 E-submission
E-submission
Search
- Page Path
- HOME > Search
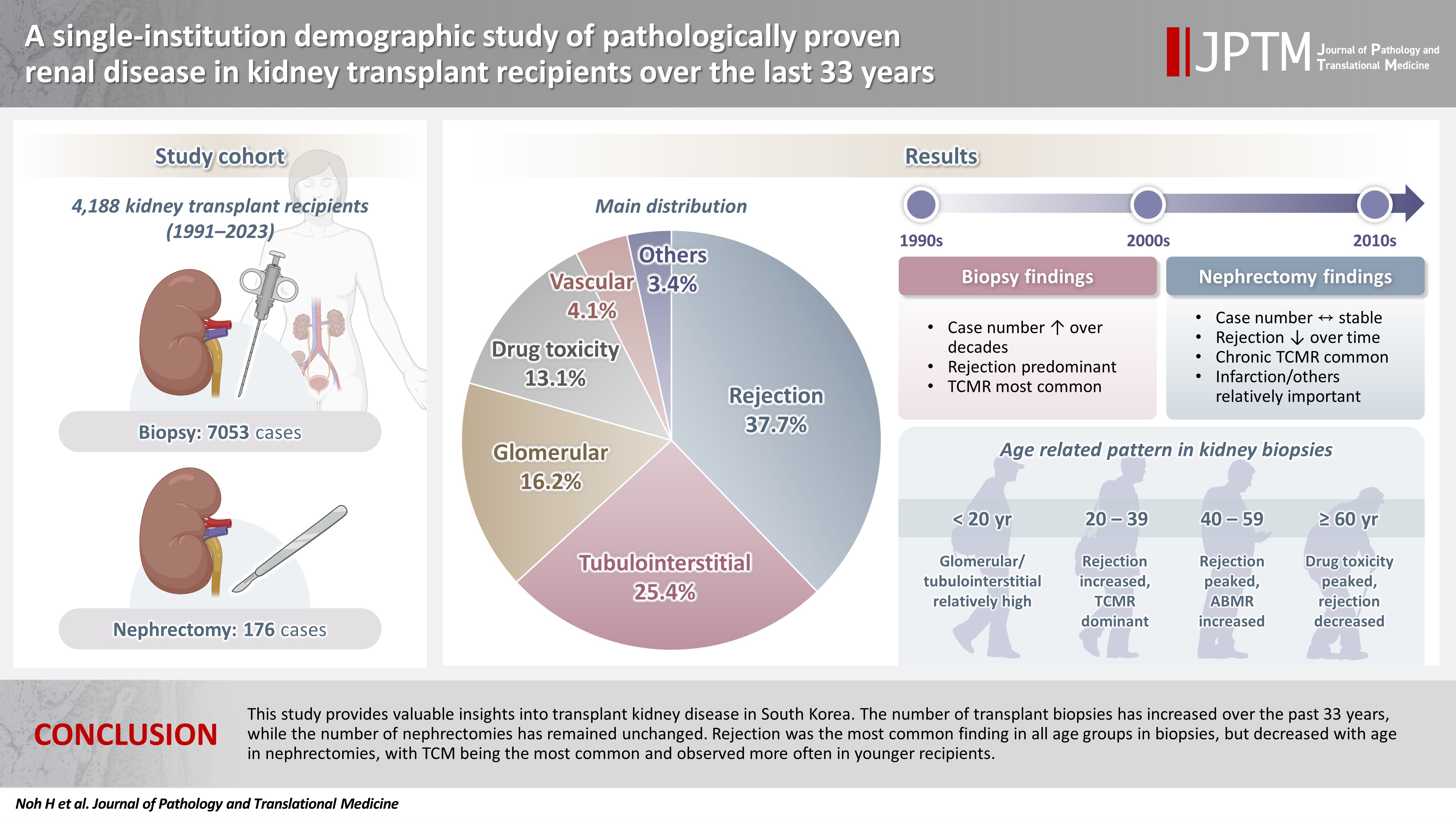
- A single-institution demographic study of pathologically proven renal disease in kidney transplant recipients over the last 33 years
- Hyejin Noh, Jiyeon Kim, Yeong Jin Choi
- J Pathol Transl Med. 2026;60(4):398-412. Published online May 26, 2026
- DOI: https://doi.org/10.4132/jptm.2026.03.28
- 1,218 View
- 20 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background
While the number of kidney transplants for end-stage renal disease (ESRD) is increasing, studies examining the long-term demographic analyses based on pathological diagnosis of transplant kidney remain limited. Methods: We conducted a retrospective analysis of 4,188 transplant recipients who underwent either biopsy or nephrectomy from 1991 to 2023 at Seoul St. Mary’s Hospital. Results: Among 7,229 pathologically confirmed cases, rejection was the most prevalent (37.7%), followed by tubulointerstitial (25.4%), glomerular, drug toxicity, and vascular diseases. In 7,053 transplant biopsies, rejection was predominant across all age groups, with T-cell mediated (TCM) category being the most common (60.1%), followed by antibody-mediated and mixed. Drug toxicity increased with age (p = .047), while glomerular and tubulointerstitial diseases were highest in recipients under 20 (p < .001). Among glomerular diseases, IgA-related glomerulonephritis (45.2%) was the most common. In 176 transplant nephrectomies, the most common diagnosis was rejection (33.5%), followed by renal infarction (19.9%), tubulointerstitial, vascular, glomerular disease, and drug toxicity. “Others” included infarction, ESRD, and lymphangiectasia, which increased with age (p = .011). In nephrectomy cases, rejection decreased over time, with chronic TCM rejection (40.7%) being the most frequent. Conclusions: This study provides valuable insights into transplant kidney disease in South Korea. The number of transplant biopsies has increased over the past 33 years, while the number of nephrectomies has remained unchanged. Rejection was the most common finding in all age groups in biopsies, but decreased with age in nephrectomies, with TCM being the most common and observed more often in younger recipients.
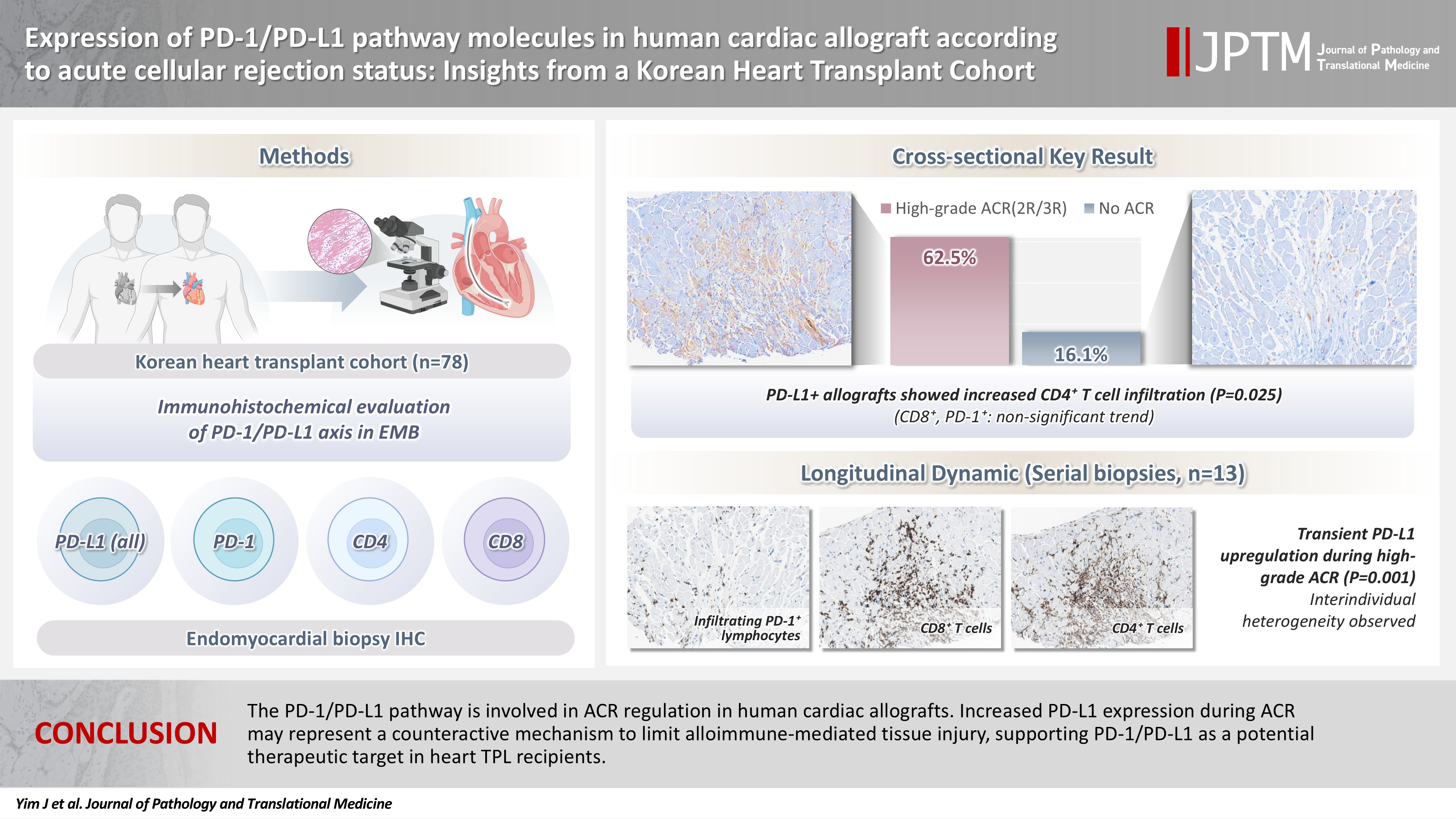
- Expression of PD-1/PD-L1 pathway molecules in human cardiac allograft according to acute cellular rejection status: insights from a Korean Heart Transplant Cohort
- Jeemin Yim, Yoon Kyung Jeon, Doo Hyun Chung, Jaemoon Koh
- J Pathol Transl Med. 2026;60(3):319-330. Published online March 27, 2026
- DOI: https://doi.org/10.4132/jptm.2026.01.02
- 2,353 View
- 78 Download
-
Abstract
PDF
- Background
Acute cellular rejection (ACR) following heart transplantation (TPL) compromises graft function and survival. The programmed cell death-1 (PD-1)/PD-1 ligand-1 (PD-L1) pathway represents an immune checkpoint that maintains peripheral immune tolerance, but its expression and significance in human cardiac allografts with ACR remain unclear. Thus, we investigated PD-1/ PD-L1 expression in endomyocardial biopsies from heart TPL recipients to clarify the role of this pathway in the ACR of human cardiac allografts and explore the potential of therapeutic modulation of PD-1/PD-L1 in this setting. Methods: Endomyocardial biopsies of 78 patients with heart TPL were subjected to immunohistochemistry for PD-L1, PD-1, CD4, and CD8. PD-L1 expression and quantities of PD-1+, CD4+, and CD8+ infiltrating lymphocytes were evaluated according to clinicopathological features, ACR presence, and clinical outcomes. Results: Allografts with high-grade ACR (International Society for Heart and Lung Transplantation grades 2R and 3R) demonstrated markedly higher PD-L1 expression than did those without ACR (62.5% vs. 16.1%, p < .001). PD-L1 expression was positively associated with CD4+ lymphocyte infiltration (p = .025), whereas CD8 and PD-1+ lymphocyte counts were higher in PD-L1-positive allografts without reaching statistical significance (p = .059 and p = .390, respectively). Serial biopsies revealed that PD-L1 expression was upregulated in patients with high-grade ACR compared with that in previous non-ACR tissues, and follow-up biopsies were performed after ACR resolution. Conclusions: The PD-1/PD-L1 pathway is involved in ACR regulation in human cardiac allografts. Increased PD-L1 expression during ACR may represent a counteractive mechanism to limit alloimmune-mediated tissue injury, supporting PD-1/PD-L1 as a potential therapeutic target in heart TPL recipients.
- Post-transplant liver biopsies: a concise and practical approach for beginners
- Mohamad Besher Ourfali, David Hirsch, Marianna Scranton, Tony El Jabbour
- J Pathol Transl Med. 2025;59(1):1-10. Published online January 15, 2025
- DOI: https://doi.org/10.4132/jptm.2024.11.15
- 7,432 View
- 449 Download
- 2 Web of Science
- 2 Crossref
-
Abstract
PDF
- Exposure to post-transplant liver biopsies varies among pathology residencies and largely depends on the institution's training program, particularly if the hospital has a liver transplant program. The interpretation of biopsies from transplanted livers presents its own set of challenges, even for those with a solid understanding of non-transplant medical liver biopsies. In this review, we aim to provide a succinct, step-by-step approach to help you interpret liver transplant biopsies. This article may be beneficial for residents interested in liver pathology, gastrointestinal and liver pathology fellows in the early stages of training, clinical gastroenterology and hepatology fellows, hepatologists and general pathologists who are curious about this niche.
-
Citations
Citations to this article as recorded by
- Primary biliary cholangitis: Beyond classical histopathology - diagnostic challenges in native and transplanted livers
Ivana Juskova, Andrea Vajsova, John Jackson, Ondrej Fabian, Eva Sticova
Annals of Diagnostic Pathology.2026; 85: 152683. CrossRef - Histological and Molecular Evaluation of Liver Biopsies: A Practical and Updated Review
Joon Hyuk Choi
International Journal of Molecular Sciences.2025; 26(16): 7729. CrossRef
- Primary biliary cholangitis: Beyond classical histopathology - diagnostic challenges in native and transplanted livers
- Quilty Lesions in the Endomyocardial Biopsies after Heart Transplantation
- Haeyon Cho, Jin-Oh Choi, Eun-Seok Jeon, Jung-Sun Kim
- J Pathol Transl Med. 2019;53(1):50-56. Published online December 26, 2018
- DOI: https://doi.org/10.4132/jptm.2018.11.30
- 9,537 View
- 132 Download
- 7 Web of Science
- 7 Crossref
-
Abstract
PDFSupplementary Material
- Background
The aim of this study was to investigate the clinical significance of Quilty lesions in endomyocardial biopsies (EMBs) of cardiac transplantation patients.
Methods
A total of 1190EMBs from 117 cardiac transplantation patients were evaluated histologically for Quilty lesions,acute cellular rejection, and antibody-mediated rejection. Cardiac allograft vasculopathy wasdiagnosed by computed tomography coronary angiography. Clinical information, including thepatients’ survival was retrieved by a review of medical records.
Results
Eighty-eight patients(75.2%) were diagnosed with Quilty lesions, which were significantly associated with acute cellularrejection, but not with acute cellular rejection ≥ 2R or antibody-mediated rejection. In patientsdiagnosed with both Quilty lesions and acute cellular rejection, the time-to-onset of Quilty lesionsfrom transplantation was longer than that of acute cellular rejections. We found a significant associationbetween Quilty lesions and cardiac allograft vasculopathy. No significant relationship wasfound between Quilty lesions and the patients’ survival.
Conclusions
Quilty lesion may be an indicator of previous acute cellular rejection rather than a predictor for future acute cellular rejection. -
Citations
Citations to this article as recorded by- A molecular reappraisal of quilty lesions: Insights from tissue and circulating biomarkers in heart transplantation
Andrea Fernandez Valledor, Cathrine M. Moeller, Adi Hertz, Daniel Oren, Ilan Richter, Boaz Elad, Julia Baranowska, Salwa Rahman, Carolyn Hennecken, Afsana Rahman, Dor Lotan, David Bae, Adil Yunis, Justin A. Fried, Ersilia M. DeFilippis, David T. Majure, J
The Journal of Heart and Lung Transplantation.2026; 45(5): 724. CrossRef - The roles of tertiary lymphoid structures in orchestrating immune responses in peripheral organs
Keisuke Taniguchi, Takahisa Yoshikawa, Motoko Yanagita
Inflammation and Regeneration.2025;[Epub] CrossRef - The human myocardium harbors a population of naive B-cells with a distinctive gene expression signature conserved across species
Kevin C. Bermea, Nicolas Kostelecky, Sylvie T. Rousseau, Chieh-Yu Lin, Luigi Adamo
Frontiers in Immunology.2022;[Epub] CrossRef - Examination of tracheal allografts after long-term survival in dogs
Tao Lu, Yiwei Huang, Yulei Qiao, Yongxing Zhang, Yu Liu
European Journal of Cardio-Thoracic Surgery.2021; 59(1): 155. CrossRef - Essentials in the diagnosis of postoperative myocardial lesions similar to or unrelated to rejection in heart transplant
Costel Dumitru, Ancuta Zazgyva, Adriana Habor, Ovidiu Cotoi, Horațiu Suciu, Carmen Cotrutz, Bogdan Grecu, Ileana Anca Sin
Revista Romana de Medicina de Laborator.2021; 29(3): 307. CrossRef - Clinical outcome of donor heart with prolonged cold ischemic time: A single‐center study
Fazal Shafiq, Yixuan Wang, Geng Li, Zongtao Liu, Fei Li, Ying Zhou, Li Xu, Xingjian Hu, Nianguo Dong
Journal of Cardiac Surgery.2020; 35(2): 397. CrossRef - The XVth Banff Conference on Allograft Pathology the Banff Workshop Heart Report: Improving the diagnostic yield from endomyocardial biopsies and Quilty effect revisited
Jean-Paul Duong Van Huyen, Marny Fedrigo, Gregory A. Fishbein, Ornella Leone, Desley Neil, Charles Marboe, Eliot Peyster, Jan von der Thüsen, Alexandre Loupy, Michael Mengel, Monica P. Revelo, Benjamin Adam, Patrick Bruneval, Annalisa Angelini, Dylan V. M
American Journal of Transplantation.2020; 20(12): 3308. CrossRef
- A molecular reappraisal of quilty lesions: Insights from tissue and circulating biomarkers in heart transplantation
- Prognosis of Hepatocellular Carcinoma after Liver Transplantation: Comparative Analysis with Partial Hepatectomy
- Kyuho Lee, Kyoung-Bun Lee, Nam-Joon Yi, Kyung-Suk Suh, Ja-June Jang
- J Pathol Transl Med. 2017;51(1):79-86. Published online December 25, 2016
- DOI: https://doi.org/10.4132/jptm.2016.10.13
- 10,372 View
- 152 Download
- 6 Web of Science
- 5 Crossref
-
Abstract
PDF
- Background
Liver transplantation (LT) is the treatment of choice for hepatocellular carcinoma (HCC). The aim of this study was to investigate the recurrence rate of HCC after LT and prognostic factors for recurrence by comparing LT with non-transplanted resection. Methods: The participants were 338 patients who underwent LT between 1996 and 2012 at Seoul National University Hospital (LT group) and 520 HCC patients who underwent partial hepatectomy between 1995 and 2006 (control group, non-LT group). Results: In the LT group, 68 of 338 patients (19.8%) showed relapse, and the recurrence rate was lower than that in the non-LT group (64.9%, 357/520, p < .001). Stratification analysis by American Joint Committee on Cancer (AJCC) stage showed that the stage I-II LT group had a lower recurrence rate than the non-LT group. Univariate comparative analysis demonstrated that multiplicity of tumor, tumor size, gross type, Edmondson- Steiner (ES) nuclear grade, extent of tumor, angioinvasion, AJCC stage, Milan criteria, University of California at San Francisco criteria on explant pathology (all p < .001), positive expression of cytokeratin 19 (p = .002), and preoperative α-fetoprotein (AFP) (p < .001) were predictors of tumor recurrence. In multivariate analysis, LT, preoperative AFP, multiplicity of tumor, extent of tumor, size of tumor, and ES nuclear grade were independent prognostic factors. Conclusions: LT might have a protective effect against the late recurrence of stage I-II HCC compared to non-LT, and the prognostic factors for recurrence were similar to previously well-known prognostic factors for HCC. -
Citations
Citations to this article as recorded by- Locoregional and Surgical Treatment of Single-Nodule Hepatocellular Carcinoma Recurrence After Liver Transplantation: A Systematic Review and a Meta-Analysis
Marco Maria Pascale, Camilla Marandola, Francesco Frongillo, Erida Nure, Salvatore Agnes
Cancers.2025; 17(9): 1501. CrossRef - Risk Factor Analysis of Death in Patients With Hepatic Cellular Carcinoma After Radical Operation: A Consecutive Cohort of 433 Patients
Zhengyang He, Wenfeng Lu, Dongze Qiu, Weimin She
Health Science Reports.2025;[Epub] CrossRef - Related Factors of Hepatocellular Carcinoma Recurrence Associated With Hyperglycemia After Liver Transplantation
Yujian Zheng, Qing Cai, Lishan Peng, Shibo Sun, Shaoping Wang, Jie Zhou
Transplantation Proceedings.2021; 53(1): 177. CrossRef - Oncological Outcomes of Hepatic Resection vs Transplantation for Localized Hepatocellular Carcinoma
A.T. Akcam, A.G. Saritas, A. Ulku, A. Rencuzogullari
Transplantation Proceedings.2019; 51(4): 1147. CrossRef - Clustering Asian Countries According to the Trend of liver cancer Mortality Rates: an Application of Growth Mixture Models
Maryam Salari, Anoshirvan Kazemnejad, Farid Zayeri
Iranian Red Crescent Medical Journal.2017;[Epub] CrossRef
- Locoregional and Surgical Treatment of Single-Nodule Hepatocellular Carcinoma Recurrence After Liver Transplantation: A Systematic Review and a Meta-Analysis
- Expression of CD99 in Multiple Myeloma: A Clinicopathologic and Immunohistochemical Study of 170 Cases
- Su-Jin Shin, Hyangsin Lee, Geunyoung Jung, Minchan Gil, Hosub Park, Young Soo Park, Dok Hyun Yoon, Cheolwon Suh, Chan-Jeoung Park, Jooryung Huh, Chan-Sik Park
- Korean J Pathol. 2014;48(3):209-216. Published online June 26, 2014
- DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.3.209
- 10,507 View
- 82 Download
- 9 Crossref
-
Abstract
PDF
Background Multiple myeloma (MM) is a heterogeneous and ultimately fatal disease. Risk stratification using prognostic biomarkers is crucial to individualize treatments. We sought to investigate the role of CD99, a transmembrane protein highly expressed in many hematopoietic cells including subpopulations of normal and neoplastic plasma cells, for MM risk stratification.
Methods CD99 expression was measured in paraffin samples of bone marrow and extramedullary biopsies of 170 patients with MM. Patients were divided into those with high score (moderately and strongly positive) and low score (negative and weakly positive), with all staining being cytoplasmic and/or membranous.
Results High anti-CD99 immunostaining was observed in 72 of 136 (52.9%) bone marrow biopsies and 24 of 87 (27.6%) extramedullary biopsies in MM. High CD99 expression of extramedullary specimens was associated with significantly longer overall survival (OS; p=.016). High CD99 expression of extramedullary specimens was also associated with better prognosis in the nonautologous stem cell transplantation group of MM patients (p=.044). In multivariate analysis, International Staging System stage was an independent prognostic factor, whereas CD99 expression was no longer statistically significant.
Conclusions Expression of CD99 in extramedullary specimens was correlated with longer OS, suggesting that CD99 may be a helpful immunohistochemical marker for risk stratification.
-
Citations
Citations to this article as recorded by- Cell Adhesion Molecule CD99 in Cancer Immunotherapy
Feng Yu, Guodong Liu, Hailing Zhang, Xiaoyan Wang, Zhi Wu, Qinggang Xu, Yan Wu, Dongfeng Chen
Current Molecular Medicine.2023; 23(10): 1028. CrossRef - Detection of Circulating Tumor Plasma Cells in Monoclonal Gammopathies: Methods, Pathogenic Role, and Clinical Implications
Luzalba Sanoja-Flores, Juan Flores-Montero, Martín Pérez-Andrés, Noemí Puig, Alberto Orfao
Cancers.2020; 12(6): 1499. CrossRef - Tumor suppressor CD99 is downregulated in plasma cell neoplasms lacking CCND1 translocation and distinguishes neoplastic from normal plasma cells and B-cell lymphomas with plasmacytic differentiation from primary plasma cell neoplasms
Qi Gao, Venkata Yellapantula, Maly Fenelus, Janine Pichardo, Lu Wang, Ola Landgren, Ahmet Dogan, Mikhail Roshal
Modern Pathology.2018; 31(6): 881. CrossRef - EWSR1 fusion proteins mediate PAX7 expression in Ewing sarcoma
Gregory W Charville, Wei-Lien Wang, Davis R Ingram, Angshumoy Roy, Dafydd Thomas, Rajiv M Patel, Jason L Hornick, Matt van de Rijn, Alexander J Lazar
Modern Pathology.2017; 30(9): 1312. CrossRef - Activation of the polycomb repressive complex pathway in the bone marrow resident cells of diffuse large B-cell lymphoma patients
Eun Ji Oh, Eun Kyung Kim, Woo Ick Yang, Sun Och Yoon
Leukemia & Lymphoma.2016; 57(8): 1921. CrossRef - CD99 Is Strongly Expressed in Basal Cells of the Normal Adult Epidermis and Some Subpopulations of Appendages: Comparison with Developing Fetal Skin
Gawon Choi, Jin Roh, Chan-Sik Park
Journal of Pathology and Translational Medicine.2016; 50(5): 361. CrossRef - Towards Stratified Medicine in Plasma Cell Myeloma
Philip Egan, Stephen Drain, Caroline Conway, Anthony Bjourson, H. Alexander
International Journal of Molecular Sciences.2016; 17(10): 1760. CrossRef - Human Myeloma Cell Lines Induce Osteoblast Downregulation of CD99 Which Is Involved in Osteoblast Formation and Activity
Angela Oranger, Giacomina Brunetti, Claudia Carbone, Graziana Colaianni, Teresa Mongelli, Isabella Gigante, Roberto Tamma, Giorgio Mori, Adriana Di Benedetto, Marika Sciandra, Selena Ventura, Katia Scotlandi, Silvia Colucci, Maria Grano
Journal of Immunology Research.2015; 2015: 1. CrossRef - CD99 regulates CXCL12-induced chemotaxis of human plasma cells
Minchan Gil, Hyo-Kyung Pak, A-Neum Lee, Seo-Jung Park, Yoonkyung Lee, Jin Roh, Hyunji Lee, Yoo-Sam Chung, Chan-Sik Park
Immunology Letters.2015; 168(2): 329. CrossRef
- Cell Adhesion Molecule CD99 in Cancer Immunotherapy
- Silent Colonic Malakoplakia in a Living-Donor Kidney Transplant Recipient Diagnosed during Annual Medical Examination
- Go Eun Bae, Nara Yoon, Ha Young Park, Sang Yun Ha, Junhun Cho, Yunkyung Lee, Kyoung-Mee Kim, Cheol Keun Park
- Korean J Pathol. 2013;47(2):163-166. Published online April 24, 2013
- DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.2.163
- 9,373 View
- 62 Download
- 10 Crossref
-
Abstract
PDF
Malakoplakia is a characteristic inflammatory condition, which is usually seen in the urogenital tract, and less frequently in the gastrointestinal tract. We present a case of colonic malakoplakia in an immunocompromised patient. A 55-year-old female visited the outpatient clinic for routine cancer surveillance. Her past medical history was significant for kidney transplantation 11 years ago, and she had been taking immunosuppressants. A colonoscopy revealed several depressed flat lesions and elevated polyps, which were 0.3 to 0.4 cm in size and accompanied by whitish exudates. A biopsy revealed an infiltration of histiocytes with ample granular eosinophilic cytoplasm, with some lymphocytes and plasma cells. Many histiocytes had the characteristic morphology, described as Michaelis-Gutmann bodies: one or several round basophilic structures of approximately 1 to 10 µm in size with some being laminated, some appearing homogeneous, and others having a dense central core with a targetoid appearance. These Michaelis-Gutmann bodies were positively stained on von Kossa stain, and were diagnostic for malakoplakia.
-
Citations
Citations to this article as recorded by- Malakoplakia in kidney transplant recipients: Three case reports
Prathap Kumar Simhadri, Renish Contractor, Deepak Chandramohan, Matthew McGee, Udit Nangia, Mohammad Atari, Syed Bushra, Sanjana Kapoor, Ramya Krishna Velagapudi, Pradeep K Vaitla
World Journal of Nephrology.2025;[Epub] CrossRef - Caecal malakoplakia: a rare mimic of malignancy
Jeffrey Li Voon Chong, Noor Ali
BMJ Case Reports.2024; 17(1): e257130. CrossRef - Malakoplakia Associated with Colonic Adenocarcinoma: Case Report and Literature Review of a Rare Occurrence
Sarah Tolaymat, Faryal Afridi, MD, Emily Groves, MD
West Virginia Medical Journal.2024; 120(4): 18. CrossRef - A Surgical Challenge Generated by Colonic Malakoplakia in Disguise as a Locally Advanced Colonic Malignancy—A Case Report
Cristina Șerban, Alexandra Toma, Dragoș Cristian Voicu, Constantin Popazu, Dorel Firescu, George Țocu, Raul Mihailov, Laura Rebegea
Medicina.2023; 59(1): 156. CrossRef - Colonic malakoplakia in a cardiac transplant recipient: A case report
Sadiya Shafijan
Indian Journal of Pathology and Microbiology.2020; 63(2): 322. CrossRef - Immunosuppressive drugs and the gastrointestinal tract in renal transplant patients
Merel M. Tielemans, Gerben A.J. van Boekel, Teun van Gelder, Eric T. Tjwa, Luuk B. Hilbrands
Transplantation Reviews.2019; 33(2): 55. CrossRef - Malakoplakia of the colon following renal transplantation in a 73 year old woman: report of a case presenting as intestinal perforation
Andrew Mitchell, Alexandre Dugas
Diagnostic Pathology.2019;[Epub] CrossRef - Colonic malakoplakia in a liver transplant recipient: A case report
Rana Ajabnoor, Mohammad Mawardi, Abdulmonem Almutawa
Human Pathology: Case Reports.2019; 18: 200323. CrossRef - Malakoplakia after kidney transplantation: Case report and literature review
John Fredy Nieto‐Ríos, Isabel Ramírez, Mónica Zuluaga‐Quintero, Lina María Serna‐Higuita, Federico Gaviria‐Gil, Alejandro Velez‐Hoyos
Transplant Infectious Disease.2017;[Epub] CrossRef - Megalocytic Interstitial Nephritis Following Acute Pyelonephritis with Escherichia coli Bacteremia: A Case Report
Hee Jin Kwon, Kwai Han Yoo, In Young Kim, Seulkee Lee, Hye Ryoun Jang, Ghee Young Kwon
Journal of Korean Medical Science.2015; 30(1): 110. CrossRef
- Malakoplakia in kidney transplant recipients: Three case reports
- Histopathological Causes of Late Liver Allograft Dysfunction: Analysis at a Single Institution
- Eun Shin, Ji Hoon Kim, Eunsil Yu
- Korean J Pathol. 2013;47(1):21-27. Published online February 25, 2013
- DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.1.21
- 10,491 View
- 73 Download
- 5 Crossref
-
Abstract
PDF
Background We summarize our experience in the pathological diagnosis of late complications of liver transplantation (LT) to better understand the causes of late allograft dysfunction in a population mostly composed of patients with hepatitis B virus (HBV) infection.
Methods We reviewed 361 post-transplant liver biopsies from 174 patients who underwent LT and first presented with liver function abnormalities 3 months post-procedure. The underlying diseases included HBV-associated liver disease (77%), toxic or alcoholic liver disease (10.3%), hepatitis C virus (HCV)-associated liver disease (8.6%), primary biliary cirrhosis (1.2%), primary sclerosing cholangitis (1.2%), and metabolic disease (1.7%).
Results The three most common late complications were acute rejection (32.5%), recurrent disease (19.1%), and biliary complication (17.1%). Patients who underwent LT for HBV infection or for drug- or alcohol-related liver disease had a lower incidence of recurring disease than those who underwent transplantation for HCV infection. During post-transplantation months 3-12, acute rejection was the most common cause of allograft dysfunction and recurring disease was the leading cause for allograft dysfunction (p=0.039). The two primary causes of late allograft dysfunction have overlapping histological features, although acute rejection more frequently showed bile duct damage and vascular endothelialitis than recurring HBV infection, and recurring HBV infection had more frequent lobular activity and piecemeal necrosis.
Conclusions The causes of late liver allograft dysfunction are closely associated with the original liver diseases and the period after LT. Careful attention is required for differential diagnosis between acute rejection and recurrent HBV.
-
Citations
Citations to this article as recorded by- Renal Allograft Pathology Classifications: Contemporary Updates and Diagnostic Utility
Hussein Qasim, Hamza Abuuqteish, Karis Khattab, Matteo Luigi Giuseppe Leoni , Giustino Varrassi
Cureus.2025;[Epub] CrossRef - Liver Transplantation from a Human Leukocyte Antigen-Matched Sibling Donor: Effectiveness of Direct-Acting Antiviral Therapy against Hepatitis C Virus Infection
Tatsuo Kanda, Naoki Matsumoto, Tomotaka Ishii, Shuhei Arima, Shinji Shibuya, Masayuki Honda, Reina Sasaki-Tanaka, Ryota Masuzaki, Shini Kanezawa, Masahiro Ogawa, Shintaro Yamazaki, Osamu Aramaki, Hirofumi Kogure, Yukiyasu Okamura
Reports.2022; 5(4): 49. CrossRef - A comparative histological analysis of early and late graft dysfunction in different time zones following living donor liver transplantation
Archana Rastogi, Nayana Patil, Sphurti Srivastava, Gayatri Ramakrishna, Rakhi Maiwal, Guresh Kumar, Ashok K. Choudhary, Seema Alam, Chhagan Bihari, Viniyendra Pamecha
Indian Journal of Pathology and Microbiology.2022; 65(4): 802. CrossRef - Differences in risk factors for early-onset and late-onset biliary complications in liver transplant patients
Hsiu-Lung Fan, An-Chieh Feng, Meng-Hsing Ho, Shih-Ming Kuo, Wei-Chou Chang, Teng-Wei Chen
Journal of Medical Sciences.2015; 35(5): 201. CrossRef - Vitamin C exerts beneficial hepatoprotection against Concanavalin A-induced immunological hepatic injury in mice through inhibition of NF-κB signal pathway
Tao Liang, Xiaoyu Chen, Min Su, Hongqiu Chen, Guozhe Lu, Kun Liang
Food & Function.2014; 5(9): 2175. CrossRef
- Renal Allograft Pathology Classifications: Contemporary Updates and Diagnostic Utility
- Clinicopathologic Analysis of the Liver Explant with Severe Hepatitis A Virus Infection.
- Joo Young Kim, Sung Gyu Lee, Shin Hwang, Ji Hoon Kim, Se Jin Jang, Eunsil Yu
- Korean J Pathol. 2011;45:S48-S52.
- DOI: https://doi.org/10.4132/KoreanJPathol.2011.45.S1.S48
- 3,950 View
- 25 Download
-
Abstract
PDF
- The incidence of severe hepatitis A virus (HAV) infection has been increasing. However, clinicopathologic features of severe HAV infection that lead to liver transplantation (LT) have not been reported in Korea. We retrieved 16 LT cases with HAV infection during the last 3 years at Asan Medical Center, Seoul, Korea. Fifteen cases progressed to hepatic encephalopathy. Thirteen cases survived with or without complications, and three patients died of sepsis. The explanted liver showed massive or zonal necrosis with moderate to severe cholestasis. The zonal distribution of necrosis was frequently associated with endothelialitis of portal and/or central veins. Degenerative changes of hepatocytes were various in degree and distribution. Viral inclusions were suspected in two cases. Although HAV infection is usually confirmed by serological tests, significant venulitis of central and/or portal veins and viral inclusions, which are rarely observed, can suggest an HAV infection as a cause of massive hepatic necrosis of unknown mechanism.
- Newly Formed Hepatic Masses in Children with Biliary Atresia after Kasai Hepatic Portoenterostomy.
- Hye Jong Song, Yeon Lim Suh
- Korean J Pathol. 2011;45(2):160-169.
- DOI: https://doi.org/10.4132/KoreanJPathol.2011.45.2.160
- 5,352 View
- 31 Download
- 3 Crossref
-
Abstract
PDF
- BACKGROUND
This report describes the clinicopathologic findings of six hepatic masses that developed after Kasai hepatic portoenterostomy (HPE) in six patients with longstanding biliary atresia (BA).
METHODS
Hepatic masses were found in six of 55 pediatric patients who underwent liver transplantation for BA after Kasai HPE from 1997 to 2009. Clinicopathologic analysis was performed and immunohistochemical staining was carried out for CD34, smooth muscle actin (SMA) and cytokeratin 7.
RESULTS
Of the six hepatic masses, two were diagnosed as focal nodular hyperplasia (FNH)-like lesions, two were large regenerative nodules (LRN), one was a mesenchymal hamartoma (MH) and one was a cholangiocarcinoma. The immunohistochemical staining findings for SMA and CD34 were more prominent for the FNH-like nodules than for the cirrhotic background liver. Dysplastic biliary epithelium arising from intestinal metaplasia was found in the cholangiocarcinoma.
CONCLUSIONS
Our findings suggest that FNH-like lesions, LRNs and MH are the results of vascular hemodynamic changes after Kasai HPE and that cholangiocarcinoma is due to recurrent cholangitis after BA. All the lesions in this series must be included in the differential diagnosis of a newly formed hepatic mass in patients after portoenterostomy. -
Citations
Citations to this article as recorded by- Imaging Findings and Management Strategies for Liver Masses in Children with Predisposition Disorders: A Review by the Pediatric LI-RADS Group
Amy B. Kolbe, Michael R. Acord, Geetika Khanna, Cara E. Morin, HaiThuy N. Nguyen, Mitchell A. Rees, Esther Ro, Gary R. Schooler, Judy H. Squires, Ali B. Syed, Elizabeth R. Tang, Alexander J. Towbin, Adina Alazraki
RadioGraphics.2025;[Epub] CrossRef - Features of Nodules in Explants of Children Undergoing Liver Transplantation for Biliary Atresia
Ana M. Calinescu, Anne-Laure Rougemont, Mehrak Anooshiravani, Nathalie M. Rock, Valerie A. McLin, Barbara E. Wildhaber
Journal of Clinical Medicine.2022; 11(6): 1578. CrossRef - Biliary Atresia Patients With Successful Kasai Portoenterostomy Can Present With Features of Obliterative Portal Venopathy
Kalyani R. Patel, Sanjiv Harpavat, Zahida Khan, Sadhna Dhingra, Norma Quintanilla, Mihail Firan, John Goss
Journal of Pediatric Gastroenterology and Nutrition.2020; 71(1): 91. CrossRef
- Imaging Findings and Management Strategies for Liver Masses in Children with Predisposition Disorders: A Review by the Pediatric LI-RADS Group
- Comparison of Detecting Methods of BK Virus Infection in Patients with Renal Allograft Recipients.
- Sung Hak Lee, Youn Jun Park, Chul Woo Yang, Yong Soo Kim, In Sung Moon, Chang Suk Kang, Yeong Jin Choi
- Korean J Pathol. 2010;44(6):636-641.
- DOI: https://doi.org/10.4132/KoreanJPathol.2010.44.6.636
- 4,889 View
- 26 Download
- 2 Crossref
-
Abstract
PDF
- BACKGROUND
BK virus nephropathy (BKVN) is an emerging problem as a consequence of the use of potent immunosuppressive agents. Because optimal detection methods for the diagnosis of BKVN are required clinically, we compared the results of renal allograft biopsy, urine cytology, and urine and blood viral loads.
METHODS
Four hundred sixty two case notes from 2004 to 2009 at Seoul St. Mary's Hospital were reviewed. During that period, 286 cases of urine cytology for decoy cells, 938 cases of urine BKV reverse transcription-polymerase chain reaction (RT-PCR), and 1,029 cases of blood BKV RT-PCR were performed. All diagnostic methods were performed in 85 cases.
RESULTS
A histological diagnosis of BKVN was made in 2.4% of cases (11/462). Urine cytology for decoy cells was positive in 26.2% (75/286). BKV RT-PCR revealed viruria in positivity of 22.1% (207/938) and viremia in 5.2% (54/1,029). In cases of BKVN, the sensitivities of urine and blood BKV RT-PCR were all 100% and the specificities were 69% and 94.5%, respectively. In cases with positive urine decoy cells, the sensitivities of urine and blood BKV RT-PCR were 50% and 27.7%, with specificities of 77.7% and 100%, respectively.
CONCLUSIONS
BKV screening by RT-PCR assays may be a clinically useful noninvasive test to identify renal recipients with concurrent BKVN. -
Citations
Citations to this article as recorded by- Prevalence of BK Virus among Iranian Renal Transplant Recipients: A Systematic Review and Meta-Analysis
Mohsen Ebrahimi, Alireza Mohebbi, Mohammad Mostakhdem Hashemi, Mobina Ashrafi Shahmirzadi
Journal of Clinical and Basic Research.2020; 4(4): 50. CrossRef - Asymptomatic hematuria associated with urinary polyomavirus infection in immunocompetent patients
Sung Hak Lee, Sung Hoo Hong, Ji Youl Lee, Tae Kon Hwang, Kyoung Suk Kim, Hyoungnam Lee, Yeong Jin Choi
Journal of Medical Virology.2014; 86(2): 347. CrossRef
- Prevalence of BK Virus among Iranian Renal Transplant Recipients: A Systematic Review and Meta-Analysis
- Characterization of Histopathological Features that Differentiate Hepatitis B Virus Infection from Acute Cellular Rejection.
- Dong Eun Song, Dong Hwan Jung, Shin Hwang, Bong Hee Park, Eunsil Yu
- Korean J Pathol. 2009;43(6):535-541.
- DOI: https://doi.org/10.4132/KoreanJPathol.2009.43.6.535
- 4,966 View
- 19 Download
- 3 Crossref
-
Abstract
PDF
- BACKGROUND
Differentiation of viral hepatitis from acute cellular rejection (ACR) after liver transplantation can be difficult because of overlapping histological features. Here we investigated clinicopathologic characteristics of 311 liver allograft biopsies and searched for characteristic histopathological features that would facilitate the differential diagnosis between hepatitis B virus (HBV) infection and ACR. METHODS: A retrospective clinicopathologic examination of 311 liver allograft biopsies consisting of clinically proven ACR or HBV infection was performed. Immunohistochemical staining for HBcAg and HBsAg was done for 64 allograft biopsies showing HBV infection. RESULTS: Moderate to severe bile duct damage, diffuse centrilobular necrosis and centrilobular inflammation (p<0.000, for each) were more frequently observed in cases of ACR, whereas diffuse acidophilic bodies and spotty necrosis (p<0.000, for each) were more prevalent in cases of HBV infection. Immunopositivity for HBcAg (n=60, 93.8%) was higher than that for HBsAg (n=14, 21.9%) CONCLUSIONS: The presence of moderate to severe bile duct damage, diffuse centrilobular necrosis and centrilobular inflammation was a characteristic feature of ACR, whereas diffuse distribution of acidophilic bodies or spotty necrosis was the only characteristic feature of HBV infection. HBcAg was a more sensitive immunohistochemical marker than HBsAg for detecting HBV infection in liver allograft biopsies. -
Citations
Citations to this article as recorded by- Analysis of S Gene Mutation of the Hepatitis B Virus in Adult Liver Transplant Recipients Showing Resistance to Hepatitis B Immunoglobulin Therapy
G.-C. Park, S. Hwang, C.-S. Ahn, K.-H. Kim, D.-B. Moon, T.-Y. Ha, G.-W. Song, D.-H. Jung, Y.W. Shin, S.-H. Kim, K.-H. Chang, J.-M. Namgoong, C.-S. Park, H.-W. Park, Y.-H. Park, S.-H. Kang, B.-H. Jung, S.-G. Lee
Transplantation Proceedings.2013; 45(8): 3047. CrossRef - Posttransplantation prophylaxis with primary high-dose hepatitis B immunoglobulin monotherapy and complementary preemptive antiviral add-on a
Shin Hwang, Chul-Soo Ahn, Gi-Won Song, Ki-Hun Kim, Deok-Bog Moon, Heung-Bum Oh, Young-Suk Lim, Han Chu Lee, Tae-Yong Ha, Dong-Hwan Jung, Young-Hwa Chung, Sung-Gyu Lee
Liver Transplantation.2011; 17(4): 456. CrossRef - Posttransplantation Prophylaxis with Primary High-dose Hepatitis B Immunoglobulin Monotherapy and Complementary Preemptive Antiviral Add-on. Liver Transpl 2011;17:456-465
Dong-Hwan Jung, Shin Hwang
The Korean Journal of Gastroenterology.2011; 57(5): 330. CrossRef
- Analysis of S Gene Mutation of the Hepatitis B Virus in Adult Liver Transplant Recipients Showing Resistance to Hepatitis B Immunoglobulin Therapy
- Graft-Versus-Host Disease of the Lung after Allogeneic Hematopoietic Stem Cell Transplantation: A Report of Two Cases.
- Ji Hyeon Roh, Joungho Han, Keon Hee Yoo, Kang Mo Ahn, Jihye Kim
- Korean J Pathol. 2009;43(4):378-381.
- DOI: https://doi.org/10.4132/KoreanJPathol.2009.43.4.378
- 3,973 View
- 71 Download
-
Abstract
PDF
- Herein, we describe cases of pulmonary acute graft-versus-host disease (aGVHD) in two patients occurring after allogeneic hematopoietic stem cell transplantation (HSCT) due to precursor B-cell acute lymphoblastic leukemia in a 6-year-old patient and in acute myeloid leukemia in a 14-year-old boy. In both cases, chest CT revealed confluent ground-glass attenuation along the bronchovascular bundles, as well as some bronchial dilatation. Microscopically, in both cases we noted a characteristic bronchiolocentric pattern and bronchiolar epithelial changes, which included denudation of the bronchiolar epithelium, regenerating atypical cells, and wall thickening with subepithelial or transmural fibroblast proliferation, along with some lymphocytic infiltration. One patient died on day 86 after allogeneic HSCT due to sudden acute respiratory distress syndrome, and the other patient currently remains alive without active aGVHD. The authors' experiences in these two cases demonstrate that intense awareness of the pathologic findings of GVHD is mandatory after allogeneic HSCT.
- Alteration of Bile Acid Transporter Expression in Patients with Early Cholestasis Following Living Donor Liver Transplantation.
- Eun Sun Jung, Byung Kee Kim, So Youn Kim, Youn Soo Lee, Si Hyun Bae, Seung Kew Yoon, Jong Young Choi, Young Min Park, Dong Goo Kim
- Korean J Pathol. 2009;43(1):48-55.
- DOI: https://doi.org/10.4132/KoreanJPathol.2009.43.1.48
- 4,616 View
- 36 Download
-
Abstract
PDF
- BACKGROUND
Intrahepatic cholestasis can occur early after living donor liver transplantation (LDLT). We investigated the changes in the expressions of the bile acid transporters and the liver histology in the patients who suffered with early cholestasis (EC) following LDLT.
METHODS
The histological differences between 15 graft livers with EC after LDLT and 5 graft livers with biliary stricture following LDLT were evaluated. The hepatic mRNA levels of the bile canaliculi transporters (BSEP, MRP2, MRP3, MDR1, MDR3, NTCP) in 40 (20 graft livers, 20 matched donor livers) liver biopsy tissues were analyzed by performing real-time reverse-transcription polymerase chain reaction (RT-PCR).
RESULTS
Microscopic examination revealed hepatocellular and/or bile canalicular cholestasis around acinar zone 3 in the livers of the patients with EC. In the livers with biliary stricture, the cholestasis was dominantly observed in the hepatocytic cytoplasm and in the bile ductules around the portal area rather than around acinar zone 3. The BSEP and MRP2 mRNA levels in the EC livers were significantly reduced by 44% and 23%, respectively (p=0.000), compared to the matched donor livers. The levels of MDR3 and NTCP mRNA in the EC livers increased by 738% (p=0.000) and 281% (p<0.01), respectively. The change of the expressions of the bile acid transporters in the patients with biliary stricture was less significant than that in the EC group.
CONCLUSIONS
These results suggest that the altered expressions of the bile acid transporters may play a role in the pathogenesis of EC following LDLT.
- Cardiac Sarcoidosis Treated by Cardiac Transplantation: A Case Report.
- Jaejung Jang, Kwangseon Min, Gyeong cheon Jung, Jaejung Kim, Inchul Lee
- Korean J Pathol. 2001;35(1):71-75.
- 2,063 View
- 15 Download
-
Abstract
PDF
- Sarcoidosis, in general, has a low mortality rate. But cardiac sarcoidosis (CS) is a serious condition which may lead to death. Here, we report a rare case of CS that was treated by heart transplantation. A 47-year-old male had occasional syncopes and atypical chest pain. Ventricular tachycardia with right bundle branch block was noted by electrocardiogram. Multiple fixed myocardial perfusion defects in the interventricular septum and both the inferior-posterior ventricular walls were observed by thallium scan. Coronary angiography was unremarkable. Neither perihilar nor mediastinal lymphadenopathy was noted. The patient also suffered three times from tonic-clonic generalized seizures in 3 years, but no neurologic abnormalities were detected. The explanted heart displayed multiple white patches on the endomyocardial surface, measuring up to 8x7 cm. On microscopic examination, the lesion consisted of multiple well-formed and confluent granulomas with numerous scattered multinucleated giant cells, CD68-positive epithelioid histiocytes, and T-lymphocytes. Neither microorganisms nor foreign material was identified on special stain and culture study. It has been six months since the heart transplant, and the patient has been doing well.
- Pathological Analysis of Post-Transplantation Endomyocardial Biopsies.
- Jaegul Chung, Soonae Oak, Gheeyoung Choe, Gyungyub Gong, Jooryung Huh, Eunsil Yu, Inchul Lee, Meong Gun Song, Kwang Hyun Sohn, Jae Joong Kim, Jong Goo Lee
- Korean J Pathol. 1995;29(4):431-441.
- 2,470 View
- 17 Download
-
Abstract
PDF
- Heart transplantation was first performed in 1967. It is now regarded as a well-established treatment modality for end-stage cardiac diseases. Once the transplantation is performed, endomyocardial biopsy(EMB) is the examination of choice in monitoring the transplanted heart. We analyzed the pathological findings of follow-up EMB of 6 heart transplant patients. All patients have been suffered from severe heart failure. Four patients were adult male and two were adult females. All the hearts, except for one, displayed characteristic features of dilated cardiomyopathy. The remaining heart was diagnosed as having giant cell myocarditis. Post-transplantion EMBs were performed according to the protocol and standard cardiac biopsy grading of ISHT (1990). The standards were applied for grading of cellular rejection. In five patients, there were one or two episodes of biopsy proven acute rejection, grade II or IIIA without any clinical symptoms of rejection. Immediate "pulse therapy" was performed and follow-up biopsies were done. All episodes of rejection were cleared in subsequent biopsies. All patients are doing well without evidence of cardiac problem. The postoperative monitoring of acute rejection is critical since clinical signs of rejection are usually absent. At present, EMB is regarded as the most reliable method for diagnosis and grading of acute rejection and is an efficient guide to the monitoring of the cardiac recipients. Our experience of post-transplantation EMB corresponds with previously published reports.
- Image Analysis of Glomerular Changes in Patients with Post-transplant IgA Nephropathy.
- Kye Won Kwon, Hyeon Joo Jeong
- Korean J Pathol. 2001;35(3):206-211.
- 2,258 View
- 18 Download
-
Abstract
PDF
- BACKGROUND
IgA nephropathy after renal transplantation (post-transplant IgAN) may recapitulate the IgAN of native kidneys, however, little has been reported about the histologic characteristics. The aim of this study is to apply glomerular morphometry using an image analyser to examine the histologic characteristics of post-transplant IgAN.
METHODS
The outer margin of the glomerulus (Bowman's area, BA) and glomerular tuft area (GA) were traced manually. The measured area were automatically calculated by KS300 image analysis system (Kontron, Munchen, Germany). The mesangial area (MA) was calculated with a summing each manually traced mesangial area. The total number of glomerular (GC) and mesangial cells (MC) were counted. Eight cases of renal section obtained by nephrectomy due to renal cell carcinoma (normal control: N-CTRL) and nineteen cases of renal section obtained from post-transplantation patients without IgAN (transplantation control: Tx-CTRL) served as controls.
RESULTS
A total of 35 biopsies were finally selected for measurement. BA and GA of post-transplant IgAN were 1.6 and 1.4 times larger than the N-CTRL, respectively, and were not significantly different from Tx-CTRL. MA was 1.4 times significantly larger than that of the Tx-CTRL. As compared to that of the N-CTRL, it was 1.2 times larger, but this difference was not statistically significant. The GC and MC of post-transplant IgAN and the Tx-CTRL were significantly lower than the N-CTRL. There were no significant correlations between glomerular hypertrophy and duration after renal transplantation, mesangial changes, segmental sclerosis, or degree of renal cortical interstitial fibrosis in post-transplant IgAN.
CONCLUSIONS
Prominent glomerular hypertrophy and mesangial expansion suggest a hyperfiltration injury in post-transplant IgAN and a possible way to glomerulosclerosis.
- Posttransplant Lymphoproliferative Disorder: A Report of 4 Cases.
- Sunhee Chang, Jooryung Hugh, Kyung Mo Kim, Duck Jong Han, Seung Kyu Lee, Eunsil Yu
- Korean J Pathol. 2002;36(1):45-50.
- 2,653 View
- 14 Download
-
Abstract
PDF
- Posttransplant lymphoproliferative disorder (PTLD) is a proliferation of B-cells associated with Epstein-Barr virus (EBV) infection as a complication of immunosuppression, especially by FK506. We investigated four cases of PTLD which developed either in allografts or in other organs.
Case
1 was a 38-year-old woman, who developed monomorphic PTLD in a kidney 7 years and 7 months after renal transplantation. Case 2 was a 37-year-old man, who developed monomorphic PTLD in the right submandibular lymph node 4 months after liver transplantation. Case 3 was a 60-year-old man, who developed monomorphic PTLD in the liver 8 months after liver transplantation. Case 4 was a 2-year-old female child, who developed polymorphic PTLD in the colon, liver, and mesenteric lymph node 10 months after liver transplantation. FK506 was administered to case 4. EBV was identified in the tissues of all cases by immunohistochemistry and/or in situ hybridization.
- Recurrent Viral Hepatitis Following Liver Transplantation: Report of 4 Cases.
- Sunhee Chang, Kwangseon Min, Jaegul Jung, Ghil Suk Yoon, Seung Kyu Lee, Yung Sang Lee, Eunsil Yu
- Korean J Pathol. 2002;36(2):122-127.
- 2,297 View
- 13 Download
-
Abstract
PDF
- The recurrence of viral hepatitis B or C after liver transplantation is almost universal but their clinical courses and outcomes are vary widely. We investigated four cases of rapidly progressive and fatal recurrent viral hepatitis following liver transplantation, which were rapidly progressive and fatal. Case 1 was a 58-year-old male, who developed recurrent viral hepatitisC. Case 2, 3, and 4 were a 59-year-old female, a 42-year-old male, and a 50-year-old male, respectively, who developed recurrent viral hepatitis B. In cases 1 and 2, the histopathological features of the first liver biopsies were prominent ballooning degeneration of the hepatocytes but later biopsies revealed significant lobular activity. Case 3 began with a marked fatty change and mild lobular and porto-periportal activity and progressed to severe lobular activity and septal fibrosis. In case 4, the first liver biopsy revealed minimal lobular activity but the second biopsy revealed severe lobular activity.
- Multiple Kaposi's Sarcoma in the Renal Transplant Patient: A case report .
- Jae Kyung Koh, Eun Sun Jung, Youn Soo Lee, Seok Jin Kang, Byung Kee Kim, Sun Moo Kim
- Korean J Pathol. 1999;33(11):1097-1101.
- 2,332 View
- 19 Download
-
Abstract
PDF
- The Kaposi's sarcoma, which was found in an immunosuppressed patient of renal transplantation, may have been developed by long term use of immunosuppressant agent after the renal transplantation. The case was a 29-year-old woman who was diagnosed as chronic renal failure in 1988, and since then, she had been on CAPD until May, 1997. After the renal transplantation in May 1997, the patient has been prescribed cyclosporin and prednisone as immunosuppressant agent. In June 1997, she showed clinical symptom of Kaposi's sarcoma with multiple papules and nodules in the skin and viscera, such as ureter, urinary bladder, stomach, duodenum and subcutaneous tissue of the chest. Multiple excisional biopsies were carried out in the skin, ureter, urinary bladder, stomach and duodenum. All of excisional biopses indicated nodular stages with extensive proliferation of spindle shaped, somewhat pleomorphic cells which have slit-like vascular spaces, proliferation of small vessels, and extravasation of erythrocytes. These lesions nearly diminished after sytemic chemotherpy, excision and discontinuity of immunosuppressive agents.
- Pathologic Analysis of Endomyocardial Biopsies in Heart Transplantation.
- Mee Hye Oh, Jeong Wook Seo, Kook Yang Park, Young Tak Lee, Yoon Seop Jeong, Suk Keun Hong, Joon Ryang Rho, Byung Hee Oh, Sung Sook Kim
- Korean J Pathol. 1998;32(2):104-114.
- 2,456 View
- 26 Download
-
Abstract
PDF
- Endomyocardial biopsy (EMB) is a valuable diagnostic procedure for the surveillance of cardiac allograft rejection. Interpretation of individual cases is still problematic due to variations of findings for grading of rejection and other associated lesions. We reevaluated an experience on endomyocardial biopsies to develop better diagnostic criteria for rejection and other complications. Immunohistochemical studies against cytokines were performed to assess the usefulness of the method for the diagnosis or researches. A total of 249 EMBs taken from 33 cardiac allograft recipients were reviewed. There were 25 males and 8 females. Dilated cardiomyopathy was present (24 cases) and valvular heart disease (4 cases), restrictive cardiomyopathy (3 cases) were also common conditions. We applied the grading system of the International Society for Heart Transplantation (ISHT) for the assessment of acute cellular rejection. Grades of 0, 1A, 1B, 2, 3A and 3B were 39.0%, 28.1%, 11.2%, 11.5%, 12.4% and 1.6% respectively, but 3.2% were inadequate. Thirty five episodes of grade 3A or 3B were present in 17 patients. The response to therapy was assessed using a next follow up biopsy, which revealed resolving or resolved rejection in 85% of patients. The intensity of immunohistochemical stains for IL-6 and TNF-alpha was increased in proportion to the histologic grade but Quilty lesion and cardiomyopathy also showed a positive reaction. The other pathologic findings were ischemic change, previous biopsy site, interstitial edema and fibrosis, and Quilty lesion. These findings showed usefulness of endomyocardial biopsy not only for the evaluation of cardiac allograft rejection but also for the diagnosis of associated cardiac lesions. Immunohistochemical study of the cytokines was related to the degree of inflammation rather than degree of rejection.
- Giant Cell Myocarditis: A case report.
- Ho Jung Lee, Jae Gul Chung, In Chul Lee, Myeong Gun Song, Jae Jung Kim, Jong Goo Lee
- Korean J Pathol. 1996;30(6):523-527.
- 2,554 View
- 31 Download
-
Abstract
PDF
- Giant cell myocarditis(GCM) is a rare inflammatory heart disease which is characterized by multinucleated giant cells and a granulomatous reaction. It usually progresses rapidly and results in a fatal course. We report a patient with giant cell myocarditis who was treated by cardiac transplantation. A 35-year-old male was admitted with dyspnea which had developed 4 months before. On echocardiography, the right and left ventricles were markedly dilated and severe global hypokinesia was noted. He was diagosed with dilated cardiomyopathy with secondary severe mitral regurgitation. His cardiac function deteriorated progressively. He underwent orthotopic heart transplantation. Grossly the heart was enlarged, weighing 420gm and round with a blunt apex. Both right and left ventricles were markedly dilated. There were numerous white patches, measuring up to 4cm, throughout the epi- and myocardium. Microscopically, extensive fibrosis and multiple exuberant granulomas with numerous scattered multinucleated giant cells were seen. Lymphocytes and eosinophils were also frequent. Coronary arteries were unremarkable. Neither microorganisms nor foreign materials were found. By serial endomyocardial biopsies of the transplanted heart, only mild perivascular lymphocytic infiltration was occasionally observed without any evidence of rejection or recurrence of giant cell myocarditis. The patient's postoperative course has been uneventful so far(postoperative 21 months). The etiology of GCM remains to be clarified, although various factors are suspected. No matter what the cause, our experience suggests that this grave disease might be treated well by heart transplantation.
- Disseminated Systemic Candidiasis and Aspergillosis in a Liver Transplant Patient: An Autopsy Report.
- Na Rae Kim, Dae Su Kim, Young Hyeh Ko, Sung Joo Kim
- Korean J Pathol. 2002;36(5):348-352.
- 2,381 View
- 19 Download
-
Abstract
PDF
- Postoperative complications of liver transplantation include rejection, infection, hepatic vascular thrombus, and primary graft failure, etc. Among them, fungal infection shows nonspecific clinical symptoms and overlapping laboratory findings with variable etiologies causing post-transplant hepatic dysfunction. Therefore, early diagnosis of fungal infection is not easy. Here, we report an autopsy case of disseminated candidiasis and aspergillosis in a liver transplant patient. The case was at first misinterpreted as acute cellular rejection on biopsy because the histology of predominantly cellular infiltration, ductulitis and endothelialitis were similar to those of acute cellular rejection. On autopsy, the liver, lung and kidney showed multifocal hemorrhagic infarcts due to intra-arterial fungal emboli, which were composed mostly of candida species and a minor fraction of aspergillus. Fungal thrombi invading portal vein, intrahepatic arterioles with subsequent coagulation necrosis, venulitis and ductulitis were ascribed to the misdiagnosis on biopsies. It is unusual that systemic candidiasis, unlike aspergillosis, involves large arteries.
- Primary Sclerosing Cholangitis: A Report of Two Liver Explants.
- Sun Young Jun, Jung Sun Kim, Eun Sil Yu
- Korean J Pathol. 2002;36(6):420-424.
- 2,225 View
- 28 Download
-
Abstract
PDF
- Primary sclerosing cholangitis (PSC) is usually progressive to the end stage liver disease and a common indication for liver transplantation (LT). We report two cases of liver explants with PSC. Case 1 was that of a 35-year-old male who was admitted for 4 weeks because he had jaundice. He had been treated several times without receiving a definite diagnosis during the last 7 years because he was excreting dark urine. Case 2 was that of a 30-year-old female who had taken a prednisolone for 6 years for treatment of ulcerative colitis. She also had stones and underwent a cholecystectomy and choledocholithotomy 2 years ago. She had complained of epigastric pain and febrile sensation for 2 months. In both cases, serum levels of aspartate aminotransferase, alanine aminotransferase, alkaline phospatase, gamma glutamyl transpeptidase, and direct builirubin were elevated. Autoantibodies were not detected. Computerized tomography scan and endoscopic retrograde cholangiopancreatography revealed hepato-splenomegaly, stricture of intra- and extra-hepatic bile ducts, and beaded dilatation of the intrahepatic bile ducts. Despite stent insertions and medication, another episode of jaundice occurred in case 1 and cirrhosis finally developed in case 2. The histopathologic features of liver needle biopsy specimens were nonspecific, while explant livers displayed periductal fibrosis, ductopenia, and/or ductular proliferation, which are characteristic features for PSC.
- Cytologic Findings of Polyomavirus Infection in the Urine: A Case Report.
- Mi Seon Kwon, Young Shin Kim, Kyo Young Lee, Yeong Jin Choi, Chang Suk Kang, Sang In Shim
- J Pathol Transl Med. 1996;7(2):192-196.
- 2,815 View
- 28 Download
-
Abstract
PDF
- The principal significance of the urothelial changes caused by polyomavirus activation is in an erroneous diagnosis of urothelial cancer; however, the clue to their benign nature is the smooth structureless nuclear configuration and the relative paucity of affected cells. Though virologic studies and electron microscopy are usually needed to firmly establish the diagnosis, cytology is the most readily available and rapid means of establishing a presumptive diagnosis of human polyomavirus infection. A urine specimen of a 24-year-old man with hemorrhagic cystitis beginning two months after bone marrow transplantation for acute myeloblastic leukemia(M2) was submitted for cytologic evaluation. Cytologic findings revealed a few inclusion-bearing epithelial cells intermingled with erythrocytes, neutrophils, lymphocytes, and macrophages. Most of the inclusion-bearing -cells had large, round to ovoid nuclei almost completely filed with homogeneous dark, basophilic inclusion. The chromatin was clumped along the periphery and the cytoplasm was mostly degenerated. The other cells exhibited irregular inclusions attached to the nuclear membrane surrounded by an indistinct halo. These findings were consistent with polyomavirus infection.
- Flush Perfusion, Preservation and Reperfusion Effects in Lung Transplantation: Light Microscopic and Ultrastructural Study.
- Kun Young Kwon, Young Keun Lim, Jae Hoon Bae, Chang Kwon Park
- Korean J Pathol. 1998;32(11):967-977.
- 2,163 View
- 10 Download
-
Abstract
- This study was undertaken to investigate the morphologic changes following flushing, preservation and reperfusion procedures in a canine lung allotransplantation model. Donor lungs were flushed with modified Euro-Collins (MEC) solution, low potassium dextran glucose (LPDG) solution or University of Wisconsin (UW) solution, then stored at 10oC for 20 hours. Light microscopic and electron microscopic features of the lungs were examined after flushing, preservation and 2 hours after reperfusion. After flushing light microscopy showed focal mild alveolar collapse and interstitial edema. After preservation the lung tissue showed multiple foci of alveolar collapse, consolidation, and alveolar epithelial cell damage. After reperfusion the lung tissue showed diffuse alveolar collapse, consolidation and many destroyed cellular debris in the alveolar lumina. After flushing electron microscopy showed focal alveolar collapse and mild swelling of type I epithelial cells. After preservation both type I epithelial cells and endothelial cells were swollen and destroyed focally. Some type I epithelial cells were detached from the basal lamina. The endothelial cells showed luminal protrusion of tactile-like structure and vacuoles of the cytoplasm. After reperfusion the lung tissue showed fibrin material in the alveoli, prominent type I epithelial cell swelling with fragmented cytoplasmic debris and marked endothelial cell swelling with vacuoles or tactile-like projections. The alveolar macrophages showed active phagocytosis. After preservation scanning electron microscopic examination of the pulmonary arteries showed multiple patchy areas of swelling or conglomerated lesions in the inner surface of the pulmonary arteries. In conclusion, the ultrastructural changes associated with flushing were mild in severity, the donor lungs were injured during the preservation, and further damage occurred during the reperfusion.
- Immunohistochemical Profile of Acute Cellular Rejection in Renal Allograft.
- Jongha Park, Seung Woon Byun, Eunsil Yu, Su Kil Park, Duck Jong Han, Yong Mee Cho
- Korean J Pathol. 2007;41(1):15-20.
- 2,344 View
- 25 Download
-
Abstract
PDF
- BACKGROUND
We wanted to find an adjunctive marker(s) in renal allograft biopsies for predicting acute cellular rejection (ACR), and so the expression patterns of immune-related molecules were compared between ACR, borderline ACR and non-ACR cases.
METHODS
The expression patterns of Fas ligand (FasL), HLA-DR, granzyme B, caspase-3, CD56, interferon stimulated growth factor-3 (ISGF-3), and CD53 were assessed via immunohistochemical study in 75 allograft biopsies from patients with ACR (n=19), borderline ACR (n=22), and non-ACR (n=34).
RESULTS
Compared to those of the non-ACR group, the ACR group revealed an elevated number of FasL positive interstitial inflammatory cells, HLA-DR positive tubular inflammatory cells, cytoplasmic caspase-3 positive tubular epithelial cells, granzyme B positive interstitial mononuclear inflammatory cells and CD53 positive interstitial inflammatory cells. The expression patterns of the borderline ACR group were similar to those of non-ACR group, except for the intensity of FasL in the tubular epithelial cells.
CONCLUSIONS
Immunohistochemical investigations of the adjunctive markers FasL, HLA-DR, granzyme B, caspase-3 and CD56 can be useful for making the diagnosis of ACR.
 First
First Prev
Prev


