,2,4,5 Six cases showed invasion to the adjacent stomach wall, but three cases were confined within the wall of the duplication cyst, as in the present case.
- Differential diagnoses based on radiologic or endoscopic findings are cystic neoplasms or tumors with cystic degeneration, such as a GIST, neuroendocrine tumor, neurogenic tumor, or heterotopic pancreas. An abdominal CT or magnetic resonance imaging can be a useful tool in differentiating duplication cysts from other cystic lesions. However, depending on the series, up to 70% of the cases can be misdiagnosed as solid lesions due to the variable amount of highly concentrated proteins in cystic contents.6 Therefore, histological confirmation through endoscopic ultrasonography-guided aspiration or biopsy is generally recommended to rule out the possibility of malignant changes in gastric duplication cysts.6,7
- The present case of adenocarcinoma arising in a gastric duplication cyst presented as a submucosal tumor during endoscopic examination. Adenocarcinoma arising in gastritis cystica profunda (GCP)8,9,10 is an important differential diagnosis, both histologically and endoscopically. GCP is a benign lesion characterized by herniated or displaced normal gastric glands in the submucosa, which sometimes show cystic dilatations. GCPs can also present as polypoid lesions and are thus sometimes called gastritis cystica polyposa. Although most GCPs are found in a previously operated stomach, they can also be found in an unoperated stomach. The major difference between a gastric duplication cyst and a GCP is that a GCP does not have a smooth muscle coat surrounding the lesion. Additionally, a gastric duplication cyst is usually located in the proper muscle layer, but GCP does not go deeper than the submucosa. Finally, a gastric duplication cyst is a congenital lesion, whereas a GCP is thought to be a reactive lesion due to chronic gastritis.
- The location of malignancy is also different in the cases of adenocarcinomas associated with GCPs versus the cases associated with gastric duplication cysts. In GCPs, the focus of the carcinoma is located in the superficial portion of the GCP and invades below the submucosal layer,10 but the focus of a carcinoma arising in a duplication cyst lies in the mucosal layer of the cyst wall and invades beyond the cyst wall and further into the gastric wall layers.1,2,4,5 Therefore, an adenocarcinoma associated with GCP can be diagnosed by endoscopic biopsies, but an adenocarcinoma arising in a duplication cyst cannot be confirmed without wedge resection.
- In summary, a gastric duplication cyst is a rare congenital anomaly with a potential for malignant transformation. It should be considered as a differential diagnosis of cystic lesions in the stomach, and wedge resection is the most effective way to confirm the diagnosis.
DISCUSSION
- 1. Kuraoka K, Nakayama H, Kagawa T, Ichikawa T, Yasui W. Adenocarcinoma arising from a gastric duplication cyst with invasion to the stomach: a case report with literature review. J Clin Pathol 2004; 57: 428-431. ArticlePubMedPMC
- 2. Horne G, Ming-Lum C, Kirkpatrick AW, Parker RL. High-grade neuroendocrine carcinoma arising in a gastric duplication cyst: a case report with literature review. Int J Surg Pathol 2007; 15: 187-191. ArticlePubMedPDF
- 3. Bonacci JL, Schlatter MG. Gastric duplication cyst: a unique presentation. J Pediatr Surg 2008; 43: 1203-1205. ArticlePubMed
- 4. Barussaud ML, Meurette G, Cassagnau E, Dupasc B, Le Borgne J. Mixed adenocarcinoma and squamous cell carcinoma arising in a gastric duplication cyst. Gastroenterol Clin Biol 2008; 32: 188-191. ArticlePubMed
- 5. Zheng J, Jing H. Adenocarcinoma arising from a gastric duplication cyst. Surg Oncol 2012; 21: e97-e101. ArticlePubMed
- 6. Seijo Rios S, Larino Noia J, Abdulkader Nallib I, et al. Adult gastric duplication cyst: diagnosis by endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA). Rev Esp Enferm Dig 2008; 100: 586-590. PubMed
- 7. Kojima T, Takahashi H, Parra-Blanco A, Kohsen K, Fujita R. Diagnosis of submucosal tumor of the upper GI tract by endoscopic resection. Gastrointest Endosc 1999; 50: 516-522. ArticlePubMed
- 8. Park CH, Park JM, Jung CK, et al. Early gastric cancer associated with gastritis cystica polyposa in the unoperated stomach treated by endoscopic submucosal dissection. Gastrointest Endosc 2009; 69: e47-e50. ArticlePubMed
- 9. Tuncer K, Alkanat M, Musoglu A, Aydin A. Gastritis cystica polyposa found in an unoperated stomach: an unusual case treated by endoscopic polypectomy. Endoscopy 2003; 35: 882.ArticlePubMed
- 10. Aoyagi K, Koufuji K, Yano S, et al. Two cases of cancer in the remnant stomach derived from gastritis cystica polyposa. Kurume Med J 2000; 47: 243-248. ArticlePubMed
REFERENCES
Fig. 1(A) Esophagogastroduodenoscopy reveals gastric submucosal lesion with normal overlying mucosa. (B) Abdominal computed tomography shows a 5.5-cm cystic lesion, located along the greater curvature side of the stomach, during the arterial phase. (C) An unilocular cyst is readily seen below the mucosa when the lesion is bisected. The inner surface of the cyst is smooth but the cut surface of the cyst wall shows focal irregularity. (D) The cyst wall shares a common wall with the gastric proper muscle layer.
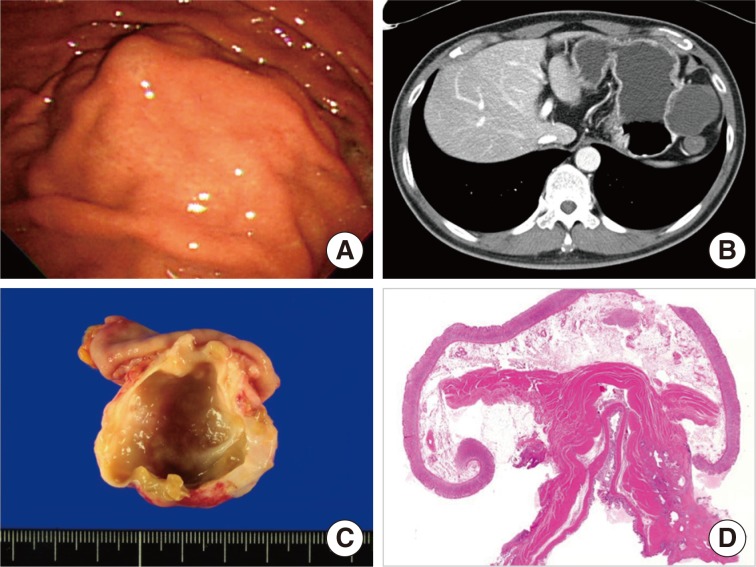
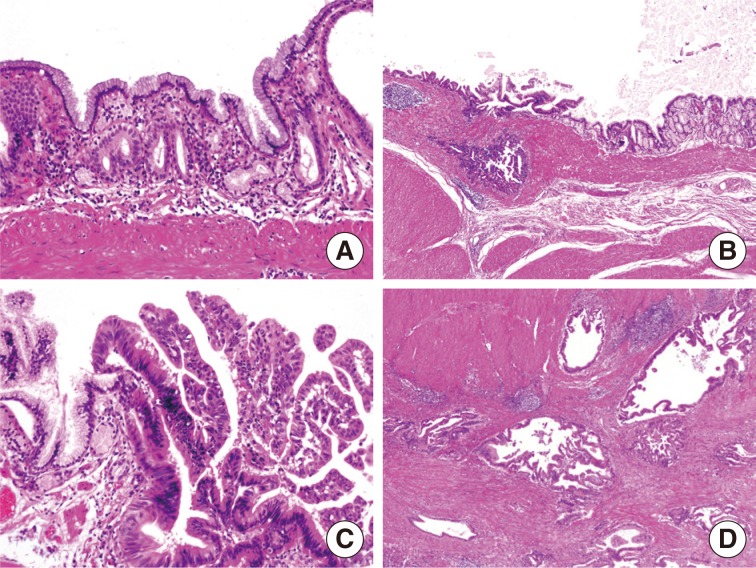
Figure & Data
References
Citations
Citations to this article as recorded by 
- Low-Grade Mucinous Neoplasm Arising in an Enteric Duplication Cyst of Pancreas: A Case Report and Literature Review
Mengjing Fan, Fang Yang
International Journal of Surgical Pathology.2024; 32(2): 422. CrossRef - Mixed Pancreatobiliary Ductal Adenocarcinoma and Squamous Cell Carcinoma Arising from an Ectopic Pancreas in a Gastric Duplication Cyst—A Rare Double Diagnosis
Minhye Kim, Jungwook Yang, Daehyun Song, Hyojung An, Dongchul Kim
Diagnostics.2024; 14(23): 2727. CrossRef - Resección laparoscópica de quiste de duplicación gástrica asistida por endoscopia
Camilo Naranjo-Salazar, Juan Esteban Botero-Velásquez, Mauricio Moreno
Revista Colombiana de Cirugía.2023; 39(3): 470. CrossRef - Clinical features of gastric duplications: evidence from primary case reports and published data
Yang Li, Chen Li, Hao Wu, Quan Wang, Zhi-Dong Gao, Xiao-Dong Yang, Ke-Wei Jiang, Ying-Jiang Ye
Orphanet Journal of Rare Diseases.2021;[Epub] CrossRef - Sarcomatoid Carcinoma Arising in a Gastric Duplication Cyst
Mohamed A. H. Ahmed, Kanchana Sanjeewani Liyanaarachchi, Shaun R. Preston, Madeleine Hewish, Izhar N. Bagwan
ACG Case Reports Journal.2021; 8(5): e00584. CrossRef - Pancreatobiliary Adenocarcinoma in a Gastric Duplication Cyst: A Doubly Rare Diagnosis
Ana Rolo, Rui Caetano Oliveira, Bárbara Lima, Ana Barbosa, Ilda Faustino
Cureus.2021;[Epub] CrossRef - Adenocarcinoma Arising From a Gastric Duplication Cyst With Lymph Node Metastasis
Shoichi Kinugasa, Hiroyuki Monma, Yoshio Sakamoto, Takafumi Watanabe, Masayo Fujimoto
Cureus.2020;[Epub] CrossRef - Adult Gastric Bronchogenic Cyst With Elevated Tumor Marker in Containing Fluid: A Case Report and Literature Review
Jixuan Duan, Sheng Yan, Qiyi Zhang, Jingjin Wu, Yu Du, K. G Owusu-Ansah, Shusen Zheng
International Surgery.2019; 104(1-2): 58. CrossRef - Papillary Adenocarcinoma in a Gastric Duplication Cyst
Sonali Sethi, Satyajit Godhi, Sunil Kumar Puri
Indian Journal of Surgical Oncology.2018; 9(1): 79. CrossRef - Non‐communicating gastric duplication cyst in a 10‐week‐old Labrador Retriever puppy
MW Jack, D Burgess, A Griffin
Australian Veterinary Journal.2016; 94(5): 166. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
Adenocarcinoma Arising in Gastric Duplication Cyst


Fig. 1 (A) Esophagogastroduodenoscopy reveals gastric submucosal lesion with normal overlying mucosa. (B) Abdominal computed tomography shows a 5.5-cm cystic lesion, located along the greater curvature side of the stomach, during the arterial phase. (C) An unilocular cyst is readily seen below the mucosa when the lesion is bisected. The inner surface of the cyst is smooth but the cut surface of the cyst wall shows focal irregularity. (D) The cyst wall shares a common wall with the gastric proper muscle layer.
Fig. 2 (A) The lining epithelium of the cyst is columnar and mucus-secreting cells resembling foveolar epithelium. (B, C) High grade dysplasia is observed in the papillary configuration. (D) Tumor glands are invading into proper muscle layer of the cyst wall.
Fig. 1
Fig. 2
Adenocarcinoma Arising in Gastric Duplication Cyst

