 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 46(3); 2012 > Article
-
Case Report
Tumor Budding and Recurrence in Submucosal Invasive Colorectal Cancers of Favorable Histology: Case Reports of Two Early Colorectal Cancers with Advanced Recurrences - Heae Surng Park, Hee Jin Chang1,2, Ji Won Park1, Byung Chang Kim1, Dae Kyung Sohn1, Chang Won Hong1, Ji-Yeon Baek1, Sun Young Kim1, Hyo Seong Choi1, Jae Hwan Oh1
-
Korean Journal of Pathology 2012;46(3):272-277.
DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.3.272
Published online: June 22, 2012
Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
1Center for Colorectal Cancer, National Cancer Center, Goyang, Korea.
2Department of Pathology, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
- Corresponding Author: Hee Jin Chang, M.D. Center for Colorectal Cancer and Department of Pathology, Research Institute and Hospital, National Cancer Center, 323 Ilsan-ro, Ilsandong-gu, Goyang 410-769, Korea. Tel: +82-31-920-1741, Fax: +82-31-920-1369, heejincmd@yahoo.com
• Received: November 1, 2010 • Revised: January 5, 2011 • Accepted: January 6, 2011
© 2012 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Complete resection of submucosal invasive colorectal cancer (SICC) showing favorable histology is regarded as curative. We report on two cases of SICC showing recurrence within 5 years despite complete resection. The first patient was a 68-year-old woman with well differentiated rectal adenocarcinoma invading the superficial submucosa, which recurred after 4.7 years. The second patient was a 53-year-old man with pT1N0 moderately differentiated colonic adenocarcinoma. He developed widespread tumor recurrence after 3.9 years. Retrospective pathologic review of the original tumors showed multiple foci of tumor budding at the invasive front. Immunohistochemical staining for D2-40 of deeper levels of the paraffin blocks showed rare foci of small lymphatic invasion. Tumor budding at the invasive front may be an important indicator for SICC aggressiveness or may reflect early lymphatic invasion. More aggressive pathologic examination and follow-up is required for patients with SICC showing tumor budding, even in the absence of unfavorable histologic findings.
- Case 1 was a 68-year-old female patient who was admitted for further treatment of an incidentally detected rectal polyp. Colonoscopic examination (Fig. 1A) showed a 2 cm-sized semipedunculated polyp, 7 cm from the anal verge. A biopsy showed an adenocarcinoma with a background of tubulovillous adenoma. Since preoperative computed tomography (CT) showed no evidence of lymph node or distant metastasis, she underwent transanal endoscopic microsurgery with full thickness of excision in August 2003. Histologic examination revealed a 3.5 mm-sized, well differentiated adenocarcinoma invading the submucosa at a depth of 1.2 mm from the muscularis mucosa (sm1; thickness of submucosal layer 4 mm) (Fig. 1B). Since no lymph nodes were included within the perirectal fat, the pathologic stage was pT1NX. The nearest safety margin to carcinoma was 1.3 cm (deep margin). There was no definitive evidence of lymphatic invasion at first pathologic diagnosis, and she therefore received no additional therapy. In April 2008, an abdominal CT performed during routine follow-up revealed a 2 cm-sized nodular lesion in her perirectal fat (Fig. 2A). Anterior resection was performed, and histologic examination showed that this tumor, which involved the perirectal adipose tissue with no metastasis out of 15 regional lymph nodes (rpT0N1c), was compatible with a recurrence of the previous rectal cancer (Fig. 2B).
- Case 2 was a 53-year-old male patient with tenesmus that had undergone a colonoscopy, which revealed a 1 cm-sized flat-elevated lesion with central depression in the sigmoid colon, 25 cm from the anal verge (Fig. 3A). He underwent anterior resection in March 2004, and histologic examination showed that the tumor was a 5 mm-sized, moderately differentiated adenocarcinoma invading the submucosa (sm3) (Fig. 3B). The depth of submucosal invasion was 2.5 mm and the safety margin was at least 3 cm. No metastases were detected out of six pericolic lymph nodes, and the patient did not receive any adjuvant treatment. In February 2008, the patient developed widespread recurrence of the cancer (Fig. 4A) and underwent a low anterior resection with paraaortic lymph node dissection and segmental resection of the small intestine. Pathologic examination revealed a recurrent adenocarcinoma extended to the periureteral soft tissue and multiple metastases to the small intestine, regional and para-aortic lymph nodes (rpT4N2bM1b) (Fig. 4B).
- Retrospective pathologic review of the two primary carcinomas showed tumor buddings, defined as multiple foci of a single cancer cell and/or a micro-nest composed of several tumor cells, at the invasive front of both primary tumors (Fig. 5). A magnification of ×400 showed more than 10 foci in both primary tumors. In addition, small endolymphatic tumor emboli were detected only after deeper cutting of the paraffin blocks in both cases. These minute lymphatic invasion were not observed on the orginial hematoxylin and eosin slides. In both patients, the presence of tumor budding and lymphatic invasion was confirmed by immunohistochemical assays for cytokeratin and D2-40, respectively (Fig. 6). Immunohistochemical staining was performed using a mouse monoclonal antibody for cytokeratin (1:500, Dako, Glostrup, Denmark) and D2-40 (1:200, Dako).
CASE REPORTS
- Complete endoscopic resection of intramucosal carcinomas in the colorectum is regarded as curative, as there is no risk of lymph node metastasis.2,8 In contrast, lymph node metastasis is present in 6-12% of patients with SICC. Positive lymph node status has been reported to be the only significant independent predictor of 5-year cancer specific survival and 5-year disease-free survival in patients with pT1 and pT2 colorectal cancers.9 The standard of care for node-positive colorectal cancer patients is adjuvant chemotherapy based on 5-flourouracil regimens.10 Therefore, it is critical to evaluate the likelihood of lymph node metastasis in SICC. Poorly differentiated histology, presence of deep submucosal invasion, and lymphatic invasion are predictors of lymph node metastasis in patients with T1 colorectal cancer.3,6,7 Most T1 lesions without adverse pathologic features can be locally excised because the risks of local recurrence and lymph node metastasis are very low. However, a T1 lesion with unfavorable histologic features has a high risk of local recurrence and lymph node metastasis, whether metachronous or synchronous, indicating the need for additional treatment,2 since the prognosis is worse for patients who undergo additional surgery after local recurrence or lymph node metastasis.
- Tumor budding, or the presence of isolated single tumor cells or small cell clusters (up to 4 cells) scattered in the stroma at the invasive tumor margins, has been considered a malignant characteristic of colorectal carcinomas.11,12 Tumor budding is observed in many colorectal carcinomas and has been reported to be a useful predictor of patient outcome13,14 and lymph node metastasis6,7,12,13,15 in T1 colorectal cancer. Rectal cancer patients having a tumor budding intensity of >10 foci within a microscopic field of ×250 had lower 5-year survival rates than patients with tumor budding intensity of <10. Moreover, high-grade "tumor budding activity," defined as 10 or more foci in a microscopic field of ×200, has been closely associated with lymphatic involvement and lymph node metastasis in SICC.16 Immunophenotypically, loss of E-cadherin in budding cells of colorectal cancers has been reported, with loss of E-cadherin within the main tumor body being significantly associated with tumor budding.17
- Both patients described here had tumors with moderate to well differentiated histology and safety margins were sufficient for complete resection. However, recurrent disease developed within relatively short intervals. In the first patient, tumor recurrence without lymph node metastasis was observed 4.7 years after local tumor excision. In the second patient, both locoregional and systemic recurrences were observed 3.9 years after surgical resection, although lymph node metastasis was not identified in the primary tumor. Since a study of endoscopically-resected SICC demonstrated that recurrent primary cancers were significantly associated with poorly differentiated histology,18 we believed that other factors may have contributed to disease recurrence in these 2 patients. A thorough retrospective histologic review revealed frequent tumor budding from both tumors. Lymphatic channel permeation was not initially apparent on hematoxylin and eosin staining alone but was detected only after deeper cutting of the paraffin blocks and additional immunohistochemical assays. Similar to our patients was a patient with a submucosal invasive colon cancer of the pedunculated type, who developed lung metastasis 6 years after curative endoscopic polypectomy.19 The lesion was a 1 cm-sized, well differentiated adenocarcinoma showing tumor budding in the invasive front without lymphatic invasion, suggesting that tumor budding may be a significant prognostic factor for cancer recurrence and distant metastasis. Moreover, tumor budding may be closely associated with lymphatic channel involvement and lymph node metastasis. Although lymphatic invasion is regarded as an important prognostic factor for patients with SICC, lymphatic invasion may be subjective and be overestimated or underestimated due to retraction artifacts related to tissue processing for paraffin blocks.20 In contrast to angiolymphatic invasion, detection of tumor budding is more objective. Moreover, tumor budding may reflect early lymphatic invasion, even in the absence of definite lymphatic invasion. Consequently, meticulous pathologic examination is needed to detect tumor budding and angiolymphatic invasion in patients with SICC. Furthermore, immunohistochemical staining for D2-40 and cytokeratin may be helpful in detecting tumor budding and lymphatic channel permeation.
- To our knowledge, this is the first report of cases in Korea of SICC showing tumor budding with advanced recurrences. Multiple tumor budding at the invasive front may predict tumor aggressiveness in SICC. Further pathologic examination for lymphatic invasion such as deeper section or immunohistochemisty is needed in cases with SICC that have frequent tumor budding in which lymphatic invasion is not seen in the original hematoxylin and eosin slides. Besides, more aggressive follow-up is necessary for SICC patients showing tumor budding, even in the absence of unfavorable histologic findings. Other supplementary treatment measures, such as adjuvant chemotherapy, may be required to prevent recurrence and metastasis in these patients.
DISCUSSION
- 1. Tung SY, Wu CS, Wu MC, Su MY. Endoscopic treatment of colorectal polyps and early cancer. Dig Dis Sci 2001; 46: 1152-1156. ArticlePubMedPDF
- 2. Nivatvongs S. Surgical management of early colorectal cancer. World J Surg 2000; 24: 1052-1055. ArticlePubMedPDF
- 3. Kitajima K, Fujimori T, Fujii S, et al. Correlations between lymph node metastasis and depth of submucosal invasion in submucosal invasive colorectal carcinoma: a Japanese collaborative study. J Gastroenterol 2004; 39: 534-543. ArticlePubMedPDF
- 4. Egashira Y, Yoshida T, Hirata I, et al. Analysis of pathological risk factors for lymph node metastasis of submucosal invasive colon cancer. Mod Pathol 2004; 17: 503-511. ArticlePubMedPDF
- 5. Prall F. Tumour budding in colorectal carcinoma. Histopathology 2007; 50: 151-162. ArticlePubMed
- 6. Sohn DK, Chang HJ, Park JW, et al. Histopathological risk factors for lymph node metastasis in submucosal invasive colorectal carcinoma of pedunculated or semipedunculated type. J Clin Pathol 2007; 60: 912-915. ArticlePubMedPMC
- 7. Yamauchi H, Togashi K, Kawamura YJ, et al. Pathological predictors for lymph node metastasis in T1 colorectal cancer. Surg Today 2008; 38: 905-910. ArticlePubMedPDF
- 8. Kyzer S, Bégin LR, Gordon PH, Mitmaker B. The care of patients with colorectal polyps that contain invasive adenocarcinoma. Endoscopic polypectomy or colectomy? Cancer 1992; 70: 2044-2050. ArticlePubMed
- 9. Chok KS, Law WL. Prognostic factors affecting survival and recurrence of patients with pT1 and pT2 colorectal cancer. World J Surg 2007; 31: 1485-1490. ArticlePubMedPDF
- 10. Meyerhardt JA, Mayer RJ. Systemic therapy for colorectal cancer. N Engl J Med 2005; 352: 476-487. ArticlePubMed
- 11. Ueno H, Murphy J, Jass JR, Mochizuki H, Talbot IC. Tumour 'budding' as an index to estimate the potential of aggressiveness in rectal cancer. Histopathology 2002; 40: 127-132. ArticlePubMedPDF
- 12. Kazama S, Watanabe T, Ajioka Y, Kanazawa T, Nagawa H. Tumour budding at the deepest invasive margin correlates with lymph node metastasis in submucosal colorectal cancer detected by anticytokeratin antibody CAM5.2. Br J Cancer 2006; 94: 293-298. ArticlePubMedPMCPDF
- 13. Masaki T, Matsuoka H, Sugiyama M, et al. Budding as a useful determinant of the optimal treatment for T1 rectal carcinomas. Hepatogastroenterology 2003; 50: 388-391. PubMed
- 14. Prall F, Nizze H, Barten M. Tumour budding as prognostic factor in stage I/II colorectal carcinoma. Histopathology 2005; 47: 17-24. ArticlePubMed
- 15. Choi DH, Sohn DK, Chang HJ, Lim SB, Choi HS, Jeong SY. Indications for subsequent surgery after endoscopic resection of submucosally invasive colorectal carcinomas: a prospective cohort study. Dis Colon Rectum 2009; 52: 438-445. PubMed
- 16. Ogawa T, Yoshida T, Tsuruta T, et al. Tumor budding is predictive of lymphatic involvement and lymph node metastases in submucosal invasive colorectal adenocarcinomas and in non-polypoid compared with polypoid growths. Scand J Gastroenterol 2009; 44: 605-614. ArticlePubMed
- 17. Zlobec I, Lugli A, Baker K, et al. Role of APAF-1, E-cadherin and peritumoral lymphocytic infiltration in tumour budding in colorectal cancer. J Pathol 2007; 212: 260-268. PubMed
- 18. Nakada I, Tabuchi T, Nakachi T, et al. Histological factors contributing to a high risk of recurrence of submucosal invasive cancer (pT1) of the colon and rectum after endoscopic therapy. Surg Today 2008; 38: 675-678. ArticlePubMedPDF
- 19. Yasuda M, Torisu R, Misao T, et al. Ip-type submucosal invasive colonic cancer with lung metastasis 6 years after endoscopic polypectomy, report of a case. Stomach Intest 2003; 38: 769-774.
- 20. Compton CC, Fielding LP, Burgart LJ, et al. Prognostic factors in colorectal cancer. College of American Pathologists Consensus Statement 1999. Arch Pathol Lab Med 2000; 124: 979-994. PubMed
REFERENCES
Fig. 1Endoscopic and histologic findings of primary tumor in case 1. (A) Colonoscopic examination shows subpedunculated mass in the rectum with an ill-defined boundary. (B) Pathologic examination reveals a rectal cancer infiltrating the submucosa, with an adenoma component at the periphery.
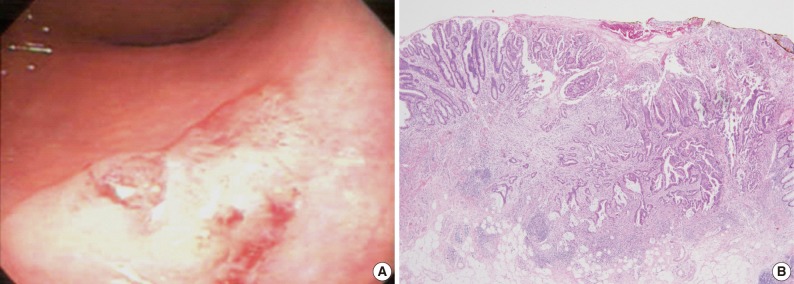
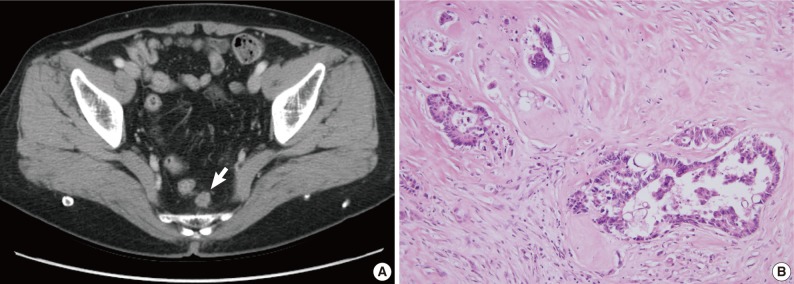
Fig. 2Radiologic and histologic findings of recurrent tumor in case 1. (A) A newly appeared soft tissue mass (arrow) in the perirectal tissue is detected upon computed tomographic imaging. (B) A perirectal mass shows an adenocarcinoma with intraluminal necrosis.

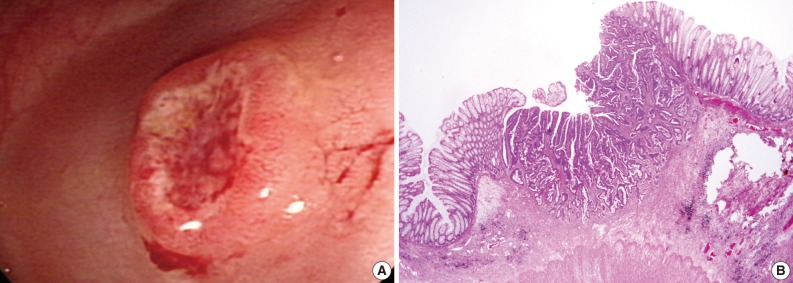
Fig. 3Endoscopic and histologic findings of primary tumor in case 2. (A) Colonoscopic examination shows an elevated tumor with central depression in the sigmoid colon. (B) Pathologic examination reveals a colon cancer invading the submucosa.
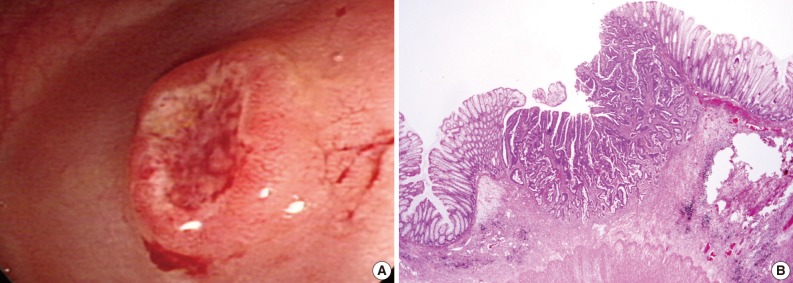
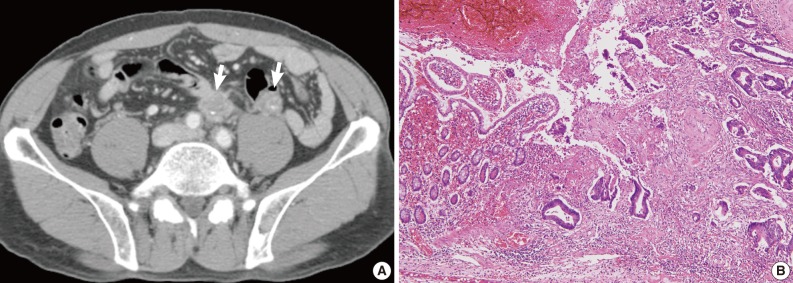
Fig. 4Radiologic and histologic findings of recurrent tumor in case 2. (A) Multiple metastatic lesions (arrows) in the para-aortic lymph node and mesentery are identified on computed tomographic imaging. (B) Adenocarcinoma involves the small intestinal mucosa, with similar histological findings to the original tumor (Fig. 2B).
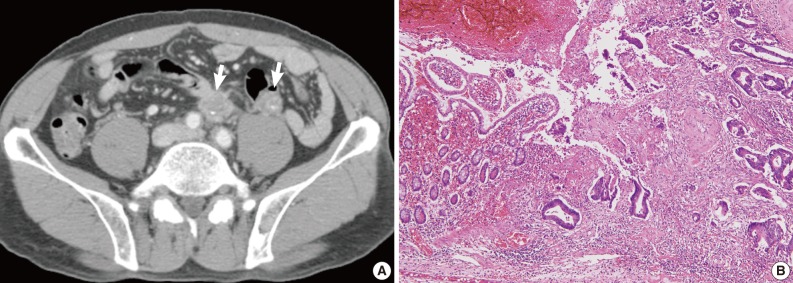
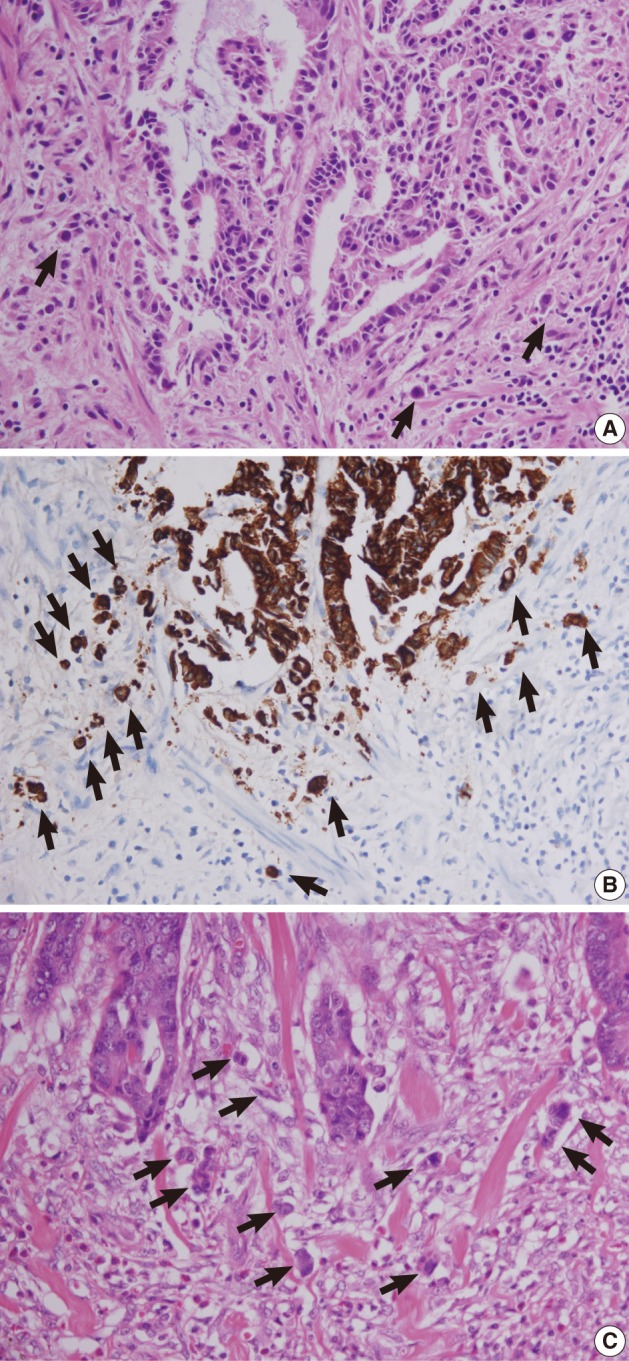

Figure & Data
References
Citations
Citations to this article as recorded by 
- Estudio de factores histológicos predictivos de metástasis ganglionar locorregional en adenocarcinoma colorrectal mínimamente invasivo pT1
Isidro Machado, Miriam Valera-Alberni, Fernando Martínez de Juan, José A. López-Guerrero, Alfonso García Fadrique, Julia Cruz, Carmen Martínez Lapiedra, Fernanda Maia de Alcantara, Ricardo Yaya, Jorge Campos, Carlos Fernández-Martos, Rafael Estevan
Gastroenterología y Hepatología.2016; 39(1): 1. CrossRef - Histological factors predicting loco-regional lymph node metastasis in early invasive colorectal adenocarcinoma pT1
Isidro Machado, Miriam Valera-Alberni, Fernando Martínez de Juan, José A. López-Guerrero, Alfonso García Fadrique, Julia Cruz, Carmen Martínez Lapiedra, Fernanda Maia de Alcantara, Ricardo Yaya, Jorge Campos, Carlos Fernández-Martos, Rafael Estevan
Gastroenterología y Hepatología (English Edition).2016; 39(1): 1. CrossRef - Tumor budding in the clinical management of colon and rectal cancer
Viktor H Koelzer, Inti Zlobec, Alessandro Lugli
Colorectal Cancer.2014; 3(4): 387. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article

Tumor Budding and Recurrence in Submucosal Invasive Colorectal Cancers of Favorable Histology: Case Reports of Two Early Colorectal Cancers with Advanced Recurrences






Fig. 1 Endoscopic and histologic findings of primary tumor in case 1. (A) Colonoscopic examination shows subpedunculated mass in the rectum with an ill-defined boundary. (B) Pathologic examination reveals a rectal cancer infiltrating the submucosa, with an adenoma component at the periphery.
Fig. 2 Radiologic and histologic findings of recurrent tumor in case 1. (A) A newly appeared soft tissue mass (arrow) in the perirectal tissue is detected upon computed tomographic imaging. (B) A perirectal mass shows an adenocarcinoma with intraluminal necrosis.
Fig. 3 Endoscopic and histologic findings of primary tumor in case 2. (A) Colonoscopic examination shows an elevated tumor with central depression in the sigmoid colon. (B) Pathologic examination reveals a colon cancer invading the submucosa.
Fig. 4 Radiologic and histologic findings of recurrent tumor in case 2. (A) Multiple metastatic lesions (arrows) in the para-aortic lymph node and mesentery are identified on computed tomographic imaging. (B) Adenocarcinoma involves the small intestinal mucosa, with similar histological findings to the original tumor (Fig. 2B).
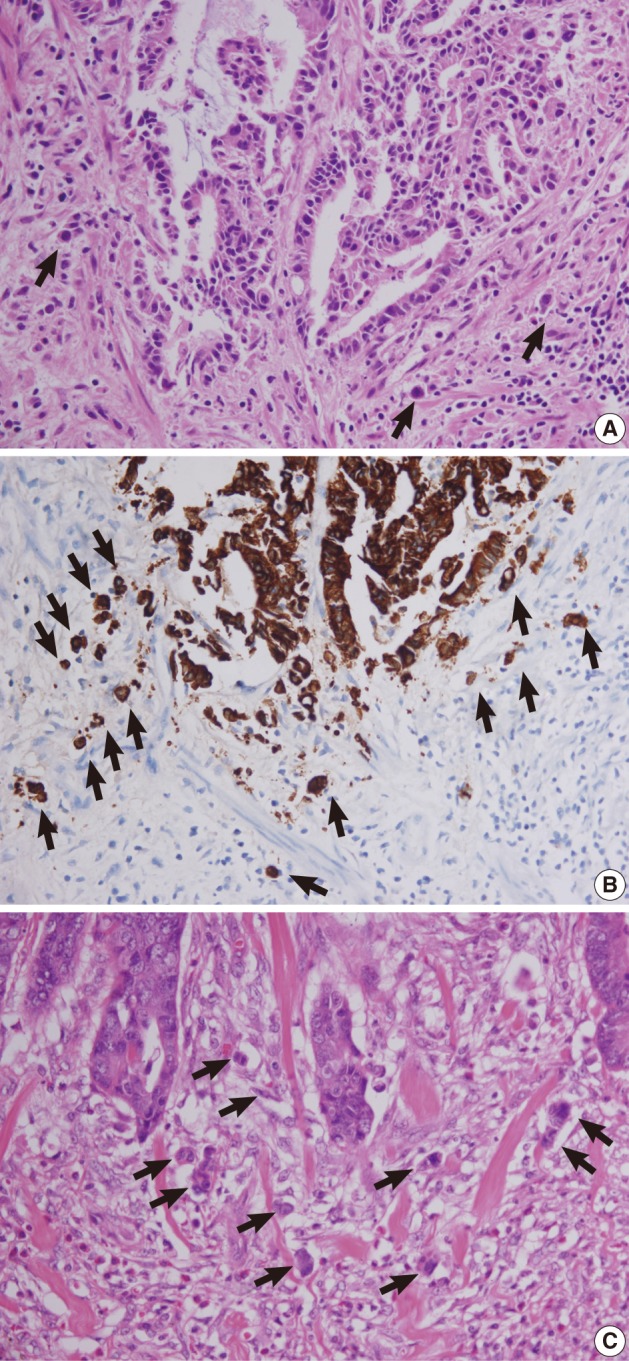
Fig. 5 Tumor buds at the invasive front of primary tumors (arrows). (A, B) In case 1, subtle budding cells (A) around the tumor margins are highlighted by immunohistochemistry using antibody to cytokeratin (B). (C) In case 2, frequent tumor budding is observed in a high power field.
Fig. 6 Lymphatic invasion in the primary tumors. (A, B) In case 1, several atypical cells are observed in the lymphatic channel (A) and proven to be carcinoma cells positive for cytokeratin (B). (C) In case 2, endolymphatic tumor emboli at the tumor border are confirmed by antibody to D2-40.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Tumor Budding and Recurrence in Submucosal Invasive Colorectal Cancers of Favorable Histology: Case Reports of Two Early Colorectal Cancers with Advanced Recurrences

