 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(1); 2013 > Article
-
Original Article
Fine Needle Aspiration Cytology of Thyroid Follicular Neoplasm: Cytohistologic Correlation and Accuracy - Changyoung Yoo, Hyun Joo Choi, Soyoung Im, Ji Han Jung, Kiouk Min1, Chang Suk Kang2, Young-Jin Suh3
-
Korean Journal of Pathology 2013;47(1):61-66.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.1.61
Published online: February 25, 2013
Department of Hospital Pathology, St. Vincent's Hospital, Suwon, Korea.
1Department of Hospital Pathology, St. Paul's Hospital, Seoul, Korea.
2Department of Hospital Pathology, Yeouido St. Mary's Hospital, Seoul, Korea.
3Department of Surgery, St. Vincent's Hospital, The Catholic University of Korea School of Medicine, Suwon, Korea.
- Corresponding Author: Hyun Joo Choi, M.D. Department of Hospital Pathology, St. Vincent's Hospital, The Catholic University of Korea School of Medicine, 93 Jungbu-daero, Paldal-gu, Suwon 442-723, Korea. Tel: +82-31-249-7592, Fax: +82-31-244-6786, chj0103@catholic.ac.kr
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- This study evaluated the accuracy of fine needle aspiration cytology (FNAC) in cases of follicular neoplasm (FN) on the basis of histologic diagnosis, and reviewed the cytologic findings of FN according to the FNAC.
-
Methods
- Among the 66 cases diagnosed with thyroid FN by FNAC during the 7-year period from 2003 to 2009, 36 cases that had undergone thyroid surgery were available for review. Cytologic diagnosis was compared with the histologic diagnosis of each case.
-
Results
- Among the 36 cases with a cytologic diagnosis of thyroid FN, histologic diagnosis was as follows: 20 follicular adenomas (55.6%), 3 Hurthle cell adenomas (8.3%), 2 follicular carcinomas (5.6%), 8 nodular goiters (22.2%), 2 papillary carcinomas (5.6%), and 1 Hashimoto's thyroiditis (2.8%), resulting in a diagnostic accuracy of FNAC for thyroid FN of 69.5%.
-
Conclusions
- This study shows that FNAC for thyroid FN is a useful primary screening method because when FN is diagnosed by FNAC, the rate of FN histologic diagnosis is relatively high, however, adequate sampling and experience is a prerequisite for this procedure.
- Among the 66 cases that had been diagnosed with thyroid FN by FNAC during the 7-year period from 2003 to 2009, 36 cases that underwent thyroid surgery were available for review. FNAC was performed under ultrasonographic guidance in all cases. We reviewed the cytology slides on the basis of representative cytologic FN findings such as abundance of follicular epithelial cells, presence of microfollicular structures, abundant cell crowding, abundant dispersed isolated cells, homogenous nuclear morphology, lack of nuclear grooves, lack of colloid material and lack of macrophages with reference to previous reports and the Bethesda system for reporting thyroid cytology.2,4,6,7 Regarding HCN, we looked only for the characteristic findings of Hurthle cells such as abundant finely granular cytoplasms enlarged, central or eccentrically located, round nucleus, prominent nucleolus, small cells with high nuclear/cytoplasmic ratio (small cell dysplasia), and large cells with at least 2× variability in nuclear size (large-cell dysplasia).7 However, for the cytologic review we applied the same cytologic standards as in FN. After slide review, cytologic diagnosis was compared with the histologic diagnosis of each case. We selected the cases which satisfied the standard adequacy criteria for interpreting thyroid cytology. The standard adequacy criteria is the presence of at least 6 groups of follicular cells in total on stained smears, with a minimum of 10 cells in each group.8 The slides used in this study were made by a conventional method and reviewed by 2 pathologists according to the guidelines provided in the Bethesda system.7 For confirmation of statistical significance the chi-square test was performed using SAS ver. 8 (SAS Inc., Cary, NC, USA). In all statistical analyses, a p<0.05 was considered significant. This study's protocol was approved by the Institutional Review Board of our hospital (no. VC11SISI0147).
MATERIALS AND METHODS
- A majority of the cases were female and only 2 cases were male. Ultrasonographic findings showed that 6 cases were benign, 5 cases were suspicious for malignancy, and 25 cases were indeterminate (Table 1). Among the 36 cases in which surgery was performed, 33 (91.7%) were diagnosed as FN and 3 (8.3%) were diagnosed as HCN in the preoperative FNAC. Of the 33 cases, 20 (55.6%) were diagnosed as FA, 3 (8.3%) were Hurthle cell adenoma (HCA), 2 (5.6%) were FC. A total of 25 cases (69.5%) were consistent with FN and the other cases included 8 (22.2%) nodular goiters, 2 (5.6%) PCs, and 1 (2.8%) Hashimoto's thyroiditis. All 3 cases which were cytologically diagnosed as HCN were proven histologically to be non-FN. Thus, the FNAC diagnostic accuracy for FN was 69.5% (Table 2). Regarding the clinicopathologic characteristics of the 25 cases which were diagnosed as FN, 23 were female and 2 were male. The age varied from 17 to 62 years and the average age was 38.4 years. The tumor sizes evaluated from the lobectomy or total thyroidectomy specimens ranged from 0.4 cm to 4.5 cm with an average size of 2.29 cm. The lesion sites included the right lobe (13 cases), left lobe (11 cases), and isthmus (1 case). Histologic subtypes were as follows: microfollicular (19 cases), normofollicular (1 case), oncocytic (3 cases), microfollicular with trabecular (1 case), and microfollicular with papillary hyperplasia (1 case) (Table 1).
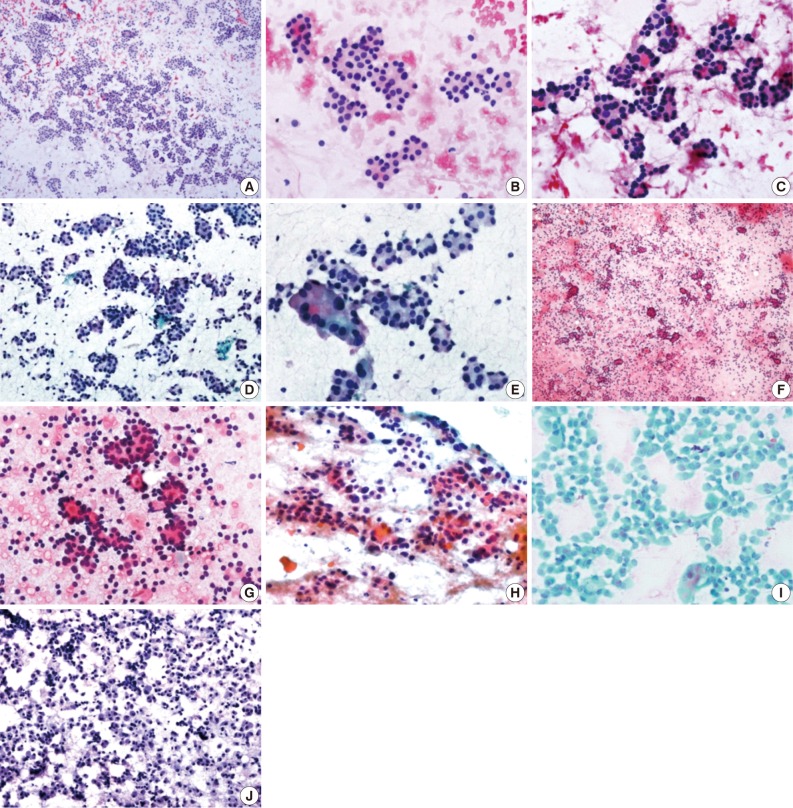
- These cases had generally sufficient cellularity for a proper diagnosis, and the majority showed the characteristic cytologic findings including abundance of follicular epithelial cells, presence of microfollicular structures, abundant cell crowding, abundant dispersed isolated cells, homogenous nuclear morphology, lack of nuclear grooves, lack of colloid material and lack of macrophages (Fig. 1). Among these cytologic features, high cellularity, abundant microfollicles, abundant cell crowding, and homogenous nuclear morphology were especially important features for the FN cytologic diagnosis (Table 3).
RESULTS
- The purpose of cytologic or pathological examination reports is to provide clinicians appropriate guidelines for the treatment of patients, including surgery to the clinicians.9 In the field of cytology, several report formats have been developed for this purpose, and presently, most reports are provided using categorical terms.10 Several forms of categorical diagnosis have been introduced. Generally, they include categories of unsatisfactory, benign, suspicious for malignancy, malignancy, and some forms have additional categories such as indeterminate, atypical, or follicular neoplasia.10 FA is defined as solitary encapsulated nodules arising in an otherwise normal thyroid that lack evidence of capsular or vascular invasion.5 HCN is considered a biologically different disease entity from FN, but is reported in the same category as FN with the additional mention of the possibility of HCN.7 Traditionally, FN and HCN were ambiguously classified in cytology because of the limitations of their cytologic diagnosis. Recently, the Bethesda system for reporting thyroid cytopathology was introduced which classified FN/HCN in the independent category. The traditional category of atypia includes the cytologic findings of suspicious FN/HCN in the terminology of follicular lesion of undetermined significance.7 However, the cytologic diagnosis of FN/HCN remains clinically controversial when compared to PC, which provides effective guidelines for the clinician.11,12 Using FNAC, the diagnostic accuracy of PC is more than 90%, but the distinction between malignancy and benign in FN or HCN is impossible because surgery is mandatory for the definitive diagnosis of FC or Hurthle cell carcinoma.2,13 Several diagnostic schemes including the Bethesda system described the malignancy rate, but in the case of FN, the malignancy rate is very low when compared to suspicious PC.7
- The Korean Thyroid Association introduced the revised edition of the updated guidelines for the diagnosis and management of thyroid nodules in 2010.1,3 In the revised guidelines, the FNAC results were described according to the Bethesda system. In this guideline, FNAC is recommended for nodules of more the 1.0 cm in size, nodules less than 1.0 cm in size but associated with risk factors, cystic nodules more than 2.0 cm in size, or patients with Hashimoto's thyroiditis because it is more commonly associated with PC.3,14 The revised edition also used the Bethesda system for the provision of treatment guidelines. For unsatisfactory cases, a repeat examination with follow-up or consideration of surgery is recommended. For benign cases, additional examination or treatments are not necessary. In the atypia category, because the malignancy rate is approximately 5-15%, a repeat FNAC with consideration of surgery is necessary. The category of suspicious malignancy or malignancy is indication for lobectomy or total thyroidectomy. For the FN, when the autonomic nodules are not found in the thyroid scan, lobectomy or total thyroidectomy is recommended. For the HCN, lobectomy or total thyroidectomy is recommended without a thyroid scan.1 In the FN or HCN cases, although a few cytologic findings can be helpful for the suspicion of FN/HCN, the prediction value of malignancy is relatively low.3,15 FNAC cannot provide definitive criteria for the distinction between benign and malignancy when FN/HCN is suspected.
- Diagnosis of FN/HCN by FNAC is the subject of several studies from Korea and other countries. In these studies, the cytologic diagnosis rate of FN was approximately 10% and a majority of FA or FC cases confirmed by histologic diagnosis showed a previous cytological diagnosis as benign, nodular hyperplasia, and even as PC.10,12,16-20 Most pathologists do not have sufficient experience with FN/HCN. In FNAC, the most important causes of diagnostic misinterpretation were overlapping cytological features among follicular-derived lesions and inadequate/suboptimal specimens. Especially, the follicular variants of PC, FN, and adenomatous hyperplasia show overlapping cytological features making the diagnosis of FN/HCN more difficult.16,21
- Although difficult, the ultimate purpose of FNAC in FN/HCN cases is to isolate FC. The present study showed the diagnostic specificity of FA including HCA was 64%, with a malignancy rate of 11% when a histologic correlation was conducted. Among the malignancies, 2 FCs and 2 PCs were identified. The malignancy rate in the present study did not reach the same level as with the Bethesda system, but PCs were not exclusively included. Therefore, PC was successfully screened by FNAC with the relevant cytological diagnosis, and the diagnostic specificity of FN by FNAC was relatively high when compared with the histologic diagnosis. Specifically, among the FNs, 2 FCs were successfully identified even though the number of cases was small. These results are well correlated with the clinical experience that lobectomy or total thyroidectomy is recommended for the cytologically suspected FN. The FN category is controversial because follicular lesions include various diseases and their differential diagnosis by FNAC is not readily made, and in particular, considerable areas of cytologically suspected FNs were identified as PCs by histologic examination.22 Because this category predicts the existence of FC to some extent and leads to surgical treatment, this category has sufficient value in FNAC.
- The present study started with the selection of cytologically diagnosed FN, and cases were chosen where correlation with histologic diagnosis was available. Therefore, this was a slightly different approach when compared with preexisting methods which started with the histologically confirmed FA or FC cases and followed by analysis of their previous cytological diagnoses. However, this approach generally results in a low diagnostic FNAC rate in the case of FNs. These results can be easily verified in the above-mentioned reports. The present study shows that FNAC may be a useful method in primary FN/HCN screening of the thyroid gland, because if the FN is diagnosed by FNAC, the rate of histologic FN diagnosis is relatively high. However, adequate sampling and experience is a prerequisite for this procedure. The present study results hopefully can contribute to available data regarding FNs and be used in the future revisions and supplements of treatment guidelines for FNs.
DISCUSSION
- 1. Yi KH. Updated guidelines for the diagnosis and management of thyroid nodules. J Korean Med Assoc 2011; 54: 629-636. Article
- 2. Yim JH, Kim EY, Kim WG, et al. Postoperative findings of the cytological diagnosis of follicular neoplasm or Hurthle cell neoplasm and the risk of malignancy. Endocrinol Metab 2010; 25: 316-320. Article
- 3. Yi KH, Park YJ, Koong SS, et al. Revised Korean Thyroid Association management guidelines for patients with thyroid nodules and thyroid cancer. J Korean Soc Radiol 2011; 64: 389-416. Article
- 4. Koo J, Jung WH, Yang S, Hong S. Correlation and accuracy between fine needle aspiration cytology of thyroid lesions and histopathologic diagnosis: analysis of 322 histopathologically confirmed cases. Korean J Cytopathol 2008; 19: 144-151. Article
- 5. LiVolsi VA, Baloch ZW. Follicular-patterned tumors of the thyroid: the battle of benign vs. malignant vs. so-called uncertain. Endocr Pathol 2011; 22: 184-189. ArticlePubMedPDF
- 6. Park HD, Park WS, Kim SH, et al. Cytologic features of follicular adenoma and follicular carcinoma of the thyroid: a study on the likelihood of cytologic diagnosis by fine needle aspiration cytology. Korean J Cytopathol 2008; 19: 152-159. Article
- 7. Ali SZ, Cibas ES. The Bethesda system for reporting thyroid cytopathology. 2010; New York: Springer.
- 8. Jing X, Wey E, Michael CW. Retrospective evaluation of instituted standard adequacy criteria for on-site adequacy assessment of thyroid fine-needle aspiration. Diagn Cytopathol 2011; 39: 391-394. ArticlePubMed
- 9. Singh RS, Wang HH. Eliminating the "atypia of undetermined significance/follicular lesion of undetermined significance" category from the Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol 2011; 136: 896-902. ArticlePubMed
- 10. Min SK, Seo J, Jun SY, Min K, Park HR. The analysis of indeterminate category in thyroid fine needle aspiration. Korean J Pathol 2010; 44: 657-661. Article
- 11. Chung YS, Yoo C, Jung JH, Choi HJ, Suh YJ. Review of atypical cytology of thyroid nodule according to the Bethesda system and its beneficial effect in the surgical treatment of papillary carcinoma. J Korean Surg Soc 2011; 81: 75-84. ArticlePubMedPMC
- 12. Lee K, Jung CK, Lee KY, Bae JS, Lim DJ, Jung SL. Application of bethesda system for reporting thyroid aspiration cytology. Korean J Pathol 2010; 44: 521-527. Article
- 13. Deandrea M, Ragazzoni F, Motta M, et al. Diagnostic value of a cytomorphological subclassification of follicular patterned thyroid lesions: a study of 927 consecutive cases with histological correlation. Thyroid 2010; 20: 1077-1083. ArticlePubMed
- 14. Fiore E, Rago T, Latrofa F, et al. Hashimoto's thyroiditis is associated with papillary thyroid carcinoma: role of TSH and of treatment with L-thyroxine. Endocr Relat Cancer 2011; 18: 429-437. ArticlePubMed
- 15. Broome JT, Solorzano CC. The impact of atypia/follicular lesion of undetermined significance on the rate of malignancy in thyroid fine-needle aspiration: evaluation of the Bethesda System for Reporting Thyroid Cytopathology. Surgery 2011; 150: 1234-1241. ArticlePubMed
- 16. Yang J, Schnadig V, Logrono R, Wasserman PG. Fine-needle aspiration of thyroid nodules: a study of 4703 patients with histologic and clinical correlations. Cancer 2007; 111: 306-315. ArticlePubMed
- 17. Deveci MS, Deveci G, LiVolsi VA, Baloch ZW. Fine-needle aspiration of follicular lesions of the thyroid: diagnosis and follow-up. Cytojournal 2006; 3: 9.PubMedPMC
- 18. Wu S, DeMay RM, Papas P, Yan B, Reeves W. Follicular lesions of the thyroid: a retrospective study of 1,348 fine needle aspiration biopsies. Diagn Cytopathol 2012; 40(Suppl 1): E8-E12. ArticlePubMed
- 19. Lee MJ, Hong SW, Chung WY, Kwak JY, Kim MJ, Kim EK. Cytological results of ultrasound-guided fine-needle aspiration cytology for thyroid nodules: emphasis on correlation with sonographic findings. Yonsei Med J 2011; 52: 838-844. ArticlePubMedPMC
- 20. Teixeira GV, Chikota H, Teixeira T, Manfro G, Pai SI, Tufano RP. Incidence of malignancy in thyroid nodules determined to be follicular lesions of undetermined significance on fine-needle aspiration. World J Surg 2012; 36: 69-74. ArticlePubMedPDF
- 21. Baloch ZW, Sack MJ, Yu GH, LiVolsi VA, Gupta PK. Fine-needle aspiration of thyroid: an institutional experience. Thyroid 1998; 8: 565-569. ArticlePubMed
- 22. Kapur U, Wojcik EM. Follicular neoplasm of the thyroid: vanishing cytologic diagnosis? Diagn Cytopathol 2007; 35: 525-528. ArticlePubMed
REFERENCES
USG, ultrasonogram; F, female; L, left; BN, benign; FA, follicular adenoma; R, right; M, male; SM, suspicious for malignancy; ID, indeterminate; NH, nodular hyperplasia; B, bilateral; HT, Hashimoto's thyroiditis; I, isthmus; FC, follicular carcinoma; HA, Hurthle cell adenoma; PC, papillary carcinoma.
| Cytologic features |
HD corresponds to FN (%) |
HD corresponds to NFN (%) |
p-valuea | ||||||
|---|---|---|---|---|---|---|---|---|---|
| FA (n = 20) | HA (n = 3) | FC (n = 2) | Total (n = 25) | NH (n = 8) | PC (n = 2) | HT (n = 1) | Total (n = 11) | ||
| High cellularity | 20 (100) | 3 (100) | 2 (100) | 25 (100) | 7 (87.5) | 1 (50) | 1 (100) | 9 (81.8) | 0.028* |
| Abundant microfollicles | 20 (100) | 3 (100) | 2 (100) | 25 (100) | 6 (75) | 1 (50) | 0 (0) | 7 (63.6) | 0.001* |
| Abundant cell crowding | 20 (100) | 3 (100) | 2 (100) | 25 (100) | 7 (87.5) | 1 (50) | 1 (100) | 9 (81.8) | 0.028* |
| Abundant dispersed isolated cells | 18 (90) | 3 (100) | 2 (100) | 23 (92) | 5 (62.5) | 2 (100) | 1 (100) | 8 (72.7) | 0.123 |
| Homogenous nuclear morphology | 20 (100) | 0 (0) | 2 (100) | 22 (88) | 5 (62.5) | 0 (0) | 0 (0) | 5 (45.5) | 0.007* |
| Lack of nuclear grooves | 20 (100) | 2 (66.7) | 2 (100) | 24 (96) | 8 (100) | 1 (50) | 0 (0) | 9 (81.8) | 0.156 |
| Lack of colloid material | 19 (95) | 3 (100) | 2 (100) | 24 (96) | 8 (100) | 2 (100) | 1 (100) | 11 (100) | 0.501 |
| Lack of macrophages | 19 (95) | 3 (100) | 2 (100) | 24 (96) | 8 (100) | 2 (100) | 1 (100) | 11 (100) | 0.501 |
FNAC, fine needle aspiration cytology; HD, histologic diagnosis; FN, follicular neoplasm; NFN, non-follicular neoplasm; FA, follicular adenoma; HA, Hurthle cell adenoma (FA, oncocytic variant); FC, follicular carcinoma; NH, nodular hyperplasia; PC, papillary carcinoma; HT, Hashimoto’s thyroiditis.
*p<0.05.
aChi-square test between FN and NFN.
Figure & Data
References
Citations
- Practical and challenging issue in thyroid cytopathology
Qianqian Zhang, Belen Padial Urtueta, Elisabetta Merenda, Gabriele Rotondaro, Noemi Morelli, Alessia Piermattei, Patrizia Straccia, Federica Cianfrini, Angela Feraco, Alessia Granitto, Antonino Mule, Esther Diana Rossi
Human Pathology.2026; 169: 106019. CrossRef - Evaluation and Management of Thyroid Nodules: A Joint Consensus Statement From the British Thyroid Association (BTA), British Association of Endocrine and Thyroid Surgeons (BAETS) and Collaborating Bodies
Ram Moorthy, Saba P. Balasubramanian, Kate Farnell, Mairead Kelly, Gitta Madani, Mufaddal Moonim, Carla Moran, Julia Priestley, Michael Stechman, Emma Watts, Kristien Boelaert
Clinical Endocrinology.2026; 104(6): 682. CrossRef - Indications for Core Needle Biopsy in Low-Suspicion Thyroid Nodules on US
Myoung Kyoung Kim, Jung Hee Shin, Haejung Kim, Soo Yeon Hahn
Journal of the Korean Society of Radiology.2026;[Epub] CrossRef - Diagnostic approach to FNA biopsy of cystic lesions of the head and neck
Stefen Andrianus, Olivia Leung, Zubair Baloch
Cancer Cytopathology.2025;[Epub] CrossRef - Malignancy risk in AUS thyroid lesions: comparison between FNA and CNB with implications for NIFTP diagnosis
Yeseul Kim, Jae Ho Shin, You-Na Sung, Dawon Park, Harim Oh, Hyo Seon Ryu, Kyeong Jin Kim, Hyun Joo Kim, Sin Gon Kim, Hoon Yub Kim, Kwang Yoon Jung, Seung-Kuk Baek, Sangjeong Ahn
Frontiers in Endocrinology.2025;[Epub] CrossRef - Correlation of Bethesda Categories in Thyroid Lesions With Histopathology: A Single Tertiary Care Center Experience
Sreenidhi Sreeram, Leena Dennis Joseph, Subalakshmi Balasubramanian
Cureus.2025;[Epub] CrossRef - Prevalence and Predictors of Malignancy in Contralateral Thyroid Lobe in Patients Undergoing Completion Thyroidectomy
Pradipta Kumar Parida, Siddhartha Pradhan, Chapity Preetam, Pradeep Pradhan, Dillip Kumar Samal, Saurav Sarkar
Indian Journal of Otolaryngology and Head & Neck Surgery.2022; 74(S2): 2053. CrossRef - Ultrasonographic and cytologic assessments of follicular neoplasms of the thyroid: Predictive features differentiating follicular carcinoma from follicular adenoma
Hye Shin Ahn, Hee Sung Kim, Min Ji Hong, Paula Soares
PLOS ONE.2022; 17(7): e0271437. CrossRef - 2019 Practice guidelines for thyroid core needle biopsy: a report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association
Chan Kwon Jung, Jung Hwan Baek, Dong Gyu Na, Young Lyun Oh, Ka Hee Yi, Ho-Cheol Kang
Journal of Pathology and Translational Medicine.2020; 54(1): 64. CrossRef - Preoperative diagnostic categories of fine needle aspiration cytology for histologically proven thyroid follicular adenoma and carcinoma, and Hurthle cell adenoma and carcinoma: Analysis of cause of under- or misdiagnoses
Hee Young Na, Jae Hoon Moon, June Young Choi, Hyeong Won Yu, Woo-Jin Jeong, Yeo Koon Kim, Ji-Young Choe, So Yeon Park, Paula Soares
PLOS ONE.2020; 15(11): e0241597. CrossRef - Core needle biopsy of thyroid nodules: outcomes and safety from a large single-center single-operator study
Jooae Choe, Jung Hwan Baek, Hye Sun Park, Young Jun Choi, Jeong Hyun Lee
Acta Radiologica.2018; 59(8): 924. CrossRef - Cytological Features That Differentiate Follicular Neoplasm from Mimicking Lesions
Kanghee Han, Hwa-Jeong Ha, Joon Seog Kong, Jung-Soon Kim, Jae Kyung Myung, Jae Soo Koh, Sunhoo Park, Myung-Soon Shin, Woo-Tack Song, Hye Sil Seol, Seung-Sook Lee
Journal of Pathology and Translational Medicine.2018; 52(2): 110. CrossRef - Comparison of the Diagnostic Efficacy of Ultrasound‐Guided Core Needle Biopsy With 18‐ Versus 20‐Gauge Needles for Thyroid Nodules
Hye Shin Ahn, Mirinae Seo, Su Min Ha, Hee Sung Kim
Journal of Ultrasound in Medicine.2018; 37(11): 2565. CrossRef - Subclassification of Bethesda Atypical and Follicular Neoplasm Categories According to Nuclear and Architectural Atypia Improves Discrimination of Thyroid Malignancy Risk
Joel Xue Yi Lim, Min En Nga, Dedrick Kok Hong Chan, Wee Boon Tan, Rajeev Parameswaran, Kee Yuan Ngiam
Thyroid.2018; 28(4): 511. CrossRef - The expression profile of integrin receptors and osteopontin in thyroid malignancies varies depending on the tumor progression rate and presence of BRAF V600E mutation
Galina Chernaya, Nina Mikhno, Tatiana Khabalova, Svetlana Svyatchenko, Lyudmila Mostovich, Sergey Shevchenko, Lyudmila Gulyaeva
Surgical Oncology.2018; 27(4): 702. CrossRef - The Usefulness of Immunocytochemistry of CD56 in Determining Malignancy from Indeterminate Thyroid Fine-Needle Aspiration Cytology
Hyunseo Cha, Ju Yeon Pyo, Soon Won Hong
Journal of Pathology and Translational Medicine.2018; 52(6): 404. CrossRef - Core Needle Biopsy of the Thyroid: 2016 Consensus Statement and Recommendations from Korean Society of Thyroid Radiology
Dong Gyu Na, Jung Hwan Baek, So Lyung Jung, Ji-hoon Kim, Jin Yong Sung, Kyu Sun Kim, Jeong Hyun Lee, Jung Hee Shin, Yoon Jung Choi, Eun Ju Ha, Hyun Kyung Lim, Soo Jin Kim, Soo Yeon Hahn, Kwang Hwi Lee, Young Jun Choi, Inyoung Youn, Young Joong Kim, Hye Sh
Korean Journal of Radiology.2017; 18(1): 217. CrossRef - Radiofrequency ablation of small follicular neoplasms: initial clinical outcomes
Su Min Ha, Jin Yong Sung, Jung Hwan Baek, Dong Gyu Na, Ji-hoon Kim, Hyunju Yoo, Ducky Lee, Dong Whan Choi
International Journal of Hyperthermia.2017; : 1. CrossRef - A meta‐analytic review of the Bethesda System for Reporting Thyroid Cytopathology: Has the rate of malignancy in indeterminate lesions been underestimated?
Patrizia Straccia, Esther Diana Rossi, Tommaso Bizzarro, Chiara Brunelli, Federica Cianfrini, Domenico Damiani, Guido Fadda
Cancer Cytopathology.2015; 123(12): 713. CrossRef - Impact of NRAS Mutations on the Diagnosis of Follicular Neoplasm of the Thyroid
Ja-Seong Bae, Seung Kyu Choi, Sora Jeon, Yourha Kim, Sohee Lee, Youn Soo Lee, Chan Kwon Jung
International Journal of Endocrinology.2014; 2014: 1. CrossRef - Diagnosis of Thyroid Follicular Neoplasm: Fine-Needle Aspiration Versus Core-Needle Biopsy
Ra Gyoung Yoon, Jung Hwan Baek, Jeong Hyun Lee, Young Jun Choi, Min Ji Hong, Dong Eun Song, Jae Kyun Kim, Jong Ho Yoon, Won Bae Kim
Thyroid.2014; 24(11): 1612. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
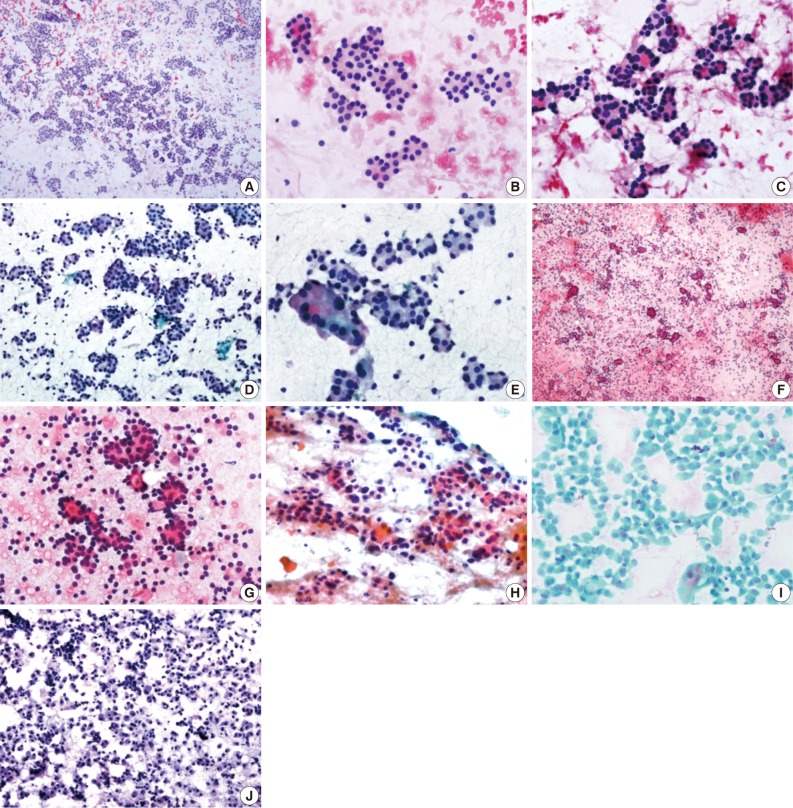

Fig. 1
| Cases | Sex/Age (yr) | Site | Size | USG | Histologic diagnosis |
|---|---|---|---|---|---|
| 1 | F/17 | L | 3.5 | BN | FA |
| 2 | F/17 | R | 1.7 | BN | FA |
| 3 | M/61 | R | 3.2 | SM | FA |
| 4 | F/51 | R | 1.7 | SM | FA |
| 5 | F/18 | L | 3.2 | BN | FA |
| 6 | F/44 | L | 4.5 | BN | FA |
| 7 | F/25 | L | 4.5 | ID | FA |
| 8 | F/28 | R | 1.9 | ID | FA |
| 9 | F/35 | R | 2.5 | BN | FA |
| 10 | F/25 | L | 1.5 | ID | FA |
| 11 | F/36 | R | 2.2 | BN | FA |
| 12 | F/37 | L | 1.6 | ID | NH |
| 13 | F/66 | L | 3.7 | ID | NH |
| 14 | F/39 | R | 2.5 | SM | FA |
| 15 | F/64 | R | 1.5 | ID | NH |
| 16 | F/64 | B | - | ID | HT |
| 17 | F/54 | R | 4 | ID | FA |
| 18 | F/36 | I | 2 | ID | FA |
| 19 | F/33 | L | 2.4 | ID | FC |
| 20 | F/62 | R | 1.3 | ID | FA |
| 21 | F/54 | R | 0.6 | SM | NH |
| 22 | F/30 | L | 1.7 | ID | FA |
| 23 | F/40 | L | 0.5 | ID | HA |
| 24 | F/44 | R | 0.4 | ID | FA |
| 25 | M/48 | L | 2.5 | ID | HA |
| 26 | F/40 | L | 1 | ID | FA |
| 27 | F/65 | L | 0.3 | ID | NH |
| 28 | F/70 | R | 0.8 | ID | NH |
| 29 | F/61 | R | 0.6 | ID | NH |
| 30 | F/39 | R | 1.5 | ID | FC |
| 31 | F/31 | R | 1.6 | ID | FA |
| 32 | F/51 | L | 2 | ID | FA |
| 33 | F/27 | B | 1.1 | ID | PC |
| 34 | F/48 | R | 5 | ID | NH |
| 35 | F/55 | R | 3.5 | ID | HA |
| 36 | F/62 | R | 1.5 | SM | PC |
| Cytologic diagnosis | No. of cases (%) | HD corresponds to FN (%) |
HD corresponds to NFN (%) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| FA | HA | FC | Total | NH | PC | HT | Total | ||
| FN | 33 (91.7) | 20 (55.6) | 3 (8.3) | 2 (5.6) | 25 (69.5) | 7 (19.4) | 1 (2.8) | - | 8 (22.2) |
| HCN | 3 (8.3) | - | - | - | - | 1 (2.8) | 1 (2.8) | 1 (2.8) | 3 (8.3) |
| Total | 36 (100) | 20 (55.6) | 3 (8.3) | 2 (5.6) | 25 (69.5) | 8 (22.2) | 2 (5.6) | 1 (2.8) | 11 (30.5) |
| Cytologic features | HD corresponds to FN (%) |
HD corresponds to NFN (%) |
p-value |
||||||
|---|---|---|---|---|---|---|---|---|---|
| FA (n = 20) | HA (n = 3) | FC (n = 2) | Total (n = 25) | NH (n = 8) | PC (n = 2) | HT (n = 1) | Total (n = 11) | ||
| High cellularity | 20 (100) | 3 (100) | 2 (100) | 25 (100) | 7 (87.5) | 1 (50) | 1 (100) | 9 (81.8) | 0.028 |
| Abundant microfollicles | 20 (100) | 3 (100) | 2 (100) | 25 (100) | 6 (75) | 1 (50) | 0 (0) | 7 (63.6) | 0.001 |
| Abundant cell crowding | 20 (100) | 3 (100) | 2 (100) | 25 (100) | 7 (87.5) | 1 (50) | 1 (100) | 9 (81.8) | 0.028 |
| Abundant dispersed isolated cells | 18 (90) | 3 (100) | 2 (100) | 23 (92) | 5 (62.5) | 2 (100) | 1 (100) | 8 (72.7) | 0.123 |
| Homogenous nuclear morphology | 20 (100) | 0 (0) | 2 (100) | 22 (88) | 5 (62.5) | 0 (0) | 0 (0) | 5 (45.5) | 0.007 |
| Lack of nuclear grooves | 20 (100) | 2 (66.7) | 2 (100) | 24 (96) | 8 (100) | 1 (50) | 0 (0) | 9 (81.8) | 0.156 |
| Lack of colloid material | 19 (95) | 3 (100) | 2 (100) | 24 (96) | 8 (100) | 2 (100) | 1 (100) | 11 (100) | 0.501 |
| Lack of macrophages | 19 (95) | 3 (100) | 2 (100) | 24 (96) | 8 (100) | 2 (100) | 1 (100) | 11 (100) | 0.501 |
USG, ultrasonogram; F, female; L, left; BN, benign; FA, follicular adenoma; R, right; M, male; SM, suspicious for malignancy; ID, indeterminate; NH, nodular hyperplasia; B, bilateral; HT, Hashimoto's thyroiditis; I, isthmus; FC, follicular carcinoma; HA, Hurthle cell adenoma; PC, papillary carcinoma.
HD, histologic diagnosis; FN, follicular neoplasm; HCN, Hurthle cell neoplasm; NFN, non-follicular neoplasm; FA, follicular adenoma; HA, Hurthle cell adenoma (FA, oncocytic variant); FC, follicular carcinoma; NH, nodular hyperplasia; PC, papillary carcinoma; HT, Hashimoto's thyroiditis.
FNAC, fine needle aspiration cytology; HD, histologic diagnosis; FN, follicular neoplasm; NFN, non-follicular neoplasm; FA, follicular adenoma; HA, Hurthle cell adenoma (FA, oncocytic variant); FC, follicular carcinoma; NH, nodular hyperplasia; PC, papillary carcinoma; HT, Hashimoto’s thyroiditis. p<0.05. Chi-square test between FN and NFN.

