 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 46(3); 2012 > Article
-
Case Report
Osteoclast-like Giant Cell Tumor of Parotid Gland with a Carcinomatous Component: A Case Report - Jung Wook Yang1, Hyeon Cheol Kim1, Jeong Hee Lee1,2, Jong Sil Lee1,2, Dong Chul Kim1,2, Dae Hyun Song1, Jin Pyeong Kim3, Gyung Hyuck Ko1,2
-
Korean Journal of Pathology 2012;46(3):297-301.
DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.3.297
Published online: June 22, 2012
1Department of Pathology, Gyeongsang National University School of Medicine, Jinju, Korea.
2Institute of Health Sciences, Gyeongsang National University, Jinju, Korea.
3Department of Otorhinolaryngology, Gyeongsang National University School of Medicine, Jinju, Korea.
- Corresponding Author: Gyung Hyuck Ko, M.D. Department of Pathology, Gyeongsang National University School of Medicine, 15 Jinju-daero 816beon-gil, Jinju 660-751, Korea. Tel: +82-55-772-8061, Fax: +82-55-759-7952, gyunghko@gnu.ac.kr
• Received: March 25, 2011 • Revised: June 17, 2011 • Accepted: June 20, 2011
© 2012 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- The giant cell tumor of the salivary gland is very rare, and 20 cases have been reported in the English-language literature. We report an additional case. A 57-year old man had noticed a mass in the right parotid area for several weeks. The diagnosis using aspiration cytology was a giant cell tumor possibly with a carcinomatous component. Superficial parotidectomy was carried out. The resected parotid gland contained a 1.8 cm-sized well-circumscribed brownish tumor. Histologically the tumor consisted of evenly distributed osteoclast-like giant cells, mononuclear cells and two small foci of a carcinomatous component. The osteoclast-like giant cells and mononuclear cells were positive for vimentin and CD68, and the carcinomatous component was positive for cytokeratin and epithelial membrane antigen. There was no metastatic lesion in the cervical lymph nodes. We believe this is the first case in Korea of an osteoclast-like giant cell tumor of the parotid gland.
- A 57-year-old man had noticed a mass in the right parotid area for several weeks. The mass was solid and firm with no pain or tenderness. Liquid-based aspiration cytology was performed (Fig. 1). The cytologic findings were numerous scattered osteoclast-like multinucleated giant cells and isolated mononuclear cells. The osteoclast-like giant cells and most of the mononuclear cells had benign-looking nuclei, but a few mononuclear cells had slightly atypical nuclei with clumped chromatin and prominent nucleoli. There was a small cluster of slightly atypical epithelial-like cells. We considered the diagnosis to be a giant cell tumor possibly with a carcinomatous component.
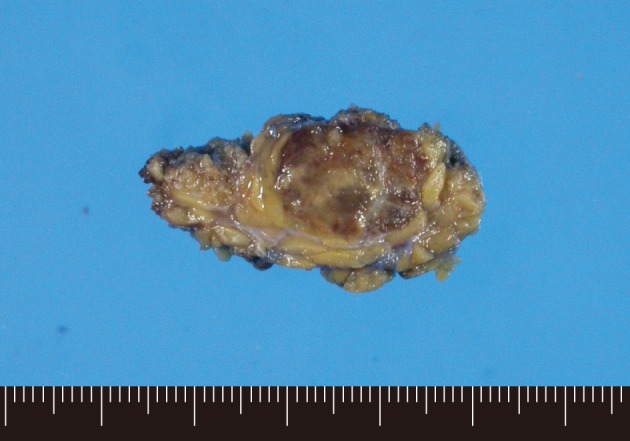
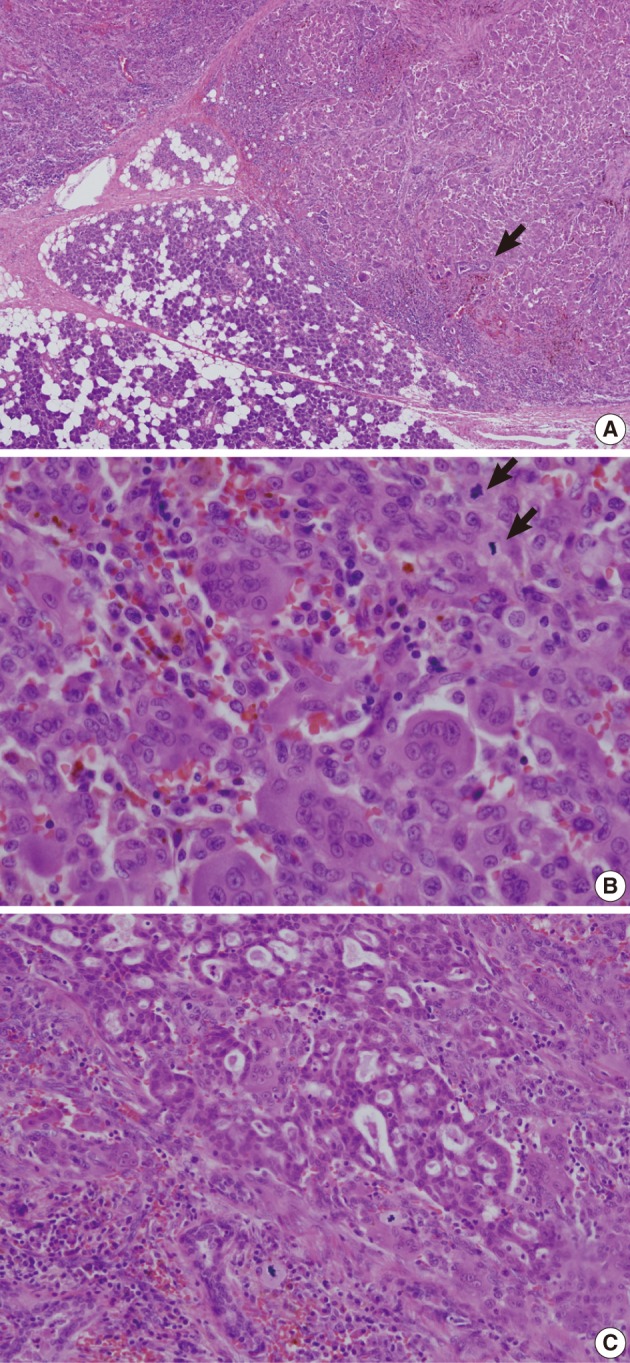
- The resected parotid gland contained a 1.8 cm-sized well-circumscribed round tumor (Fig. 2). The cut surface was mottled with light and dark brown colors. There was no necrosis or hemorrhage. Light microscopic examination revealed a well-circumscribed but not encapsulated tumor (Fig. 3). The tumor consisted of evenly distributed multinucleated giant cells, which were morphologically indistinguishable from osteoclasts, and round or short-spindled mononuclear cells. At first sight the tumor appeared to be a giant cell tumor of bone, but a careful examination revealed that many mononuclear cells had hyperchromatic nuclei with clumped chromatin. Many mitotic figures were found, up to 30 per 10 high-power fields. In addition, there were two small foci of carcinomatous component. The carcinomatous component was very small, such that it disappeared in the additional sections. The nuclei of the carcinoma cells did not appear to be very malignant but the cells were arranged in a cribriform pattern so that they were recognized as malignant. It appeared that there was no transitional area between the giant cell tumor and the carcinomatous component. There was no metastatic lesion in the cervical lymph nodes.
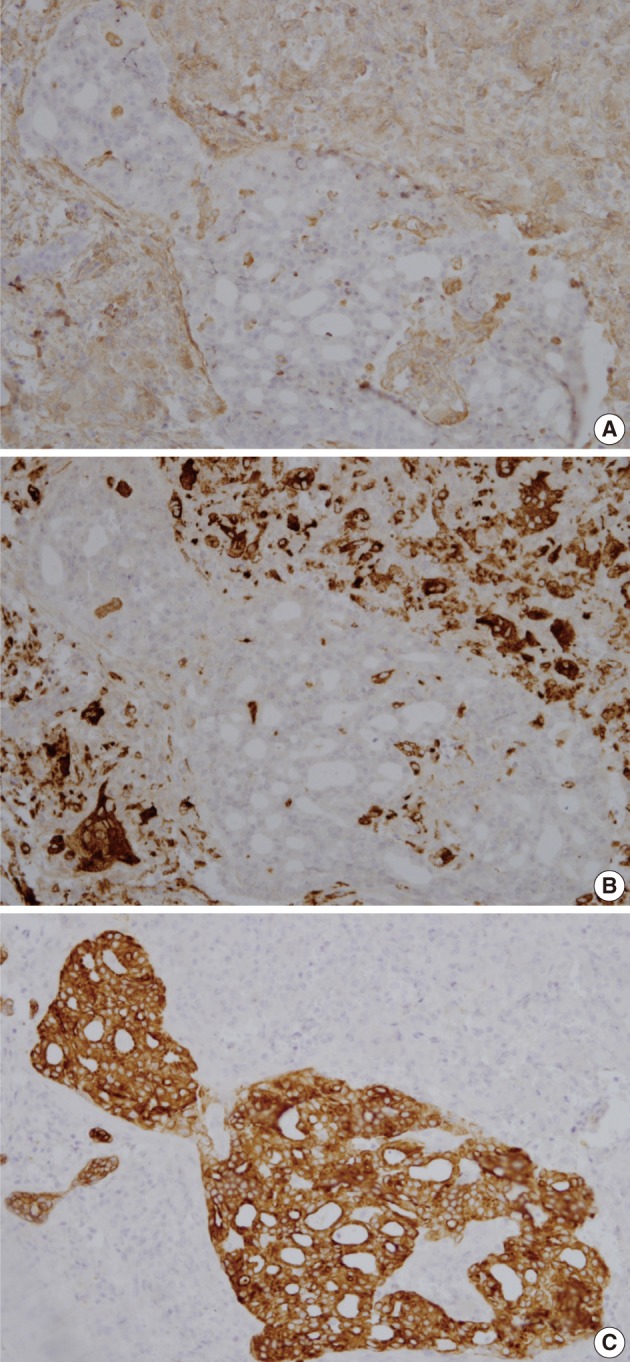
- Immunohistochemically, osteoclast-like giant cells were diffusely positive for vimentin and CD68, and negative for cytokeratin and epithelial membrane antigen (Fig. 4). Mononuclear cells were diffusely positive for vimentin, partly positive for CD68, and negative for cytokeratin and epithelial membrane antigen. The carcinoma cells were positive for cytokeratin and epithelial membrane antigen, and negative for vimentin and CD68.
CASE REPORT
- Giant cell tumors histologically mimicking giant cell tumors of bone may occur in the soft tissue and rarely in the visceral organs such as pancreas,15 thyroid,16 urinary bladder,17 and liver.18 These tumors are called osteoclast-type or osteoclast-like giant cell tumors because the giant cells seen in these tumors are morphologically similar to those seen in the giant cell tumor of bone. Of these, the giant cell tumor of soft tissue is similar to the giant cell tumor of bone both histologically and clinically. However, giant cell tumors of visceral organs usually contain a carcinomatous component and are clinically more aggressive than the giant cell tumor of bone.
- The GCT-SG is very rare and we found 20 cases in the English-language literature,1-14 with a total of 21 including our case. Seventeen cases occurred in the parotid gland, 3 cases in the submandibular gland4,8,9 and 1 case in the minor salivary gland.14 Most patients of GCT-SG were men and the male to female ratio was 17 : 4. The range of age was from 28 to 92, with the average age of 59. Twelve (57%) tumors contained a carcinomatous portion. In most cases, the carcinomatous portion was a salivary duct carcinoma, but in three cases, the carcinomatous portion was a carcinoma ex pleomorphic adenoma.1,7,9
- In two cases, the tumor contained a pleomorphic adenoma instead of a carcinoma.8,11 Metastasis to the cervical lymph node was present in one case,12 in which the metastatic tumor originated from the salivary duct carcinoma component. Eight patients were monitored for 9 months or longer. Of the 8 patients, six had no evidence of disease at 9 months up to 6 years after surgery. Two patients died with clinical evidence of disseminated disease including pulmonary metastasis.2,6 Our case showed no evidence of recurrence or metastasis at 3 months after surgery.
- GCT-SG morphologically differs from giant cell carcinoma or undifferentiated carcinoma with anaplastic giant cells. The giant cells of GCT-SG have bland-looking nuclei with homogenous chromatin distribution. In contrast, the giant cells in giant cell carcinoma or undifferentiated carcinoma with anaplastic giant cells are usually highly pleomorphic and hyperchromatic.
- GCT-SG also morphologically differs from giant cell tumor of bone. Unlike giant cell tumor of bone, the nuclei of mononuclear cells in GCT-SG are not similar to those of giant cells and show at least some nuclear irregularity and hyperchromasia, although usually not as severe as those in undifferentiated carcinoma. In our case, the mononuclear tumor cells were very bland-looking, such that at first sight the tumor appeared to be a giant cell tumor of bone. In other cases, the nuclei of neoplastic cells were described as bland, uniform, moderately atypical or uniform to bizarre. In only two cases, the nuclei of neoplastic cells were described as anaplastic2 or highly malignant.12
- Some authors believe that GCT-SG is a carcinoma and prefer the terminology of osteoclast-type giant cell carcinoma.10 We concur with this for the same reasons as they have suggested. First, GCT-SG usually contains a carcinomatous component, which cannot be explained by incidental coexistence. The carcinomatous component can be very small and focal, as it is in our case. It is possible that a small hidden focus of carcinomatous component may be found by a more diligent search in cases where the carcinomatous component was not reported to be present. Second, in contrast to giant cell tumor of bone, some of the mononuclear cells of GCT-SG expressed epithelial markers as well as histiocytic markers in several cases,2,3,10,12-14 although mononuclear cells in our case did not express epithelial markers. Third, the microsatellite pattern of the giant cell tumor component is more akin to the carcinomatous component and does not resemble giant cell tumor of bone.10
- The osteoclast-like giant cells are thought to be non-neoplastic. The giant cells are consistently negative for epithelial markers, as they are in our case, but express CD68, a histiocytic marker, and may be reactive cells representing a host response to neoplasm.
- In the World Health Organization (WHO) classification of tumors, the osteoclast-like giant cell tumor of the pancreas is described as a separate entity and is called undifferentiated carcinoma with osteoclast-like giant cells.19 In other organs, the osteoclast-like giant cell tumor is included in the undifferentiated carcinoma as an osteoclastic or a giant cell variant. According to the WHO classification of tumors, GCT-SG cannot be ascribed to any categories. We and some other authors10 do not support classifying this tumor under the category of undifferentiated carcinoma. We believe that GCT-SG has a stronger tendency of male predominance, less pleomorphic nuclei of tumor cells and more favorable prognosis than the undifferentiated carcinoma. The potential relationship of GCT-SG with salivary duct carcinoma and carcinoma ex pleomorphic adenoma, and whether the type and percent composition of the carcinomatous components determine the natural history need to be further evaluated.
- We found two cases of GCT-SG diagnosed by fine needle aspiration.11,12 The cytologic findings were numerous osteoclast-like multinucleated giant cells and isolated or clustered malignant-appearing mononuclear cells. Cohesive sheets of large polygonal epithelial cells were seen in one of the two cases. In our case, there were many osteoclast-like giant cells and mononuclear cells but only one small cluster of slightly atypical epithelial cells. When needle aspiration reveals many osteoclast-like giant cells but few atypical cells, as it did in our case, giant cell granuloma should be considered in differential diagnoses. Giant cell granuloma is smaller than GCT-SG in tumor size. The osteoclast-like giant cells in giant cell granuloma are fewer in number and have fewer and smaller nuclei.7
DISCUSSION
Acknowledgments
Acknowledgments
- 1. Eusebi V, Martin SA, Govoni E, Rosai J. Giant cell tumor of major salivary glands: report of three cases, one occurring in association with a malignant mixed tumor. Am J Clin Pathol 1984; 81: 666-675. ArticlePubMed
- 2. Balogh K, Wolbarsht RL, Federman M, O'Hara CJ. Carcinoma of the parotid gland with osteoclastlike giant cells: immunohistochemical and ultrastructural observations. Arch Pathol Lab Med 1985; 109: 756-761. PubMed
- 3. Batsakis JG, Ordonez NG, Sevidal PA Jr, Baker JR. Osteoclast-type giant cell neoplasms of the parotid gland. J Laryngol Otol 1988; 102: 901-904. ArticlePubMed
- 4. Ellis GL, Auclair PL, Genpp DR. Surgical pathology of the salivary glands. 1991; Vol. 25. Philadelphia: WB Saunder, 490-509.
- 5. Itoh Y, Taniguti Y, Arai K. A case of giant cell tumor of the parotid gland. Ann Plast Surg 1992; 28: 183-186. ArticlePubMed
- 6. Grenko RT, Tytor M, Boeryd B. Giant-cell tumour of the salivary gland with associated carcinosarcoma. Histopathology 1993; 23: 594-595. ArticlePubMed
- 7. Donath K, Seifert G, Röser K. The spectrum of giant cells in tumours of the salivary glands: an analysis of 11 cases. J Oral Pathol Med 1997; 26: 431-436. ArticlePubMed
- 8. Doğusoy G, Ozbay G, Girişken G, Dervişoğlu . Giant cell tumor of major salivary glands in association with pleomorphic adenoma. Arch Hell Med 1999; 16: 380-382.
- 9. Snyder ML, Paulino AF. Pathologic quiz case: an unusual salivary gland tumor. Arch Pathol Lab Med 2000; 124: 1559-1560. ArticlePubMedPDF
- 10. Tse LL, Finkelstein SD, Siegler RW, Barnes L. Osteoclast-type giant cell neoplasm of salivary gland. A microdissection-based comparative genotyping assay and literature review: extraskeletal "giant cell tumor of bone" or osteoclast-type giant cell "carcinoma"? Am J Surg Pathol 2004; 28: 953-961. PubMed
- 11. Torabinezad S, Kumar PV, Hashemi SB, Rahimi A. Osteoclastomalike giant cell tumor of the parotid gland: report of a case with fine needle aspiration diagnosis. Acta Cytol 2006; 50: 80-83. PubMed
- 12. Kadivar M, Nilipour Y, Sadeghipour A. Osteoclast-like giant-cell tumor of the parotid with salivary duct carcinoma: case report and cytologic, histologic, and immunohistochemical findings. Ear Nose Throat J 2007; 86: 628-630. ArticlePubMedPDF
- 13. Fang X, Hicks DG, Hicks W Jr, Zhang S. Osteoclastlike giant cell tumor of the salivary gland. Ann Diagn Pathol 2009; 13: 114-118. ArticlePubMed
- 14. Kusafuka K, Nakamura S, Asano R, et al. Osteoclast-type giant cell tumor of minor salivary gland with mucin-rich salivary duct carcinoma: a case report of unusual histology with immunohistochemical analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 109: 870-877. ArticlePubMed
- 15. Sung SH, Han WS. Fine needle aspiration cytology of osteoclastic giant cell tumor of the pancreas. Korean J Cytopathol 1998; 9: 89-94.
- 16. Cibull ML, Gray GF. Ultrastructure of osteoclastoma-like giant cell tumor of thyroid. Am J Surg Pathol 1978; 2: 401-405. ArticlePubMed
- 17. Behzatoğlu K, Durak H, Canberk S, et al. Giant cell tumor-like lesion of the urinary bladder. A report of two cases and literature review: giant cell tumor or undifferentiated carcinoma? Diagn Pathol 2009; 4: 48.ArticlePubMedPMC
- 18. Park CS, Kim JE, Chang MS. Fine needle aspiration cytology of osteoclast-like giant cell tumor of the liver: a case report. Korean J Cytopathol 1999; 10: 79-84.
- 19. Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 2010; 4th ed. Lyon: IARC Press, 294-295.
REFERENCES
Fig. 1(A) Aspiration cytology of a parotid gland mass reveals many osteoclast-like giant cells with benign-looking nuclei. (B) Most of the scattered mononuclear cells have benign-looking vesicular nuclei, but a few cells (arrow) have enlarged nuclei with chromatin clumping. (C) There is a cluster of epithelial-like cells with slightly atypical nuclei.
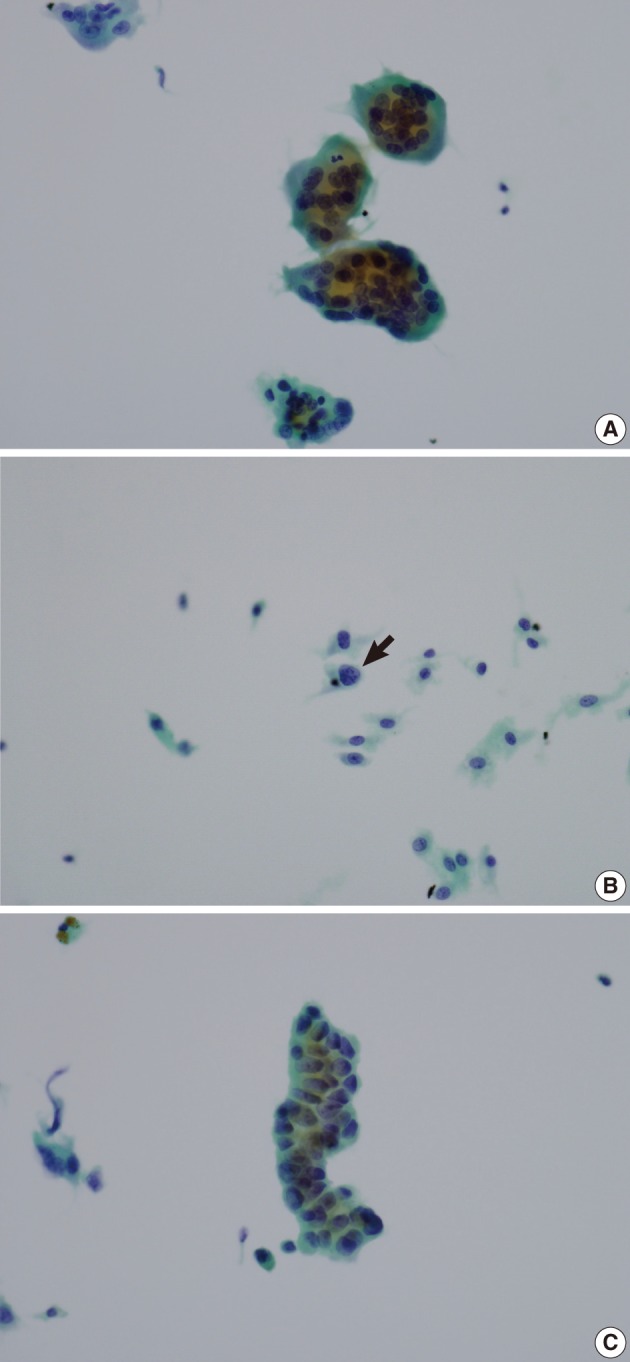
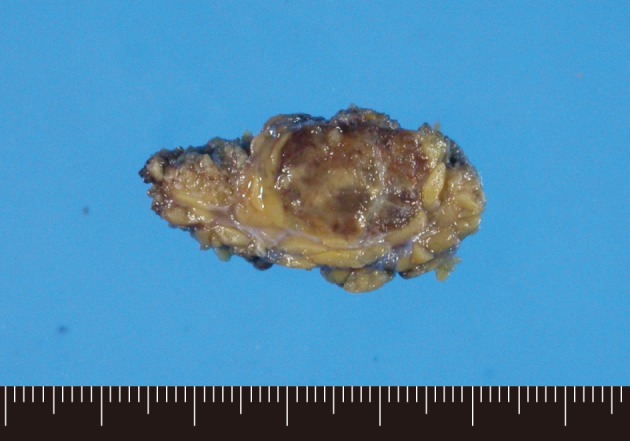
Fig. 3(A) A well-circumscribed but not encapsulated tumor is shown in the parotid gland. Several entrapped salivary ducts (arrow) are seen in the periphery of the tumor. (B) The tumor consists of osteoclast-like multinucleated giant cells and mononuclear cells. The mononuclear cells have round to oval vesicular nuclei with slightly coarse chromatin pattern. Mitotic figures (arrows) are found up to 30/10 high power field. (C) There is a small focus of carcinomatous component with cribriform arrangement of cancer cells.
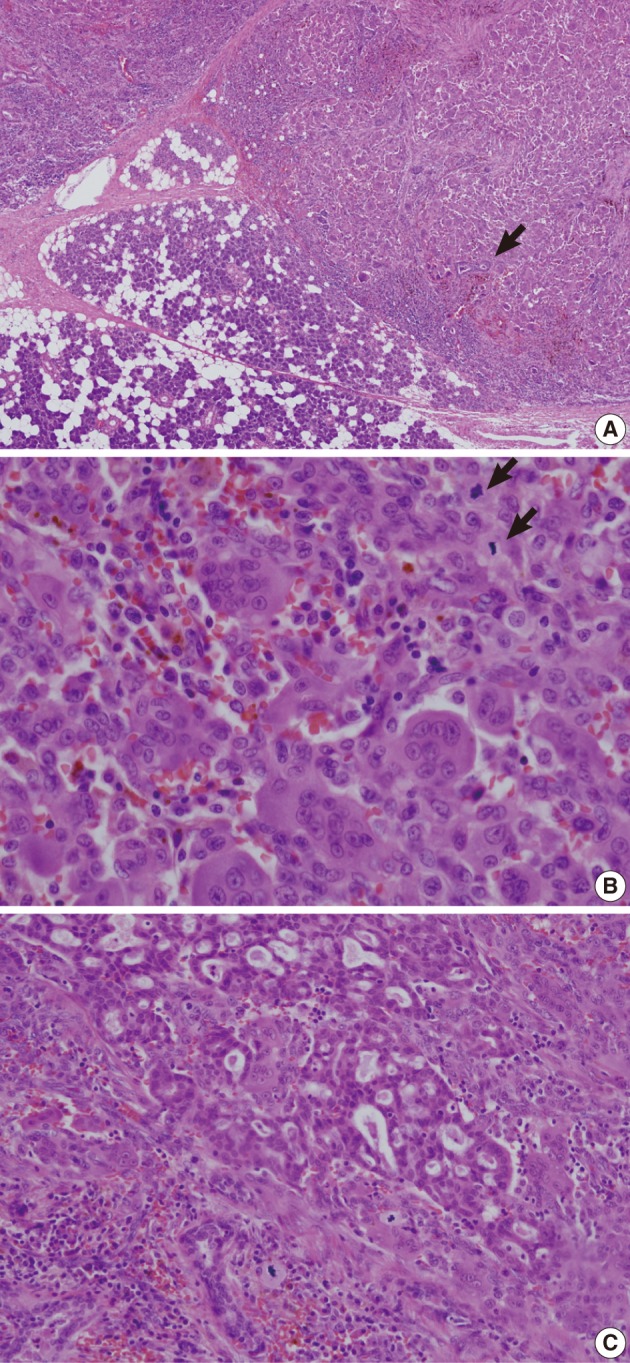
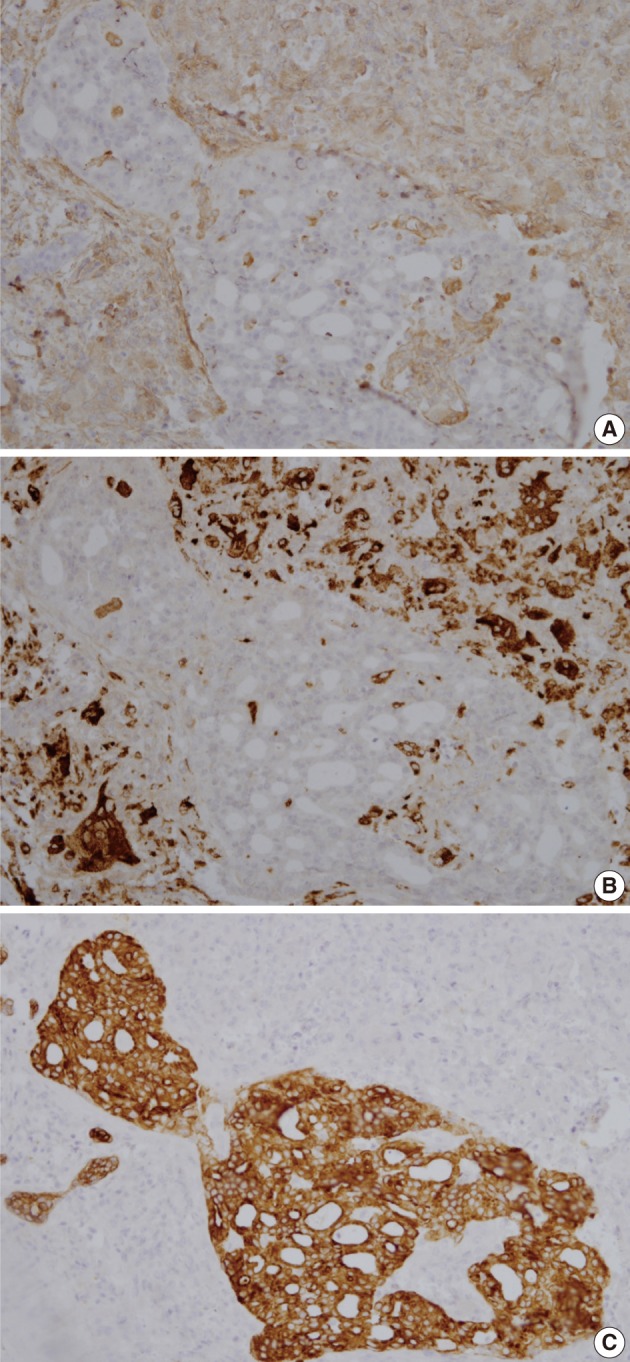
Figure & Data
References
Citations
Citations to this article as recorded by 
- Giant cell tumour of the parotid gland: a rare, unusual entity
Erna Ahsan, Kranthi Kumar Jandrasupalli, Prashant Durgapal, Divya Yadav
BMJ Case Reports.2025; 18(4): e261751. CrossRef - Genomic alteration in rare subtype of sarcomatoid salivary duct carcinoma
Ji-Seon Jeong, Kyung-Ja Cho, Deokhoon Kim, Yoon Se Lee, Joon Seon Song
Pathology - Research and Practice.2021; 228: 153678. CrossRef - Giant cell tumor of temporomandibular joint presenting as a parotid tumor: Challenges in the accurate subclassification of giant cell tumors in an unusual location
Rongqin Ren, Sandra Mueller, Adele O. Kraft, Celeste N. Powers
Diagnostic Cytopathology.2018; 46(4): 340. CrossRef - Osteoclast‐Like Giant Cell Tumor of the Parotid Gland: Report of a Case Diagnosed on Fine‐Needle Aspiration Cytology With Histological and Immunohistochemical Findings
Poonam Elhence, Meenakshi Rao, Amit Goyal, Amit Kumar, Pushpinder S. Khera, Shilajit Bhattacharya
Diagnostic Cytopathology.2016; 44(6): 548. CrossRef - Giant cell tumour of a temporomandibular joint presenting as a parotid mass: Case report and analysis of the 19 cases in the literature
Yun-Chen Huang, Jeng-Wen Chen, Yen-Lin Chen, Pei-Jen Lou
Journal of Cranio-Maxillofacial Surgery.2014; 42(8): 1778. CrossRef - Tumeur à cellules géantes de type ostéoclastique de la parotide
S. Rammeh, I. Hergli, M.K. M’farrej, N. Znaidi, S. Nechi, R. Zermani
Revue de Stomatologie, de Chirurgie Maxillo-faciale et de Chirurgie Orale.2014; 115(3): 185. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article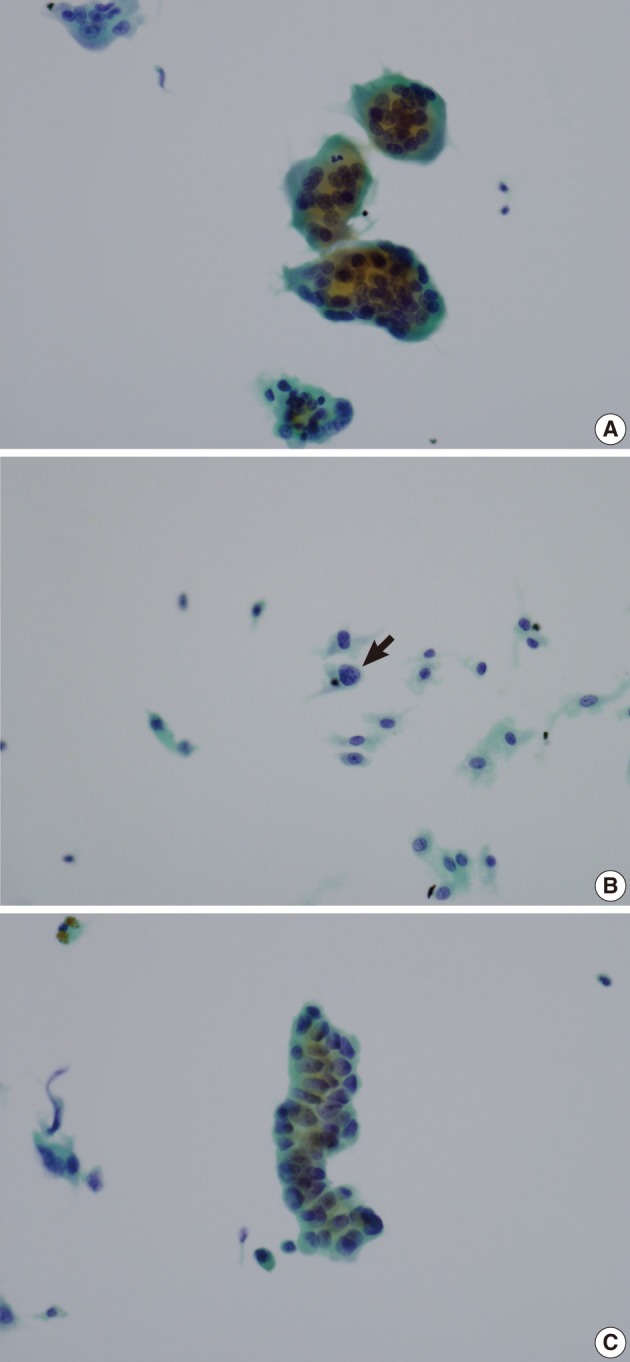
Osteoclast-like Giant Cell Tumor of Parotid Gland with a Carcinomatous Component: A Case Report




Fig. 1 (A) Aspiration cytology of a parotid gland mass reveals many osteoclast-like giant cells with benign-looking nuclei. (B) Most of the scattered mononuclear cells have benign-looking vesicular nuclei, but a few cells (arrow) have enlarged nuclei with chromatin clumping. (C) There is a cluster of epithelial-like cells with slightly atypical nuclei.
Fig. 2 A well-circumscribed brownish solid tumor is shown in the parotid gland.
Fig. 3 (A) A well-circumscribed but not encapsulated tumor is shown in the parotid gland. Several entrapped salivary ducts (arrow) are seen in the periphery of the tumor. (B) The tumor consists of osteoclast-like multinucleated giant cells and mononuclear cells. The mononuclear cells have round to oval vesicular nuclei with slightly coarse chromatin pattern. Mitotic figures (arrows) are found up to 30/10 high power field. (C) There is a small focus of carcinomatous component with cribriform arrangement of cancer cells.
Fig. 4 (A) Vimentin is expressed in osteoclast-like giant cells and mononuclear cells but not in carcinoma cells. (B) CD68 is expressed in osteoclast-like giant cells and some mononuclear cells but not in carcinoma cells. (C) Carcinoma cells are positive for cytokeratin.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Osteoclast-like Giant Cell Tumor of Parotid Gland with a Carcinomatous Component: A Case Report

