 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 57(3); 2023 > Article
-
Original Article
Frequent apocrine changes in pleomorphic adenoma with malignant transformation: a possible pre-malignant step in ductal carcinoma ex pleomorphic adenoma -
Joon Seon Song1
 , Yeseul Kim1, Yoon-Se Lee2, Seung-Ho Choi2, Soon Yuhl Nam2, Sang Yoon Kim2, Kyung-Ja Cho1
, Yeseul Kim1, Yoon-Se Lee2, Seung-Ho Choi2, Soon Yuhl Nam2, Sang Yoon Kim2, Kyung-Ja Cho1 -
Journal of Pathology and Translational Medicine 2023;57(3):158-165.
DOI: https://doi.org/10.4132/jptm.2023.03.13
Published online: May 10, 2023
1Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
2Department of Otorhinolaryngology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Corresponding Author: Kyung-Ja Cho, MD, PhD, Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Seoul 05505, Korea Tel: +82-2-3010-4545, Fax: +82-2-472-7898, E-mail: kjc@amc.seoul.kr
© 2023The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- The most common type of carcinoma ex pleomorphic adenoma (CPA) is histologically equivalent to salivary duct carcinoma, which has an apocrine phenotype. Invasive CPA is often accompanied by non-invasive or in situ carcinoma, an observation that suggests the presence of precursor lesions. The aim of this study was to identify candidate precursor lesions of CPA within pleomorphic adenoma (PA).
-
Methods
- Eleven resected cases of CPA with residual PA and 17 cases of PA with atypical changes were subjected to immunohistochemistry (IHC) for p53, human epidermal growth factor receptor 2 (HER2), androgen receptor (AR), pleomorphic adenoma gene 1, gross cystic disease fluid protein-15 (GCDFP-15), and anti-mitochondrial antibody.
-
Results
- Invasive or in situ carcinoma cells in all CPAs were positive for AR, GCDFP-15, and HER2. Atypical foci in PAs corresponded to either apocrine or oncocytic changes on the basis of their reactivity to AR, GCDFP-15, and anti-mitochondrial antibody. Atypical cells in PAs surrounding CPAs had an apocrine phenotype without HER2 expression.
-
Conclusions
- Our study identified frequent apocrine changes in residual PAs in CPA cases, suggesting a possible precursor role of apocrine changes. We recommend the use of HER2 IHC in atypical PAs, and that clinicians take HER2 positivity into serious consideration.
- Case selection
- Five resected cases of CPAs with both invasive and in situ carcinoma (CisPA) and residual PA and six cases of CisPA only with residual PA were selected from among 32 luminal-type CPA specimens collected at the Asan Medical Center, Seoul, Korea, between 2006 and 2017. Twenty-one cases without in situ carcinoma or residual PA, and 20 abluminal-type CPAs from the same period were excluded from the study. CisPAs were defined by the presence of areas of intratubular growth of markedly atypical cells, with expansion and distortion of surrounding myoepithelial frames. Seventeen resected cases of PA with atypical changes were selected from the same period at random. The presence of cellular enlargement with nuclear pleomorphism, hyperchromasia, and prominent nucleoli, without structural abnormality, was regarded as atypical change in PA.
- Immunohistochemistry
- Representative areas from 28 cases were subjected to immunohistochemistry for p53 (1:1,500, clone DO-7, DAKO, Glostrup, Denmark), human epidermal growth factor receptor 2 (HER2; 1:8, clone 4B5, Ventana Medical Systems, Tucson, AZ, USA), AR (1:100, clone SP107, Cell Marque, Rocklin, CA, USA), pleomorphic adenoma gene 1 (PLAG1; 1:50, clone 3B7, Novus, Centennial, CO, USA), GCDFP-15 (1:50, clone 23A3, Neomarkers, Fremont, CA, USA), and anti-mitochondrial antibody (AM; 1:2,000, clone 113-1, Abcam, Cambridge, UK). Staining was carried out using the Benchmark XT automated immunohistochemistry system (Ventana Medical Systems). Expression in carcinoma cells and atypical cells was evaluated as follows: nuclear staining in ≥ 10% of cells was defined as positive for p53, AR, and PLAG1. The positivity of p53 was scored as +1 when 10% to one-third of cells were positive; +2 when one-third to one-half of cells were positive; or +3 when, more than two-thirds of cells were positive [14]. HER2 was evaluated using the American Society of Clinical Oncology 2018 system [15] as follows: negative, score 0 (no staining or incomplete staining in ≤ 10% of tumor cells) or score 1 (incomplete staining in > 10% of tumor cells); equivocal, score 2 (weak/moderate complete staining in > 10% of tumor cells); positive, score 3 (intense complete staining in > 10% of tumor cells). Cytoplasmic staining for GCDFP-15 and AM was graded from 0 to +3 according to the presence and intensity of the stain.
MATERIALS AND METHODS
- Patient characteristics
- CPA specimens came from eight male and three female patients aged 35 to 78 years (mean, 57). Eight cases were located in the parotid gland and three cases occurred in the submandibular gland. The mean tumor size was 2.6 cm (range, 1.5 to 4.3 cm). The mean time between symptom presentation and diagnosis was 123 months. Six patients received postoperative adjuvant radiotherapy. No patient developed recurrence or metastasis during the mean follow-up period of 66 months (range, 15 to 104 months). The 17 patients with PA included seven males and 10 females aged 29 to 73 years. The parotid gland was the most common site. These data are presented in Tables 1 and 2.
- Immunoprofiles
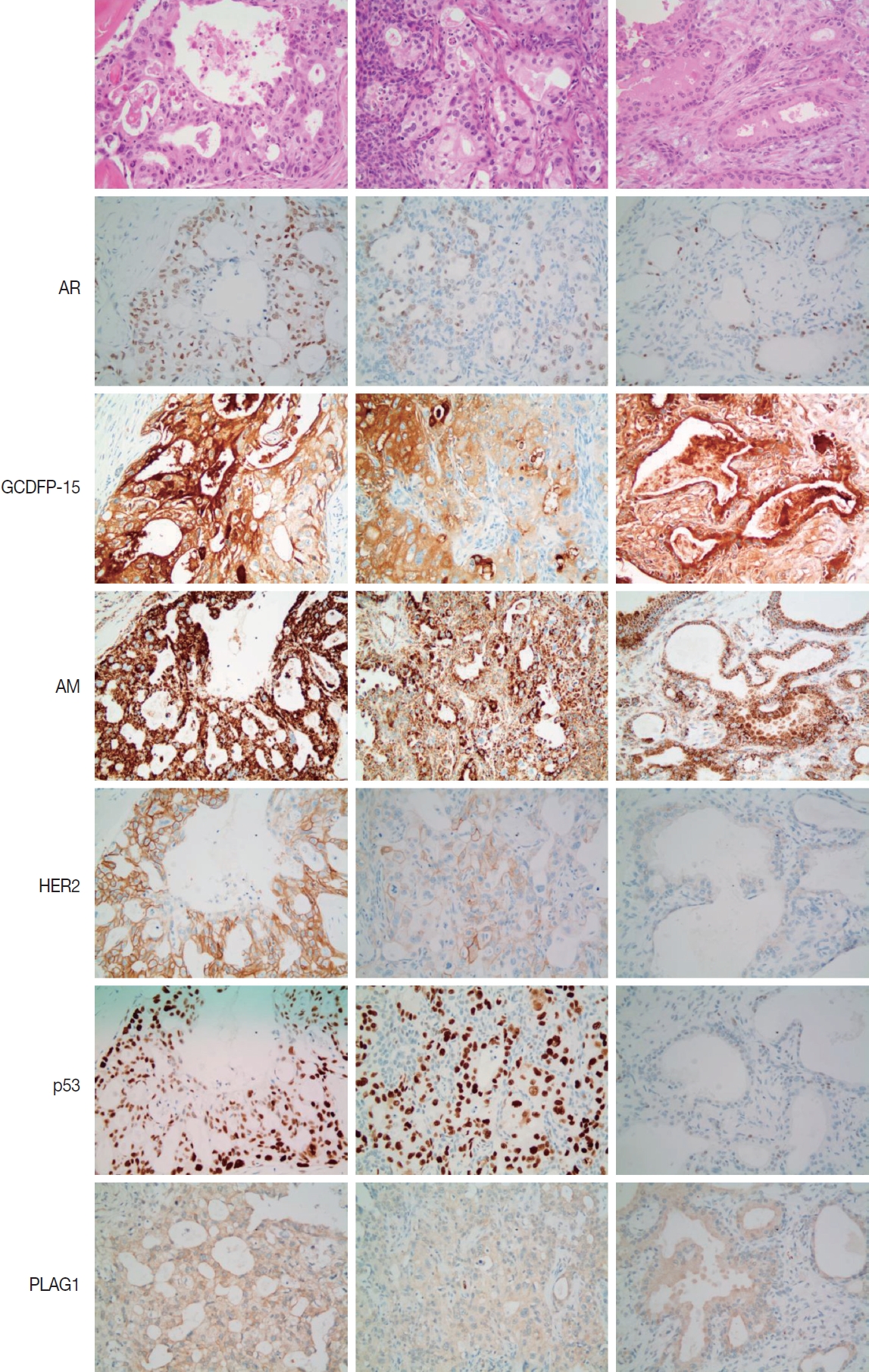
- The immunohistochemical results are summarized in Tables 1 and 2. Invasive or in situ carcinoma cells in all 11 CPAs were positive for AR and GCDFP-15, manifesting an apocrine nature. They were also positive for HER2, p53, and anti-mitochondrial antibody, and negative for PLAG1. The residual PA parts of CPA cases contained areas of apocrine phenotype and morphology including dense plump eosinophilic cytoplasm with snouts. HER2 expression was negligible in these components. The expression of p53 in the residual PAs was variable. Reaction to anti-mitochondrial antibody was strong in all cases, and PLAG1 was positive in one residual PA (Fig. 1).
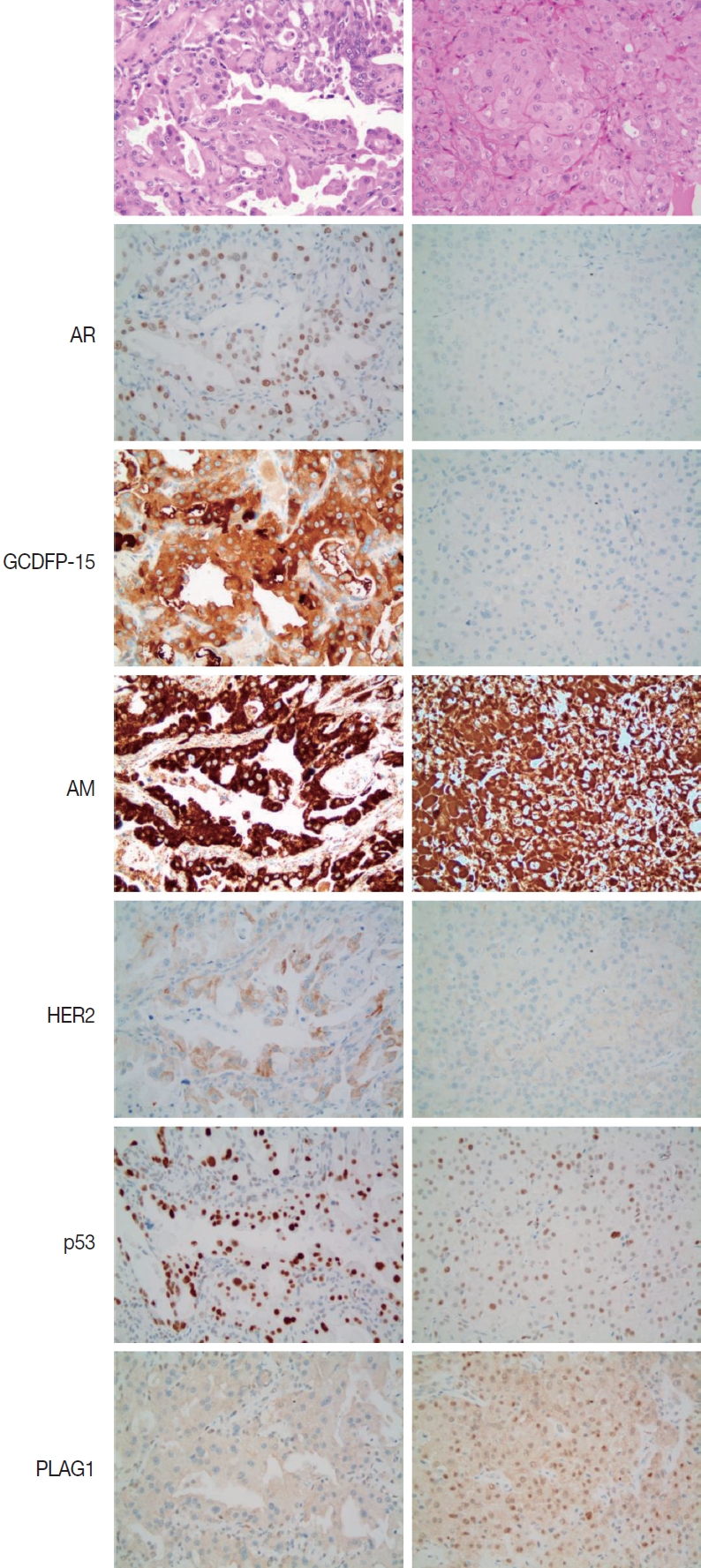
- Atypical cells in PA cases could be divided into either apocrine or oncocytic changes on the basis of reactivity to AR, GCDFP-15, and anti-mitochondrial antibody. Nine cases were positive for all, corresponding to apocrine changes, and eight cases were negative for AR or GCDFP-15 and strongly positive for anti-mitochondrial antibody, representing oncocytic changes. In the former group, the HER2 score was 1 or 0, while all cases in the latter group had a score of 0. All specimens with apocrine or oncocytic changes showed positive reactions to anti-mitochondrial antibody. There were variable positive reactions to p53 across the cases. In most specimens with oncocytic changes and in two apocrine cases, PLAG1 was expressed. These two types of metaplasia were sometimes difficult to distinguish by histology alone (Fig. 2). Interestingly, the acini of the submandibular glands stained diffusely positive for GCDFP-15, while the acini of the parotid gland did not, suggesting different constituents between the two glands.
RESULTS
- The most common type of CPA is high-grade carcinoma, which is histologically equivalent to SDC. Several genetic studies into PLAG1 or HMGA2 abnormalities in SDCs have suggested that a large proportion of SDCs arise in PAs regardless of the presence or absence of residual PA [2,16,17]. SDCs affect men more than women, and most of them show an apocrine phenotype with expression of AR [10]. We investigated whether there was an apocrine phenotype in the residual PA of CPAs and random PAs.
- Our study confirmed that carcinoma cells of luminal-type CPA or CisPA were apocrine in nature, and there were apocrine changes in the residual PA components of these cases. These results suggested that apocrine changes might precede the development of CPA, although the pre-neoplastic potential of apocrine changes cannot be determined at present. In the female breast, apocrine carcinoma is rare, while benign apocrine changes are common [18]. The neoplastic potential of apocrine changes in the breast remains controversial. Jones et al. [19] conducted comparative genomic hybridization on apocrine hyperplasia, apocrine carcinoma in situ, and invasive apocrine carcinoma, and suggested that apocrine hyperplasia is a non-obligate precursor of apocrine carcinoma. Other authors, however, have described the difficulty of distinguishing atypical apocrine lesions from low-grade apocrine carcinoma in situ, and the biological significance of atypical apocrine lesions in the breast is unclear [20].
- Apocrine changes or metaplasias are much rarer in the salivary gland than in the breast. Apocrine metaplasia in non-neoplastic salivary gland lesions has almost never been described. We found that the acini of the submandibular gland were diffusely positive for GCDFP-15, but they did not express AR. We found a similar report with respect to GCDFP-15 expression in the submandibular gland [21], and we hypothesize that there are differences in composition between the serous acini of the submandibular and parotid glands. Apocrine metaplasia is also a rare phenomenon in neoplasms of the salivary gland. Sclerosing polycystic adenosis (SPA), an uncommon proliferative lesion of the salivary gland, usually has an apocrine component, and 25.8% of these lesions develop ductal carcinoma, as reported in a review by Espinosa et al. [22] These authors described two new cases of intraductal epithelial proliferation with apocrine-like differentiation. For these reasons, many pathologists have considered SPA to be a tumorous lesion [23], and SPA is expected to be listed in the 5th edition of the WHO Classification of Head and Neck Tumors as ‘sclerosing polycystic adenoma’ [24]. A case of SPA with ductal carcinoma in situ and expression of GCDFP-15 and AR has also been reported, suggesting a pathogenesis similar to that of CPA [25].
- In PAs, apocrine metaplasia has rarely been described, while oncocytic, sebaceous, squamous, and mucinous metaplasia are relatively well recognized [26,27]. Nakajima et al. [12] reported that AR expression was observed in seven of 23 PA cases, but the relationship between AR expression and histology was not described. We could identify areas of apocrine changes in both residual PAs of CPAs and random PAs. The lesions often showed cystic changes and cytoplasmic snouts, but were sometimes histologically indistinguishable from oncocytic changes. Both changes are accompanied by cellular enlargement, rich eosinophilic cytoplasm, and large hyperchromatic nuclei with prominent nucleoli, with pathologists wavering between diagnoses of benign atypia and carcinoma in situ. Not only oncocytic but also apocrine-type cells stained strongly with anti-mitochondrial antibody, reflecting the abundance of intracytoplasmic mitochondria in both populations. The relevance of oncocytic changes in PA was not well established until Di Palma et al. [26] analyzed a case of PA with oncocytic changes using immunohistochemistry and microarray-based chromogenic in situ hybridization, and concluded that bizarre atypical cells are not malignant. They also decided, based on their expression of cytokeratin 8/18 and negativity for p63, that these cells were oncocytic epithelial cells. In contrast, non-apocrine oncocytic cells of the PAs in our series were all positive for PLAG1, suggesting that they had a myoepithelial nature.
- Many pathologists have sought to identify early malignant changes in PAs using immunohistochemistry (IHC), including p53, HER2, and AR [3,4,6]. DeRoche et al. [13] reported that three of 41 PAs exhibited multifocal staining for HER2 and AR, but that the stained ductal epithelium showed no cytological atypia. They concluded that these markers could not be used to reliably predict early carcinomatous transformation. The significance of these lesions remains unclear. Meanwhile, an HER2 positivity score of 3 correlated well with marked cellular and structural atypia in our series, and no cases of PA with apocrine or oncocytic atypia expressed HER2. This finding is consistent with those of previous studies by Di Palma et al. [4] and Logasundaram et al. [8]. It is noteworthy that all three of these studies, including ours, the HER2 expression rate in CPA was high, while the documented HER2 immunopositivity or amplification rate in de novo SDC is approximately 30% [28,29], suggesting pathogenetic differences. We recommend the use of HER2 IHC in atypical PAs, and that clinicians take HER2 positivity into serious consideration.
- We could not find any characteristic patterns of p53 overexpression in this series between PA and CPA, in contrast to a previous report on p53 positivity in focal carcinoma and atypical tumor cells in PA [3]. Other studies revealed that TP53 mutations were accompanied by malignant transformation of PA [5,30], but protein expression was ubiquitous in both PAs and CPAs in our study. Expression of p53 alone did not indicate carcinomatous transformation.
- In summary, we observed a similar apocrine phenotype in malignant and benign components of CPA, suggesting their relationship and a possible role of apocrine changes as a precursor to the development of carcinoma. Recognizing apocrine changes in PAs appears to be worth further investigation to facilitate the care of patients with PAs.
DISCUSSION
Ethics Statement
The study was approved by the institutional review board of Asan Medical Center (2021-1196), and the need for written informed consent was waived.
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Code Availability
Not applicable.
Author Contributions
Conceptualization: KJC. Data curation: KJC, JSS. Formal analysis: JSS, YK. Funding acquisition: KJC. Investigation: JSS. Methodology: KJC. Project administration: JSS. Resources: YSL, SHC, SYN, SYK. Supervision: KJC. Validation: KJC, JSS. Visualization: JSS. Writing—original draft: KJC, JSS. Writing— review & editing: KJC, JSS. Approval of final manuscript: all authors.
Conflicts of Interest
J.S.S., a contributing editor of the Journal of Pathology and Translational Medicine, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Funding Statement
No funding to declare.
AR, androgen receptor; GCDFP-15, gross cystic disease fluid protein-15; HER2, human epidermal growth factor receptor 2; AM, anti-mitochondrial antibody; PLAG1, pleomorphic adenoma gene 1; M, male; Inv. CPA, invasive carcinoma ex pleomorphic adenoma; CisPA, carcinoma in situ ex pleomorphic adenoma; PA, pleomorphic adenoma; F, female; SMG, submandibular gland.
- 1. Kim JW, Kwon GY, Roh JL, et al. Carcinoma ex pleomorphic adenoma of the salivary glands: distinct clinicopathologic features and immunoprofiles between subgroups according to cellular differentiation. J Korean Med Sci 2011; 26: 1277-85. ArticlePubMedPMCPDF
- 2. Bahrami A, Perez-Ordonez B, Dalton JD, Weinreb I. An analysis of PLAG1 and HMGA2 rearrangements in salivary duct carcinoma and examination of the role of precursor lesions. Histopathology 2013; 63: 250-62. ArticlePubMed
- 3. Ohtake S, Cheng J, Ida H, et al. Precancerous foci in pleomorphic adenoma of the salivary gland: recognition of focal carcinoma and atypical tumor cells by p53 immunohistochemistry. J Oral Pathol Med 2002; 31: 590-7. ArticlePubMedPDF
- 4. Di Palma S, Skalova A, Vanieek T, Simpson RH, Starek I, Leivo I. Non-invasive (intracapsular) carcinoma ex pleomorphic adenoma: recognition of focal carcinoma by HER-2/neu and MIB1 immunohistochemistry. Histopathology 2005; 46: 144-52. ArticlePubMed
- 5. Ihrler S, Weiler C, Hirschmann A, et al. Intraductal carcinoma is the precursor of carcinoma ex pleomorphic adenoma and is often associated with dysfunctional p53. Histopathology 2007; 51: 362-71. ArticlePubMed
- 6. Ihrler S, Guntinas-Lichius O, Agaimy A, Wolf A, Mollenhauer M. Histological, immunohistological and molecular characteristics of intraductal precursor of carcinoma ex pleomorphic adenoma support a multistep carcinogenic process. Virchows Arch 2017; 470: 601-9. ArticlePubMedPDF
- 7. Di Palma S. Carcinoma ex pleomorphic adenoma, with particular emphasis on early lesions. Head Neck Pathol 2013; 7 Suppl 1: S68-76. PubMed
- 8. Logasundaram R, Amarawickrama H, Premachandra D, Hellquist H. Intracapsular (in situ) carcinoma ex pleomorphic adenoma with unusual clinical and histological features. Eur Arch Otorhinolaryngol 2008; 265: 1563-6. ArticlePubMedPDF
- 9. Kapadia SB, Barnes L. Expression of androgen receptor, gross cystic disease fluid protein, and CD44 in salivary duct carcinoma. Mod Pathol 1998; 11: 1033-8. PubMed
- 10. Williams L, Thompson LD, Seethala RR, et al. Salivary duct carcinoma: the predominance of apocrine morphology, prevalence of histologic variants, and androgen receptor expression. Am J Surg Pathol 2015; 39: 705-13. PubMed
- 11. Nasser SM, Faquin WC, Dayal Y. Expression of androgen, estrogen, and progesterone receptors in salivary gland tumors: frequent expression of androgen receptor in a subset of malignant salivary gland tumors. Am J Clin Pathol 2003; 119: 801-6. ArticlePubMed
- 12. Nakajima Y, Kishimoto T, Nagai Y, et al. Expressions of androgen receptor and its co-regulators in carcinoma ex pleomorphic adenoma of salivary gland. Pathology 2009; 41: 634-9. ArticlePubMed
- 13. DeRoche TC, Hoschar AP, Hunt JL. Immunohistochemical evaluation of androgen receptor, HER-2/neu, and p53 in benign pleomorphic adenomas. Arch Pathol Lab Med 2008; 132: 1907-11. ArticlePubMedPDF
- 14. Schmitt FC, Soares R, Cirnes L, Seruca R. P53 in breast carcinomas: association between presence of mutation and immunohistochemical expression using a semiquantitative approach. Pathol Res Pract 1998; 194: 815-9. ArticlePubMed
- 15. Wolff AC, Hammond ME, Allison KH, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline focused update. Arch Pathol Lab Med 2018; 142: 1364-82. ArticlePubMedPDF
- 16. Chiosea SI, Thompson LD, Weinreb I, et al. Subsets of salivary duct carcinoma defined by morphologic evidence of pleomorphic adenoma, PLAG1 or HMGA2 rearrangements, and common genetic alterations. Cancer 2016; 122: 3136-44. ArticlePubMed
- 17. Katabi N, Ghossein R, Ho A, et al. Consistent PLAG1 and HMGA2 abnormalities distinguish carcinoma ex-pleomorphic adenoma from its de novo counterparts. Hum Pathol 2015; 46: 26-33. ArticlePubMed
- 18. D’Arcy C, Quinn CM. Apocrine lesions of the breast: part 2 of a two-part review. Invasive apocrine carcinoma, the molecular apocrine signature and utility of immunohistochemistry in the diagnosis of apocrine lesions of the breast. J Clin Pathol 2019; 72: 7-11. ArticlePubMed
- 19. Jones C, Damiani S, Wells D, Chaggar R, Lakhani SR, Eusebi V. Molecular cytogenetic comparison of apocrine hyperplasia and apocrine carcinoma of the breast. Am J Pathol 2001; 158: 207-14. ArticlePubMedPMC
- 20. D’Arcy C, Quinn C. Apocrine lesions of the breast: part 1 of a twopart review: benign, atypical and in situ apocrine proliferations of the breast. J Clin Pathol 2019; 72: 1-6. ArticlePubMed
- 21. Mazoujian G, Pinkus GS, Davis S, Haagensen DE Jr. Immunohistochemistry of a gross cystic disease fluid protein (GCDFP-15) of the breast: a marker of apocrine epithelium and breast carcinomas with apocrine features. Am J Pathol 1983; 110: 105-12. PubMedPMC
- 22. Espinosa CA, Rua L, Torres HE, Fernandez Del Valle A, Fernandes RP, Devicente JC. Sclerosing polycystic adenosis of the parotid gland: a systematic review and report of 2 new cases. J Oral Maxillofac Surg 2017; 75: 984-93. ArticlePubMed
- 23. Gnepp DR. Salivary gland tumor “wishes” to add to the next WHO Tumor Classification: sclerosing polycystic adenosis, mammary analogue secretory carcinoma, cribriform adenocarcinoma of the tongue and other sites, and mucinous variant of myoepithelioma. Head Neck Pathol 2014; 8: 42-9. ArticlePubMedPMCPDF
- 24. Skalova A, Hyrcza MD, Leivo I. Update from the 5th edition of the World Health Organization classification of head and neck tumors: salivary glands. Head Neck Pathol 2022; 16: 40-53. ArticlePubMedPMCPDF
- 25. Petersson F, Tan PH, Hwang JS. Sclerosing polycystic adenosis of the parotid gland: report of a bifocal, paucicystic variant with ductal carcinoma in situ and pronounced stromal distortion mimicking invasive carcinoma. Head Neck Pathol 2011; 5: 188-92. ArticlePubMedPMCPDF
- 26. Di Palma S, Lambros MB, Savage K, et al. Oncocytic change in pleomorphic adenoma: molecular evidence in support of an origin in neoplastic cells. J Clin Pathol 2007; 60: 492-9. ArticlePubMed
- 27. Triantafyllou A, Thompson LD, Devaney KO, et al. Functional histology of salivary gland pleomorphic adenoma: an appraisal. Head Neck Pathol 2015; 9: 387-404. ArticlePubMedPDF
- 28. Han MW, Roh JL, Choi SH, et al. Prognostic factors and outcome analysis of salivary duct carcinoma. Auris Nasus Larynx 2015; 42: 472-7. ArticlePubMed
- 29. Luk PP, Weston JD, Yu B, et al. Salivary duct carcinoma: clinicopathologic features, morphologic spectrum, and somatic mutations. Head Neck 2016; 38 Suppl 1: E1838-47. ArticlePubMedPDF
- 30. Valstar MH, Mast H, Ten Hove I, et al. Malignant transformation of salivary gland pleomorphic adenoma: proof of principle. J Pathol Clin Res 2021; 7: 432-7. ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
- Pleomorphic Adenoma with Epithelial Atypia, Apocrine Metaplasia, and/or In situ/Intracapsular Salivary Duct Carcinoma Are Indolent Lesions with Good Prognosis: A Proposal for Unified Nomenclature and Clinical Observation
Grayson G. Cole, Matt Levin, David Ferber, Spencer C. Roark, Peter M. Sadow, Daniel Lubin, Julie Guilmette, Jason R. Pettus, Adam S. Fisch, Dipti P. Sajed, Fouad R. Zakka, Mark W. Lingen, Nicole A. Cipriani
Head and Neck Pathology.2025;[Epub] CrossRef - Progression of Nasopharyngeal Pleomorphic Adenoma to Carcinoma Ex Pleomorphic Adenoma With Metastases: A Case Report
Krystsina Zhukovich, Alisher Tashbayev, Vladimir Osipov
Cureus.2025;[Epub] CrossRef - Carcinoma Ex Pleomorphic Adenoma of the Palate in a Young Female: A Rare and Aggressive Malignant Transformation
Sakshi Akolkar, Alka Hande, Archana Sonone, Husna Tehzeeb
Journal of Datta Meghe Institute of Medical Sciences University.2025; 20(4): 919. CrossRef - Characterization of a Molecularly Distinct Subset of Oncocytic Pleomorphic Adenomas/Myoepitheliomas Harboring Recurrent ZBTB47-AS1::PLAG1 Gene Fusion
Ziyad Alsugair, Jimmy Perrot, Françoise Descotes, Jonathan Lopez, Anne Champagnac, Daniel Pissaloux, Claire Castain, Mihaela Onea, Philippe Céruse, Pierre Philouze, Charles Lépine, Marie-Delphine Lanic, Marick Laé, Valérie Costes-Martineau, Nazim Benzerdj
American Journal of Surgical Pathology.2024; 48(5): 551. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
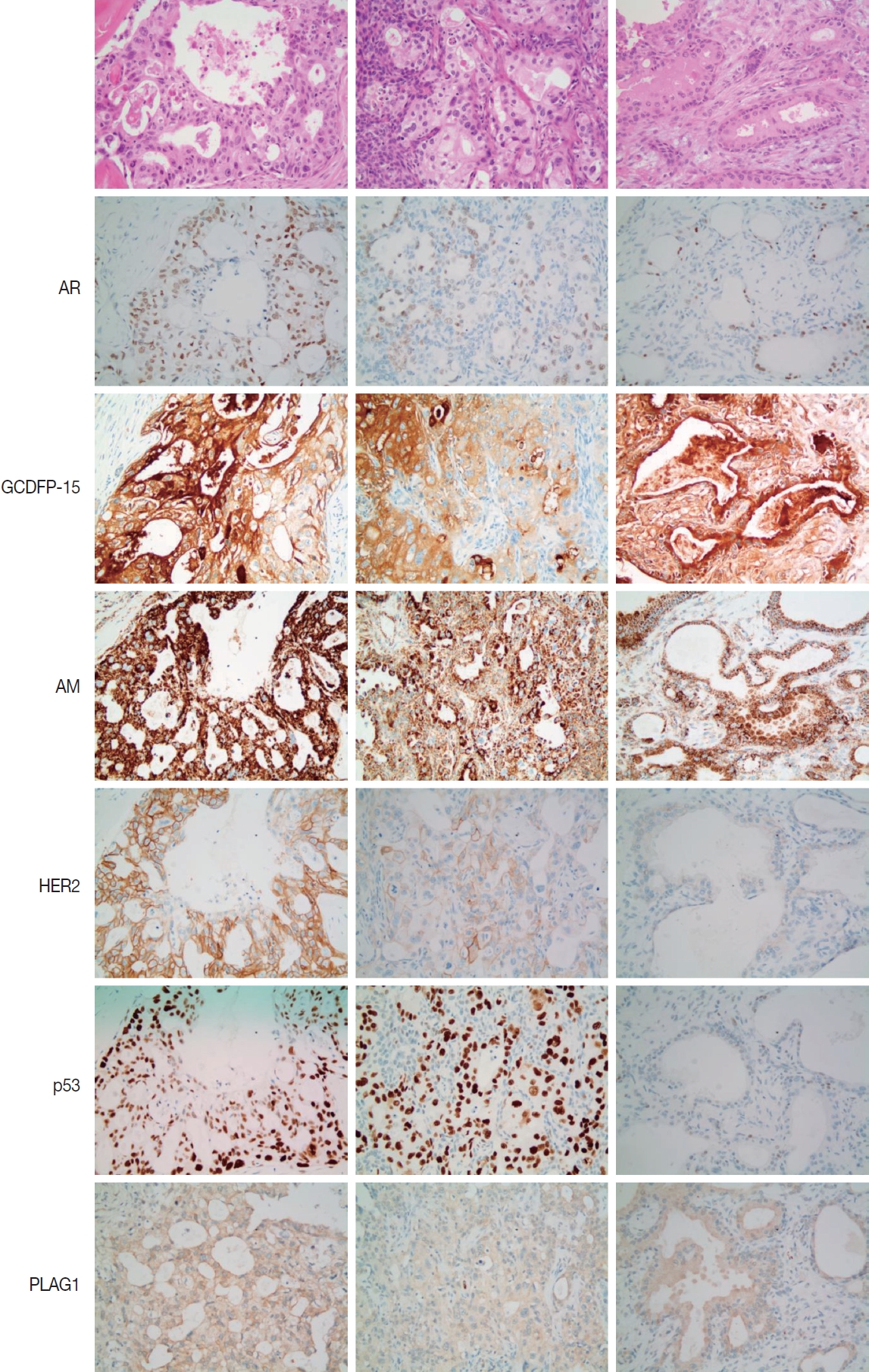
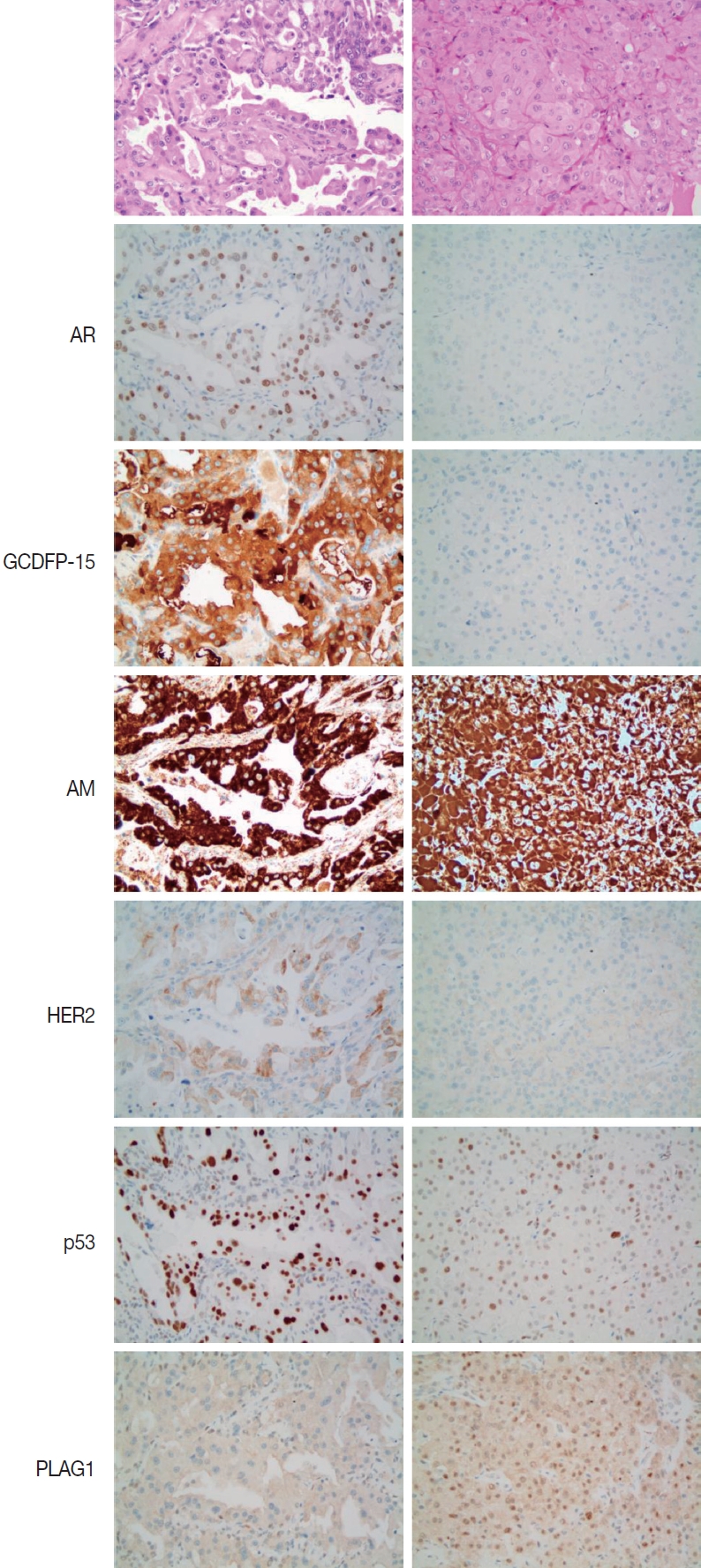


Fig. 1.
Fig. 2.
| Case No. | Location | Sex/Age (yr) | Component | AR | GCDFP-15 | HER2 | p53 | AM | PLAG1 |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Parotid | M/59 | Inv. CPA | + | +1 | 3 | +3 | +2 | – |
| CisPA | + | – | 2 | +3 | +1 | – | |||
| PA | + | +1 | 0 | +1 | +2 | – | |||
| 2 | Parotid | M/48 | Inv. CPA | + | – | 3 | +1 | +2 | – |
| CisPA | + | – | 3 | +1 | +2 | – | |||
| PA | + | +1 | 0 | - | +2 | – | |||
| 3 | Parotid | F/58 | Inv. CPA | + | – | 3 | +2 | +2 | – |
| CisPA | – | – | 1 | +2 | +2 | – | |||
| PA | + | + | 0 | +2 | +2 | + | |||
| 4 | Parotid | M/44 | Inv. CPA | + | +1 | 3 | +1 | +2 | – |
| CisPA | + | +1 | 3 | +1 | +2 | – | |||
| PA | + | +1 | 0 | +1 | +2 | – | |||
| 5 | Parotid | M/69 | Inv. CPA | + | +1 | 3 | +3 | +2 | – |
| CisPA | + | +1 | 3 | +3 | +2 | – | |||
| PA | + | +1 | 0 | +2 | +2 | – | |||
| 6 | Parotid | M/62 | CisPA | + | – | 3 | +1 | +2 | – |
| PA | + | +3 | - | +1 | +2 | – | |||
| 7 | SMG | F/78 | CisPA | + | +1 | 3 | +3 | +2 | – |
| PA | + | +1 | - | +1 | +2 | – | |||
| 8 | Parotid | M/35 | CisPA | + | +2 | 2 | +1 | +2 | – |
| PA | + | +3 | - | +1 | +2 | – | |||
| 9 | SMG | M/52 | CisPA | + | +1 | 2 | +3 | +3 | – |
| PA | + | +1 | - | +2 | +3 | – | |||
| 10 | SMG | F/52 | CisPA | + | +1 | 2 | +1 | +2 | – |
| PA | – | +2 | - | +1 | +2 | – | |||
| 11 | Parotid | M/55 | CisPA | + | +2 | 3 | +3 | +2 | – |
| PA | + | +2 | - | - | +1 | – |
| Case No. | Location | Sex/Age (yr) | AR | GCDFP-15 | HER2 | p53 | AM | PLAG1 |
|---|---|---|---|---|---|---|---|---|
| 1 | SMG | M/29 | + | +1 | 0 | +1 | +2 | – |
| 2 | Parotid | F/70 | + | +1 | 1 | +3 | +3 | + |
| 3 | Parotid | M/40 | + | +3 | 0 | +3 | +3 | – |
| 4 | Parotid | M/55 | + | +1 | 0 | +2 | +3 | – |
| 5 | Parotid | F/56 | + | +2 | 1 | +1 | +2 | – |
| 6 | Parotid | M/76 | + | +3 | 0 | +3 | +3 | – |
| 7 | Parotid | F/64 | + | +1 | 1 | +1 | +1 | + |
| 8 | SMG | M/62 | + | +1 | 1 | +1 | +1 | – |
| 9 | Oropharynx | M/70 | + | +3 | 1 | +1 | +3 | – |
| 10 | SMG | F/42 | – | – | 0 | +1 | +1 | + |
| 11 | Parotid | F/38 | – | – | 0 | +1 | +2 | + |
| 12 | SMG | F/61 | – | +1 | 0 | +1 | +2 | – |
| 13 | Parotid | M/37 | – | – | 0 | +1 | +2 | + |
| 14 | Parotid | F/73 | – | – | 0 | +2 | +1 | + |
| 15 | Buccal | F/36 | – | – | 0 | +1 | +3 | + |
| 16 | Parotid | F/64 | – | – | 0 | +2 | +3 | + |
| 17 | Parotid | F/55 | – | – | 0 | +2 | +3 | + |
AR, androgen receptor; GCDFP-15, gross cystic disease fluid protein-15; HER2, human epidermal growth factor receptor 2; AM, anti-mitochondrial antibody; PLAG1, pleomorphic adenoma gene 1; M, male; Inv. CPA, invasive carcinoma ex pleomorphic adenoma; CisPA, carcinoma in situ ex pleomorphic adenoma; PA, pleomorphic adenoma; F, female; SMG, submandibular gland.
AR, androgen receptor; GCDFP-15, gross cystic disease fluid protein-15; HER2, human epidermal growth factor receptor 2; AM, anti-mitochondrial antibody; PLAG1, pleomorphic adenoma gene 1; SMG, submandibular gland; M, male; F, female.

