 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 57(4); 2023 > Article
-
Review
Reevaluating diagnostic categories and associated malignancy risks in thyroid core needle biopsy -
Chan Kwon Jung1,2

-
Journal of Pathology and Translational Medicine 2023;57(4):208-216.
DOI: https://doi.org/10.4132/jptm.2023.06.20
Published online: July 11, 2023
1Department of Hospital Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Cancer Research Institute, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Corresponding Author: Chan Kwon Jung, MD, PhD, Department of Pathology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea Tel: +82-2-2258-1622, Fax: +82-2-2258-1627, E-mail: ckjung@catholic.ac.kr
© 2023The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Abstract
- FORMAT OF THYROID CORE NEEDLE BIOPSY REPORTS
- RISK OF MALIGNANCY OF THYROID CORE NEEDLE BIOPSY DIAGNOSTIC CATEGORIES
- DIAGNOSTIC CHALLENGES IN FOLLICULAR-PATTERNED LESIONS ON CORE NEEDLE BIOPSY
- CLASSIFICATION OF FOLLICULAR-PATTERNED LESIONS USING MUTATION-SPECIFIC IMMUNOSTAINING IN CORE NEEDLE BIOPSY
- RISK STRATIFICATION OF PREOPERATIVELY DIAGNOSED INDETERMINATE FOLLICULAR-PATTERNED LESIONS
- CONCLUSION
- NOTES
- REFERENCES
Abstract
- As the application of core needle biopsy (CNB) in evaluating thyroid nodules rises in clinical practice, the 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules have officially recognized its value for the first time. CNB procures tissue samples preserving both histologic structure and cytologic detail, thereby supplying substantial material for an accurate diagnosis and reducing the necessity for repeated biopsies or subsequent surgical interventions. The current review introduces the risk of malignancy within distinct diagnostic categories, emphasizing the implications of noninvasive follicular thyroid neoplasm with papillary-like nuclear features on these malignancy risks. Prior research has indicated diagnostic challenges associated with follicular-patterned lesions, resulting in notable variation within indeterminate diagnostic categories. The utilization of mutation-specific immunostaining in CNB enhances the accuracy of lesion classification. This review underlines the essential role of a multidisciplinary approach in diagnosing follicular-patterned lesions and the potential of mutation-specific immunostaining to strengthen diagnostic consensus and inform patient management decisions.
- Thyroid CNB reports adhere to a structured format consisting of a diagnostic category, a subcategory, and a microscopic description (Table 1) [9]. The six diagnostic categories include (1) nondiagnostic (category I); (2) benign lesion (category II); (3) indeterminate lesion (category III); (4) follicular neoplasm (category IV); (5) suspicious for malignancy (category V); and (6) malignant (category VI). Categories III and IV are further divided into subcategories based on the status of nuclear atypia, architectural atypia, or oncocytic atypia. Subcategories that exhibit nuclear atypia (categories IIIa, IIIc, and IVb) raise concerns for conditions such as papillary thyroid carcinoma and NIFTP, which are typically associated with a higher ROM compared to subcategories that display architectural or oncocytic atypia [8,12-16].
FORMAT OF THYROID CORE NEEDLE BIOPSY REPORTS
- Based on retrospective studies in the literature, the frequency and ROM for each category are summarized in Table 2. The ROM estimates for each category are based on clinical follow-up and surgically resected nodules. Benign nodules within category II were clinically confirmed based on additional benign results from FNA or CNB and stable or reduced nodule size observed over a 1-year ultrasound follow-up period. Pathological confirmations on surgical specimens were used for nodules within categories I, III, IV, V, and VI.
- The method of estimating the cancer risk, which is based on histologic follow-up, overestimates the ROM, particularly for the categories I–III, where there is selection bias given the relatively small proportion of nodules that undergo excision. Although NIFTP is a surgical disease and cannot be preoperatively diagnosed on CNB or FNA specimens, the morphologic features of NIFTP tend to lead to classification on CNB/FNA as either category III, IV, or V, thereby impacting the resultant ROM calculations [13,14,17,18]. The ROM for each category is shown when including and excluding NIFTP in malignancy, information that might help guide more conservative clinical management of some nodules. The presence of NIFTP lowers the ROM within the diagnostic category of the thyroid CNB reporting system. The corresponding modifications in the ROM within categories III and IV have been deduced from the observed shifts in malignancy risk from three retrospective studies [13,14,17].
RISK OF MALIGNANCY OF THYROID CORE NEEDLE BIOPSY DIAGNOSTIC CATEGORIES
- CNB has emerged as a viable alternative to FNA, serving to decrease inconclusive results in the diagnosis of thyroid nodules. Nonetheless, follicular-patterned lesions presented in CNB continue to pose a significant challenge to pathologists, often falling within diagnostic categories II, III, or IV. The diagnostic rates of CNB categories may fluctuate based on pathologists’ diagnostic thresholds for follicular-patterned lesions [13,14,17].
- The histologic architecture and the status of the tumor capsule are critical determinants in diagnosing follicular-patterned lesions. Within the context of CNB specimens, follicular proliferative lesions characterized by a discernible tumor capsule are typically classified as category IV (follicular neoplasm) [9,10]. Conversely, in specimens where a tumor capsule is not apparent, these lesions are generally classified as category II (benign) in the absence of nuclear or architectural atypia, or category III (indeterminate follicular lesion) when nuclear or architectural atypia is present.
- In addition to the condition of the tumor capsule, the histologic architecture also plays a significant role in determining the diagnosis of follicular-patterned lesions. A microfollicular proliferative lesion, distinctly separated from the surrounding normal parenchyma by a fibrous capsule, leans towards a diagnosis of a category IV (follicular neoplasm). In contrast, a CNB specimen exhibiting a primarily microfollicular or trabecular growth pattern, but lacking a discernible fibrous capsule or adjacent nonlesional tissue, typically falls into category IIIb (indeterminate follicular lesion with architectural atypia). This categorization stems from the uncertainty regarding the presence of a tumor capsule in the lesion. This subcategory exhibits no nuclear atypia. However, certain pathologists might classify such cases under category IV, particularly when ultrasound imaging reveals a solitary nodule with a peripheral hypoechoic halo indicative of a tumor capsule. It is noteworthy that, even if a follicular-patterned lesion presents a definitive fibrous capsule, if the lesion exhibits a macrofollicular pattern rather than microfollicular or trabecular patterns, some pathologists might lean towards categorizing it as category III [15,16]. This preference is motivated by the understanding that a macrofollicular pattern is characteristic of benign thyroid diseases, even when a definitive fibrous capsule associated with a macrofollicular proliferative lesion is present.
- A comparison of the diagnostic categories from three major Korean hospitals, all of which perform a high volume of thyroid CNBs, reveals a noticeable variation. One hospital reported the frequencies of categories II, III, and IV as 38.1%, 17.6%, and 10.2%, respectively [14]. Another hospital reported the frequencies as 38.3%, 24.5%, and 7.6%, respectively [17]. Contrastingly, at our institution, the frequencies were markedly different at 60.9%, 1.2%, and 17.5%, respectively [13]. It is noteworthy that the occurrence of category III was significantly lower in our hospital than in the others, while the incidences of categories II and IV were comparatively higher in our hospital than the others.
- CNB tends to diagnose category IV “follicular neoplasms” more frequently than FNA [13,17,19], leading to an increased number of patients undergoing surgery based on CNB diagnoses compared to FNA. While the rate of follicular neoplasms diagnosed using CNB may differ significantly across various institutions, potentially due to the variability in how different observers interpret architectural or nuclear atypia in CNB, the ROMs found post-surgery for these follicular neoplasms remain consistent [13,14,17]. This consistency is observed irrespective of whether the initial diagnosis was made via CNB or FNA [13].
DIAGNOSTIC CHALLENGES IN FOLLICULAR-PATTERNED LESIONS ON CORE NEEDLE BIOPSY
- Immunostaining has served as an essential tool, supplementing standard methodologies in clarifying differential diagnoses in surgical pathology. This straightforward and economical technique facilitates the identification of lineage or cell type in histopathology and cytopathology. The recent emergence of innovative markers, particularly mutation-specific markers and those bearing translational significance, has substantially transformed the paradigm of immunohistochemistry (IHC). These progressive strides have notably influenced clinical practice and investigative pursuits within the field of thyroid disease.
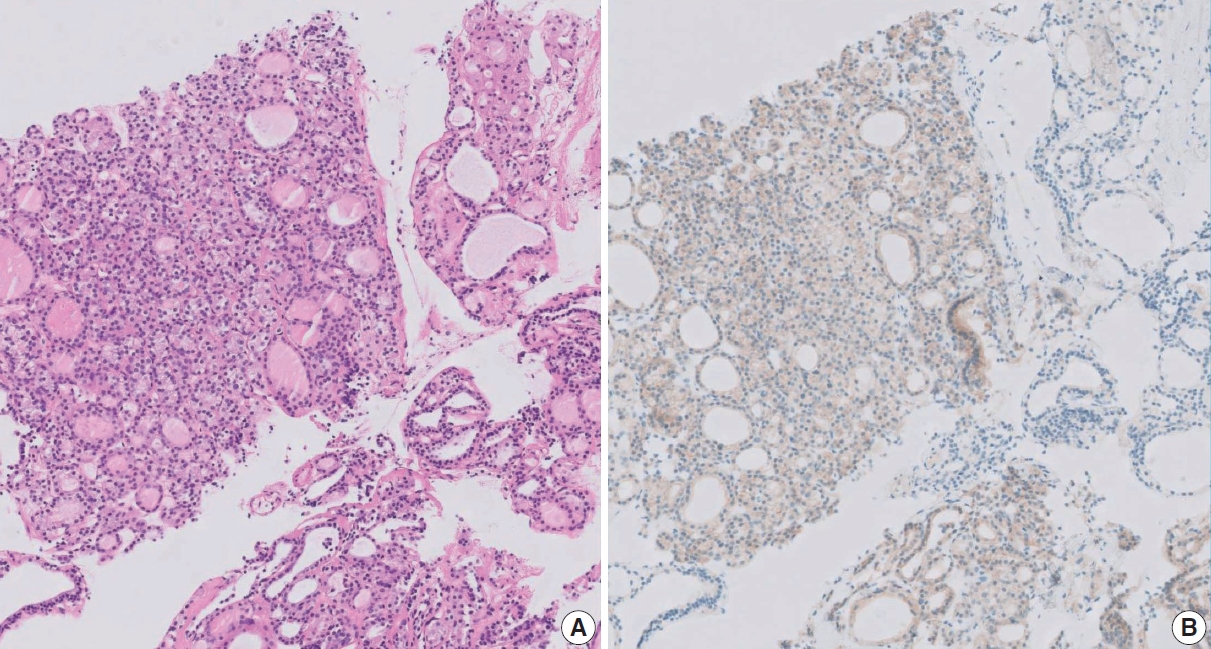
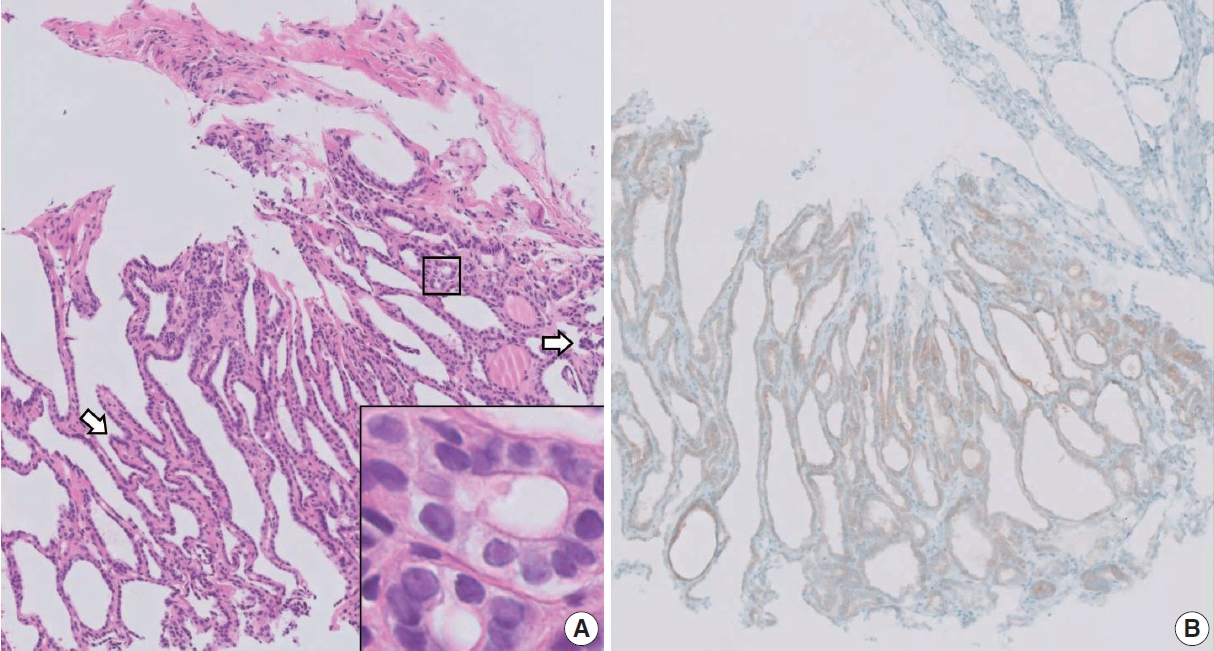
- The RAS genetic variants, typically found to be mutually exclusive with BRAF variants, are the most common oncogenic changes observed in follicular-patterned thyroid tumors [5,34,35]. Of all RAS variants identified in thyroid tumors, RAS Q61R is the most prevalent [8,36]. IHC for RAS Q61R, using the SP174 antibody, has proven to be an accurate method for detecting thyroid tumors harboring the RAS Q61R variant [8,37]. While RAS variants are not inherently sensitive or specific markers for thyroid cancers, their detection in preoperative FNA or CNB samples exhibiting indeterminate results usually prompts a diagnostic lobectomy. Thus, for CNB samples wherein histologic morphologies complicate the differential diagnosis between categories III and IV, a positive result for RAS Q61R IHC often simplifies the diagnostic process, favoring a categorization into category IV. In cases where a CNB specimen primarily displays a microfollicular or trabecular growth pattern without a discernible fibrous capsule, it is typically diagnosed as an indeterminate follicular lesion (category III). However, a positive RAS Q61R result in such a case could lead to a revised diagnosis of a follicular neoplasm (category IV) (Figs. 1, 2).
- When CNB samples display nuclear atypia yet lack sufficient histologic features for a definitive malignancy diagnosis, they may be assigned to category IIIa (Indeterminate follicular lesion with nuclear atypia) or category V (suspicious for malignancy) based on the extent of nuclear atypia and the quantity of atypical cells involved. In such situations, employing BRAF VE1 IHC to detect the BRAF p.V600E variant can be valuable for differential diagnosis (Fig. 3). Given the demonstrated reliability of BRAF VE1 IHC in identifying the BRAF p.V600E across different tumor types, including thyroid cancers [34,38], a positive result from this method has the potential to clarify indeterminate CNB results, typically pointing towards a definitive diagnosis of papillary thyroid carcinoma.
CLASSIFICATION OF FOLLICULAR-PATTERNED LESIONS USING MUTATION-SPECIFIC IMMUNOSTAINING IN CORE NEEDLE BIOPSY
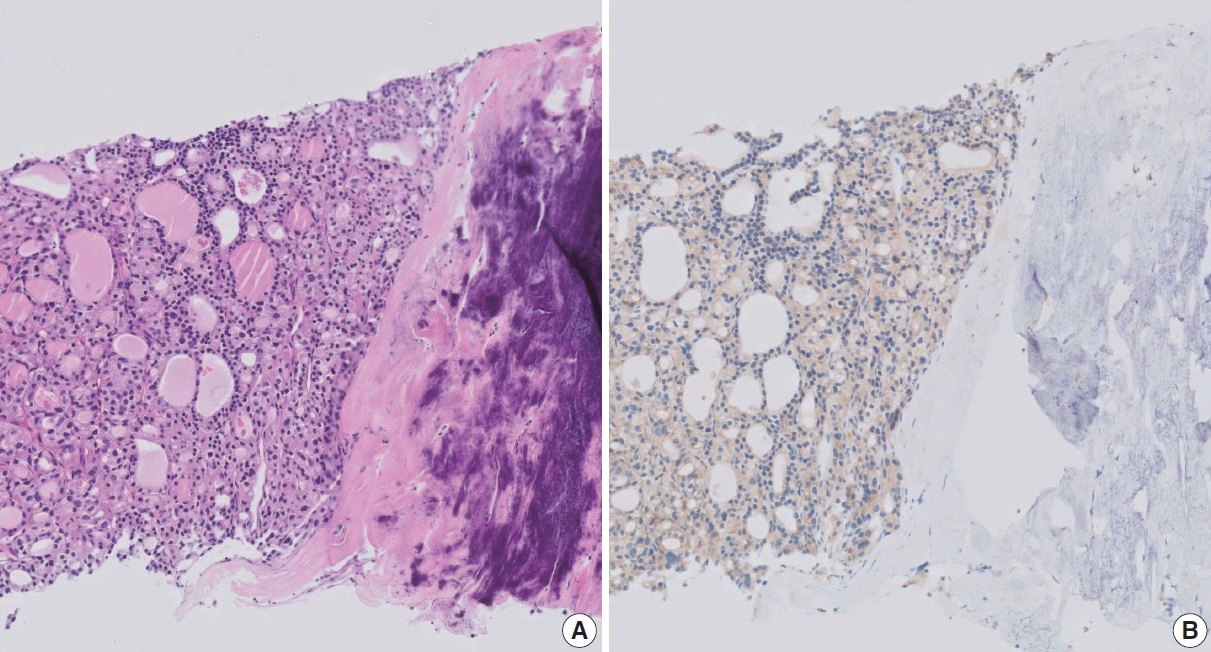
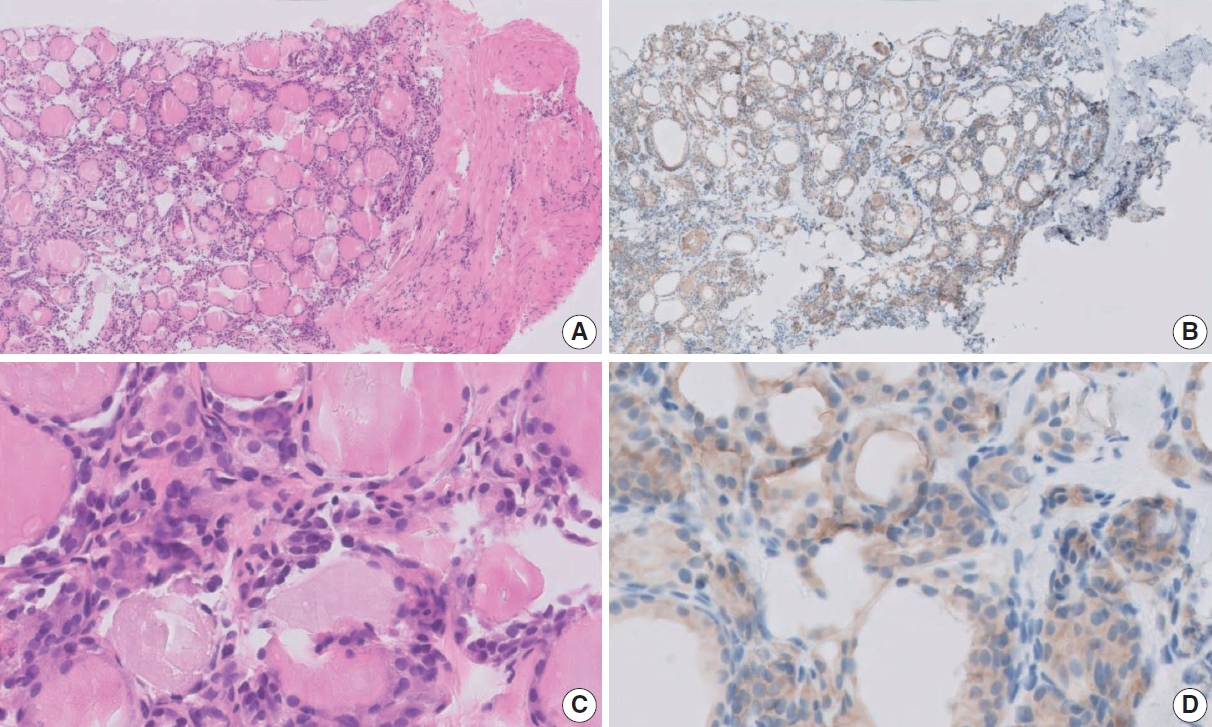
- Recently, our team established that CNB categories III and IV could be classified into two distinct risk groups based on histologic features of nuclear atypia and IHC for RAS Q61R [8]. CNBs exhibiting nuclear atypia or RAS Q61R expression were identified as high-risk, bearing an average NIFTP/malignancy risk of 75.5%. In contrast, CNBs without these findings were marked as low-risk, having a risk of approximately 34.9%. RAS Q61R IHC has shown high sensitivity and specificity for identifying the RAS p.Q61R variant and demonstrates a positive predictive value of 74.3% and a negative predictive value of 55.5% for diagnosing NIFTP/malignancy in CNB categories III and IV. Follicular lesions exhibiting both nuclear atypia and RAS Q61R expression carry an 86% NIFTP/malignancy risk. Therefore, in patients classified as CNB category III/IV, the presence of nuclear atypia or RAS Q61R expression signifies a heightened risk of NIFTP/malignancy, which may necessitate consideration for surgical resection (Figs. 4, 5). On the other hand, thyroid nodules lacking nuclear atypia and RAS Q61R expression, which present a lower likelihood of NIFTP/malignancy, might be suitable for observation without further intervention. This approach can potentially assist in the management of patients presenting with indeterminate CNB results.
- In patients preoperatively diagnosed with follicular neoplasm (category IV), nodule size plays a critical role in surgical decisionmaking due to the rising ROM associated with increasing nodule size. The 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules states that surgical intervention is typically favored for follicular neoplasms of 2 cm or more, given the escalating malignancy risk [11]. Even for tumors smaller than 2 cm, a malignancy risk exists, necessitating consideration of diagnostic surgery based on individual clinical findings [11]. A meta-analysis of 14 observational studies involving 2,016 thyroid nodules diagnosed as follicular neoplasms (category IV) demonstrated that in comparison to their smaller counterparts, nodules measuring 4 cm or larger, 3 cm or larger, and 2 cm or larger were associated with a respective 2.29-fold (95% confidence interval [CI], 1.68 to 3.11), 2.39-fold (95% CI, 1.45 to 3.95), and 1.63-fold (95% CI, 1.13 to 2.35) increase in ROM for thyroid nodules of various sizes [39-52].
- Molecular marker tests can facilitate malignancy assessment and inform decisions regarding ultrasound monitoring or surgical interventions. These decisions should account for patient preferences, clinical feasibility, and evaluations supplemented by ultrasound findings [20]. While next-generation sequencing (NGS)- based molecular panel testing is predominantly employed in Western countries, such molecular NGS testing for diagnostic or prognostic prediction on preoperative biopsy specimens is not currently permitted in Korea [11].
RISK STRATIFICATION OF PREOPERATIVELY DIAGNOSED INDETERMINATE FOLLICULAR-PATTERNED LESIONS
- The use of CNB for the evaluation of thyroid nodules has seen an increasing trend due to its potential as an alternative to FNA cytology. The 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules have recognized the value of CNB for the first time. Despite its advantages, the diagnosis of follicular-patterned lesions remains subject to interobserver variability. Therefore, a multidisciplinary approach emphasizing clinicopathologic correlation is essential. Furthermore, the utilization of mutation-specific immunostaining can enhance diagnostic consensus and contribute meaningfully to patient management by informing clinical decision-making processes.
CONCLUSION
Ethics Statement
Not applicable.
Availability of Data and Material
Data sharing not applicable to this article as no datasets were generated or analyzed during the study.
Code Availability
Not applicable.
Conflicts of Interest
C.K.J., the editor-in-chief of the Journal of Pathology and Translational Medicine, was not involved in the editorial evaluation or decision to publish this article.
Funding Statement
This research was supported by a grant (HI21C0940) from the Korean Health Technology R&D Project, Ministry of Health and Welfare, Republic of Korea.

Adapted with permission from Journal of Pathology and Translational Medicine [9].
| CNB diagnostic category | Diagnostic frequency (%)a | Risk of malignancy based on final diagnosis from clinical and/or surgical follow-up (%)b | Change in risk of malignancy due to NIFTPc |
|---|---|---|---|
| I. Nondiagnostic | 2 (2–3) | 33 (18–50) | No significant change |
| II. Benign lesion | 46 (40–53) | 4 (2–6) | No significant change |
| III. Indeterminate lesion | 10 (7–14) | 39 (32–45) | 24% Decrease (24%–34%) |
| IV. Follicular neoplasm | 7 (5–9) | 52 (46–57) | 20% Decrease (37%–45%) |
| V. Suspicious for malignancy | 2 (2–3) | 98 (96–100) | No significant change |
| VI. Malignant | 28 (23–34) | 100 | No significant change |
a95% Confidence intervals of pooled proportions from meta-analysis of literature [3-5,7,12-14,17,20-32];
bMeta-analysis based pooled proportions and 95% confidence intervals for confirmed clinical and surgical pathology follow-up [4,5,7,12-14,17,22,23,25-33];
cInfluence of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) on malignancy risk in thyroid core needle biopsy (CNB) diagnostic categories.
NIFTP appears to reduce the risk of malignancy in the diagnostic category of the thyroid CNB reporting system. The alterations in malignancy risk within categories III and IV were inferred from shifts in malignancy risk identified in three retrospective studies [13,14,17].
- 1. Na DG, Baek JH, Jung SL, et al. Core needle biopsy of the thyroid: 2016 consensus statement and recommendations from Korean Society of Thyroid Radiology. Korean J Radiol 2017; 18: 217-37. ArticlePubMedPMCPDF
- 2. Liu N, Meng Z, Jia Q, et al. Ultrasound-guided core needle biopsy for differential diagnosis of thyroid nodules: a systematic review and meta-analysis. Mol Clin Oncol 2017; 6: 825-32. ArticlePubMedPMC
- 3. Trimboli P, Nasrollah N, Guidobaldi L, et al. The use of core needle biopsy as first-line in diagnosis of thyroid nodules reduces false negative and inconclusive data reported by fine-needle aspiration. World J Surg Oncol 2014; 12: 61.ArticlePubMedPMCPDF
- 4. Suh CH, Baek JH, Lee JH, et al. The role of core-needle biopsy as a first-line diagnostic tool for initially detected thyroid nodules. Thyroid 2016; 26: 395-403. ArticlePubMed
- 5. Kim HC, Kim YJ, Han HY, et al. First-line use of core needle biopsy for high-yield preliminary diagnosis of thyroid nodules. AJNR Am J Neuroradiol 2017; 38: 357-63. ArticlePubMedPMC
- 6. Zhang M, Zhang Y, Fu S, Lv F, Tang J. Thyroid nodules with suspicious ultrasound findings: the role of ultrasound-guided core needle biopsy. Clin Imaging 2014; 38: 434-8. ArticlePubMed
- 7. Ahn HS, Youn I, Na DG, Kim SJ, Lee MY. Diagnostic performance of core needle biopsy as a first-line diagnostic tool for thyroid nodules according to ultrasound patterns: Comparison with fine needle aspiration using propensity score matching analysis. Clin Endocrinol (Oxf) 2021; 94: 494-503. ArticlePubMedPDF
- 8. Kim M, Jeon S, Jung CK. Preoperative risk stratification of follicular-patterned thyroid lesions on core needle biopsy by histologic subtyping and RAS variant-specific immunohistochemistry. Endocr Pathol 2023; 34: 247-56. ArticlePubMedPDF
- 9. Jung CK, Baek JH, Na DG, Oh YL, Yi KH, Kang HC. 2019 Practice guidelines for thyroid core needle biopsy: a report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association. J Pathol Transl Med 2020; 54: 64-86. ArticlePubMedPMCPDF
- 10. Jung CK, Min HS, Park HJ, et al. Pathology reporting of thyroid core needle biopsy: a proposal of the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group. J Pathol Transl Med 2015; 49: 288-99. ArticlePubMedPMCPDF
- 11. Park YJ, Lee EK, Song YS, et al. 2023 Korean Thyroid Association management guidelines for patients with thyroid nodules. Int J Thyroidol 2023; 16: 1-31. Article
- 12. Choe J, Baek JH, Park HS, Choi YJ, Lee JH. Core needle biopsy of thyroid nodules: outcomes and safety from a large single-center single-operator study. Acta Radiol 2018; 59: 924-31. ArticlePubMedPDF
- 13. Kim K, Bae JS, Kim JS, Jung SL, Jung CK. Diagnostic performance of thyroid core needle biopsy using the revised reporting system: comparison with fine needle aspiration cytology. Endocrinol Metab (Seoul) 2022; 37: 159-69. ArticlePubMedPMCPDF
- 14. Na HY, Woo JW, Moon JH, et al. Preoperative diagnostic categories of noninvasive follicular thyroid neoplasm with papillary-like nuclear features in thyroid core needle biopsy and its impact on risk of malignancy. Endocr Pathol 2019; 30: 329-39. ArticlePubMedPDF
- 15. Ahn SH, Park SY, Choi SI. Comparison of consecutive results from fine needle aspiration and core needle biopsy in thyroid nodules. Endocr Pathol 2017; 28: 332-8. ArticlePubMedPDF
- 16. Yoon RG, Baek JH, Lee JH, et al. Diagnosis of thyroid follicular neoplasm: fine-needle aspiration versus core-needle biopsy. Thyroid 2014; 24: 1612-7. ArticlePubMed
- 17. Chung SR, Baek JH, Lee JH, et al. Risk of malignancy according to the sub-classification of atypia of undetermined significance and suspicious follicular neoplasm categories in thyroid core needle biopsies. Endocr Pathol 2019; 30: 146-54. ArticlePubMedPDF
- 18. Na HY, Park SY. Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: its updated diagnostic criteria, preoperative cytologic diagnoses and impact on the risk of malignancy. J Pathol Transl Med 2022; 56: 319-25. ArticlePubMedPMCPDF
- 19. Ahn SH. Usage and diagnostic yield of fine-needle aspiration cytology and core needle biopsy in thyroid nodules: a systematic review and meta-analysis of literature published by Korean authors. Clin Exp Otorhinolaryngol 2021; 14: 116-30. ArticlePubMedPDF
- 20. Son HM, Kim JH, Kim SC, et al. Distribution and malignancy risk of six categories of the pathology reporting system for thyroid coreneedle biopsy in 1,216 consecutive thyroid nodules. Ultrasonography 2020; 39: 159-65. ArticlePubMedPMCPDF
- 21. Suh CH, Baek JH, Choi YJ, et al. Efficacy and safety of core-needle biopsy in initially detected thyroid nodules via propensity score analysis. Sci Rep 2017; 7: 8242.ArticlePubMedPMCPDF
- 22. Ahn HS, Seo M, Ha SM, Kim HS. Comparison of the diagnostic efficacy of ultrasound-guided core needle biopsy with 18- versus 20-gauge needles for thyroid nodules. J Ultrasound Med 2018; 37: 2565-74. ArticlePubMedPDF
- 23. Choe JY, Kwak Y, Kim M, et al. Utility of a formatted pathologic reporting system in thyroid core needle biopsy: a validation study of 1998 consecutive cases. Clin Endocrinol (Oxf) 2018; 88: 96-104. ArticlePubMedPDF
- 24. Chung SR, Baek JH, Park HS, et al. Ultrasound-pathology discordant nodules on core-needle biopsy: malignancy risk and management strategy. Thyroid 2017; 27: 707-13. ArticlePubMed
- 25. Ha EJ, Baek JH, Lee JH, et al. Core needle biopsy can minimise the non-diagnostic results and need for diagnostic surgery in patients with calcified thyroid nodules. Eur Radiol 2014; 24: 1403-9. ArticlePubMedPDF
- 26. Ha EJ, Baek JH, Lee JH, et al. Sonographically suspicious thyroid nodules with initially benign cytologic results: the role of a core needle biopsy. Thyroid 2013; 23: 703-8. ArticlePubMed
- 27. Joo L, Na DG, Kim JH, Seo H. Comparison of core needle biopsy and repeat fine-needle aspiration in avoiding diagnostic surgery for thyroid nodules initially diagnosed as atypia/follicular lesion of undetermined significance. Korean J Radiol 2022; 23: 280-8. ArticlePubMedPMCPDF
- 28. Kim YH, Kwon HJ, Kim EK, Kwak JY, Moon HJ, Yoon JH. Applying ultrasound-guided core needle biopsy for diagnosis of thyroid masses: preliminary results from a single institution. J Ultrasound Med 2015; 34: 1801-8. PubMed
- 29. Park JY, Yi SY, Baek SH, Lee YH, Kwon HJ, Park HJ. Diagnostic efficacy, performance and safety of side-cut core needle biopsy for thyroid nodules: comparison of automated and semi-automated biopsy needles. Endocrine 2022; 76: 341-8. ArticlePubMedPDF
- 30. Sung JY, Na DG, Kim KS, et al. Diagnostic accuracy of fine-needle aspiration versus core-needle biopsy for the diagnosis of thyroid malignancy in a clinical cohort. Eur Radiol 2012; 22: 1564-72. ArticlePubMedPDF
- 31. Xiong Y, Yan L, Nong L, Zheng Y, Li T. Pathological diagnosis of thyroid nodules based on core needle biopsies: comparative study between core needle biopsies and resected specimens in 578 cases. Diagn Pathol 2019; 14: 10.ArticlePubMedPMCPDF
- 32. Hong MJ, Na DG, Kim SJ, Kim DS. Role of core needle biopsy as a first-line diagnostic tool for thyroid nodules: a retrospective cohort study. Ultrasonography 2018; 37: 244-53. ArticlePubMedPDF
- 33. Suh CH, Baek JH, Lee JH, et al. The role of core-needle biopsy in the diagnosis of thyroid malignancy in 4580 patients with 4746 thyroid nodules: a systematic review and meta-analysis. Endocrine 2016; 54: 315-28. ArticlePubMedPDF
- 34. Agarwal S, Bychkov A, Jung CK. Emerging biomarkers in thyroid practice and research. Cancers (Basel) 2021; 14: 204.ArticlePubMedPMC
- 35. Jung CK, Bychkov A, Kakudo K. Update from the 2022 World Health Organization classification of thyroid tumors: a standardized diagnostic approach. Endocrinol Metab (Seoul) 2022; 37: 703-18. ArticlePubMedPMCPDF
- 36. Burge RA, Hobbs GA. Chapter two - Not all RAS mutations are equal: a detailed review of the functional diversity of RAS hot spot mutations.In: O’Bryan JP, Piazza GA, eds. Advances in Cancer Research. Vol. 153. New York: Academic Press, 2022; 29-61.
- 37. Saliba M, Katabi N, Dogan S, Xu B, Ghossein RA. NRAS Q61R immunohistochemical staining in thyroid pathology: sensitivity, specificity and utility. Histopathology 2021; 79: 650-60. ArticlePubMedPMCPDF
- 38. Chang S, Choi YL, Shim HS, Lee GK, Ha SY; Korean Cardiopulmonary Pathology Study Group. Usefulness of BRAF VE1 immunohistochemistry in non-small cell lung cancers: a multi-institutional study by 15 pathologists in Korea. J Pathol Transl Med 2022; 56: 334-41. ArticlePubMedPMCPDF
- 39. Baloch ZW, Fleisher S, LiVolsi VA, Gupta PK. Diagnosis of “follicular neoplasm”: a gray zone in thyroid fine-needle aspiration cytology. Diagn Cytopathol 2002; 26: 41-4. ArticlePubMed
- 40. Choi YJ, Yun JS, Kim DH. Clinical and ultrasound features of cytology diagnosed follicular neoplasm. Endocr J 2009; 56: 383-9. ArticlePubMed
- 41. Giorgadze T, Rossi ED, Fadda G, Gupta PK, Livolsi VA, Baloch Z. Does the fine-needle aspiration diagnosis of “Hurthle-cell neoplasm/ follicular neoplasm with oncocytic features” denote increased risk of malignancy? Diagn Cytopathol 2004; 31: 307-12. PubMed
- 42. Gulcelik NE, Gulcelik MA, Kuru B. Risk of malignancy in patients with follicular neoplasm: predictive value of clinical and ultrasonographic features. Arch Otolaryngol Head Neck Surg 2008; 134: 1312-5. ArticlePubMed
- 43. Kim HJ, Mok JO, Kim CH, et al. Preoperative serum thyroglobulin and changes in serum thyroglobulin during TSH suppression independently predict follicular thyroid carcinoma in thyroid nodules with a cytological diagnosis of follicular lesion. Endocr Res 2017; 42: 154-62. ArticlePubMed
- 44. Kuru B, Kefeli M. Risk factors associated with malignancy and with triage to surgery in thyroid nodules classified as Bethesda category IV (FN/SFN). Diagn Cytopathol 2018; 46: 489-94. ArticlePubMedPDF
- 45. Lubitz CC, Faquin WC, Yang J, et al. Clinical and cytological features predictive of malignancy in thyroid follicular neoplasms. Thyroid 2010; 20: 25-31. ArticlePubMed
- 46. Parikh PP, Allan BJ, Lew JI. Surgeon-performed ultrasound predictors of malignancy in patients with Hurthle cell neoplasms of the thyroid. J Surg Res 2013; 184: 247-52. PubMed
- 47. Petric R, Perhavec A, Gazic B, Besic N. Preoperative serum thyroglobulin concentration is an independent predictive factor of malignancy in follicular neoplasms of the thyroid gland. J Surg Oncol 2012; 105: 351-6. ArticlePubMedPDF
- 48. Raber W, Kaserer K, Niederle B, Vierhapper H. Risk factors for malignancy of thyroid nodules initially identified as follicular neoplasia by fine-needle aspiration: results of a prospective study of one hundred twenty patients. Thyroid 2000; 10: 709-12. ArticlePubMed
- 49. Raparia K, Min SK, Mody DR, Anton R, Amrikachi M. Clinical outcomes for “suspicious” category in thyroid fine-needle aspiration biopsy: patient’s sex and nodule size are possible predictors of malignancy. Arch Pathol Lab Med 2009; 133: 787-90. ArticlePubMedPDF
- 50. Roth MY, Witt RL, Steward DL. Molecular testing for thyroid nodules: review and current state. Cancer 2018; 124: 888-98. ArticlePubMedPDF
- 51. Tuttle RM, Lemar H, Burch HB. Clinical features associated with an increased risk of thyroid malignancy in patients with follicular neoplasia by fine-needle aspiration. Thyroid 1998; 8: 377-83. ArticlePubMed
- 52. Williams MD, Suliburk JW, Staerkel GA, et al. Clinical significance of distinguishing between follicular lesion and follicular neoplasm in thyroid fine-needle aspiration biopsy. Ann Surg Oncol 2009; 16: 3146-53. ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
- Evaluation and Management of Thyroid Nodules: A Joint Consensus Statement From the British Thyroid Association (BTA), British Association of Endocrine and Thyroid Surgeons (BAETS) and Collaborating Bodies
Ram Moorthy, Saba P. Balasubramanian, Kate Farnell, Mairead Kelly, Gitta Madani, Mufaddal Moonim, Carla Moran, Julia Priestley, Michael Stechman, Emma Watts, Kristien Boelaert
Clinical Endocrinology.2026; 104(6): 682. CrossRef - Advantages of thyroid core needle biopsy: an emerging selective first-line biopsy modality
Jae Ho Shin, Yeseul Kim, Min Kyoung Lee, Jung Hwan Baek, So Lyung Jung
Ultrasonography.2026; 45(3): 205. CrossRef - Lessons learned from the first 2 years of experience with thyroid core needle biopsy at an Indonesian national referral hospital
Agnes Stephanie Harahap, Maria Francisca Ham, Retno Asti Werdhani, Erwin Danil Julian, Rafi Ilmansyah, Chloe Indira Arfelita Mangunkusumso, Tri Juli Edi Tarigan
Journal of Pathology and Translational Medicine.2025; 59(3): 149. CrossRef - Risk Stratification of Thyroid Nodules Diagnosed as Follicular Neoplasm on Core Needle Biopsy
Byeong-Joo Noh, Won Jun Kim, Jin Yub Kim, Ha Young Kim, Jong Cheol Lee, Myoung Sook Shim, Yong Jin Song, Kwang Hyun Yoon, In-Hye Jung, Hyo Sang Lee, Wooyul Paik, Dong Gyu Na
Endocrinology and Metabolism.2025; 40(4): 610. CrossRef - Diagnostic implication of thyroid spherules for cytological diagnosis of thyroid nodules
Heeseung Sohn, Kennichi Kakudo, Chan Kwon Jung
Cytopathology.2024; 35(3): 383. CrossRef - A Narrative Review of the 2023 Korean Thyroid Association Management Guideline for Patients with Thyroid Nodules
Eun Kyung Lee, Young Joo Park, Chan Kwon Jung, Dong Gyu Na
Endocrinology and Metabolism.2024; 39(1): 61. CrossRef - The Diagnostic Role of Repeated Biopsy of Thyroid Nodules with Atypia of Undetermined Significance with Architectural Atypia on Core-Needle Biopsy
Hye Hyeon Moon, Sae Rom Chung, Young Jun Choi, Tae-Yon Sung, Dong Eun Song, Tae Yong Kim, Jeong Hyun Lee, Jung Hwan Baek
Endocrinology and Metabolism.2024; 39(2): 300. CrossRef - Core needle biopsy for thyroid nodules assessment-a new horizon?
David D Dolidze, Serghei Covantsev, Grigorii M Chechenin, Natalia V Pichugina, Anastasia V Bedina, Anna Bumbu
World Journal of Clinical Oncology.2024; 15(5): 580. CrossRef - Educational exchange in thyroid core needle biopsy diagnosis: enhancing pathological interpretation through guideline integration and peer learning
Agnes Stephanie Harahap, Chan Kwon Jung
Journal of Pathology and Translational Medicine.2024; 58(5): 205. CrossRef - A simplified four-tier classification for thyroid core needle biopsy
M. Paja, J. L. Del Cura, R. Zabala, I. Korta, Mª T. Gutiérrez, A. Expósito, A. Ugalde
Journal of Endocrinological Investigation.2024; 48(4): 895. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
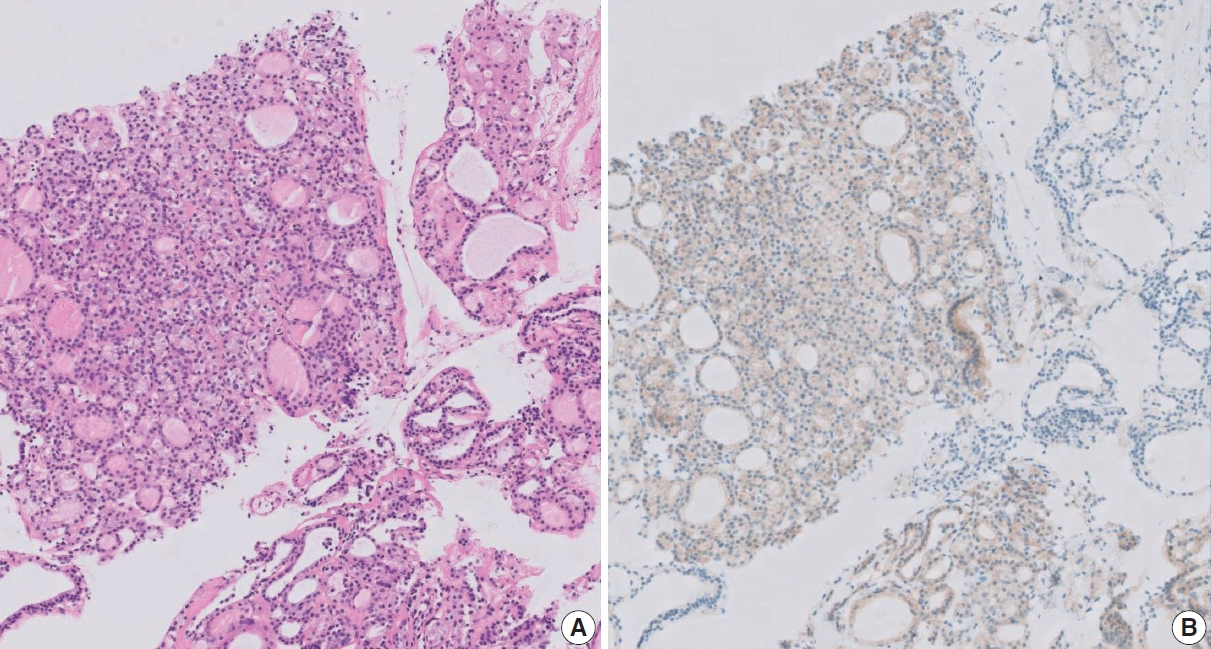
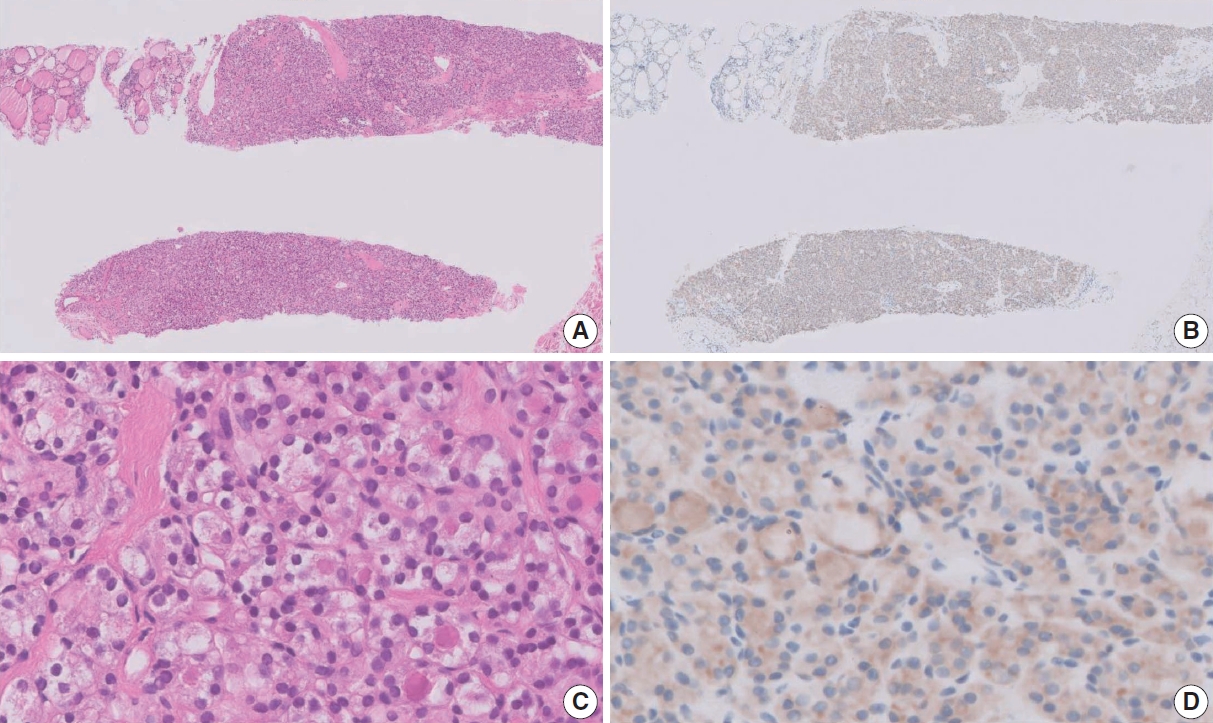
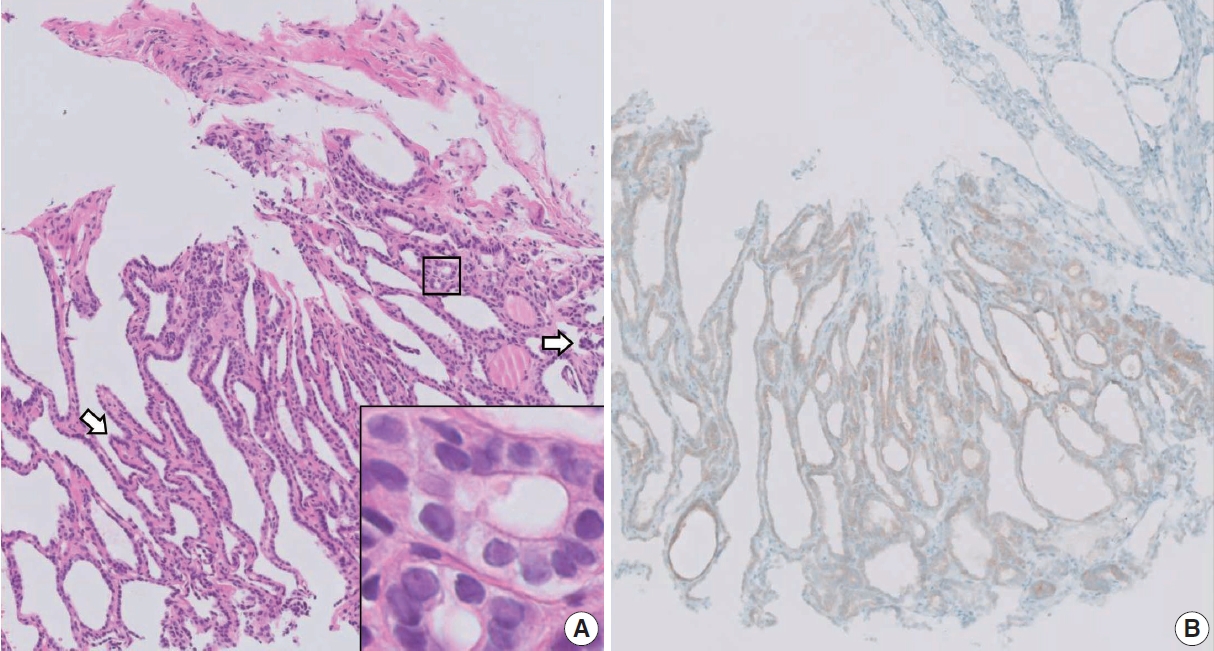
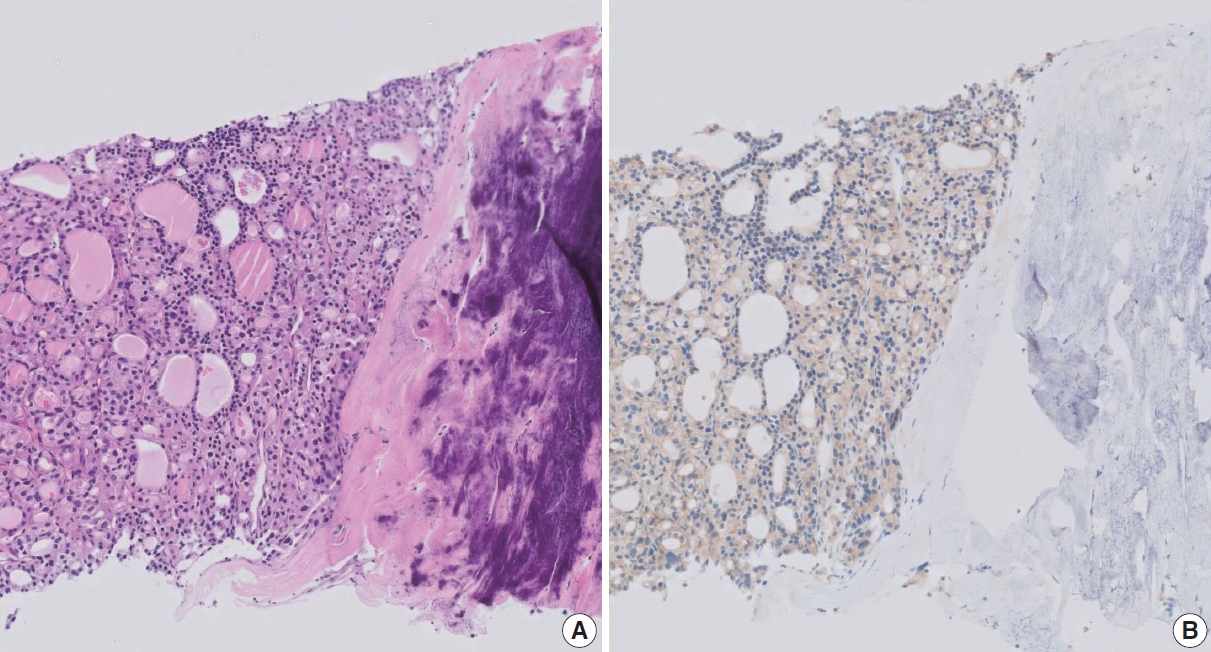
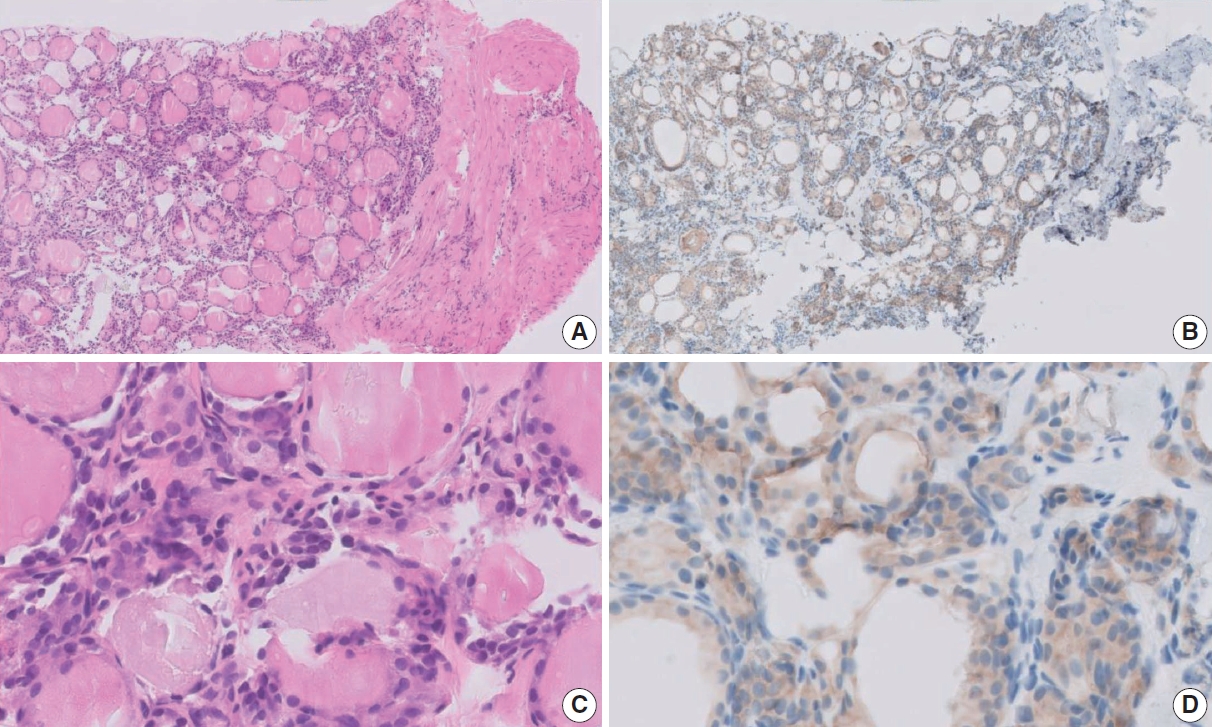





Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
| Diagnostic category | |
|---|---|
| Category I. Nondiagnostic or unsatisfactory | |
| Non-tumor adjacent thyroid tissue only | |
| Extrathyroid tissue only (e.g., skeletal muscle, mature adipose tissue) | |
| Acellular specimen (e.g., acellular fibrotic tissue, acellular hyalinized tissue, cystic fluid only) | |
| Blood clot only | |
| Other | |
| Category II. Benign lesion | |
| Benign follicular nodule | |
| Hashimoto’s thyroiditis | |
| Subacute granulomatous thyroiditis | |
| Nonthyroidal lesion (e.g., parathyroid lesions, benign neurogenic tumors, benign lymph node) | |
| Other | |
| Category III. Indeterminate lesion | |
| IIIa. Indeterminate follicular lesion with nuclear atypia | |
| IIIb. Indeterminate follicular lesion with architectural atypia | |
| IIIc. Indeterminate follicular lesion with nuclear and architectural atypia | |
| IIId. Indeterminate follicular lesion with oncocytic atypia | |
| IIIe. Indeterminate lesion, not otherwise specified | |
| Category IV. Follicular neoplasm | |
| IVa. Follicular neoplasm, conventional type | |
| IVb. Follicular neoplasm with nuclear atypia | |
| IVc. Oncocytic (Hürthle cell) neoplasm | |
| IVd. Follicular neoplasm, not otherwise specified | |
| Category V. Suspicious for malignancy | |
| Suspicious for papillary thyroid carcinoma, medullary thyroid carcinoma, poorly differentiated thyroid carcinoma, metastatic carcinoma, lymphoma, etc. | |
| Category VI. Malignant | |
| Papillary thyroid carcinoma, poorly differentiated thyroid carcinoma, differentiated high-grade thyroid carcinoma, anaplastic thyroid carcinoma, medullary thyroid carcinoma, lymphoma, metastatic carcinoma, etc | |
| CNB diagnostic category | Diagnostic frequency (%) |
Risk of malignancy based on final diagnosis from clinical and/or surgical follow-up (%) |
Change in risk of malignancy due to NIFTP |
|---|---|---|---|
| I. Nondiagnostic | 2 (2–3) | 33 (18–50) | No significant change |
| II. Benign lesion | 46 (40–53) | 4 (2–6) | No significant change |
| III. Indeterminate lesion | 10 (7–14) | 39 (32–45) | 24% Decrease (24%–34%) |
| IV. Follicular neoplasm | 7 (5–9) | 52 (46–57) | 20% Decrease (37%–45%) |
| V. Suspicious for malignancy | 2 (2–3) | 98 (96–100) | No significant change |
| VI. Malignant | 28 (23–34) | 100 | No significant change |
Adapted with permission from
95% Confidence intervals of pooled proportions from meta-analysis of literature [ Meta-analysis based pooled proportions and 95% confidence intervals for confirmed clinical and surgical pathology follow-up [ Influence of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) on malignancy risk in thyroid core needle biopsy (CNB) diagnostic categories. NIFTP appears to reduce the risk of malignancy in the diagnostic category of the thyroid CNB reporting system. The alterations in malignancy risk within categories III and IV were inferred from shifts in malignancy risk identified in three retrospective studies [

