 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Articles
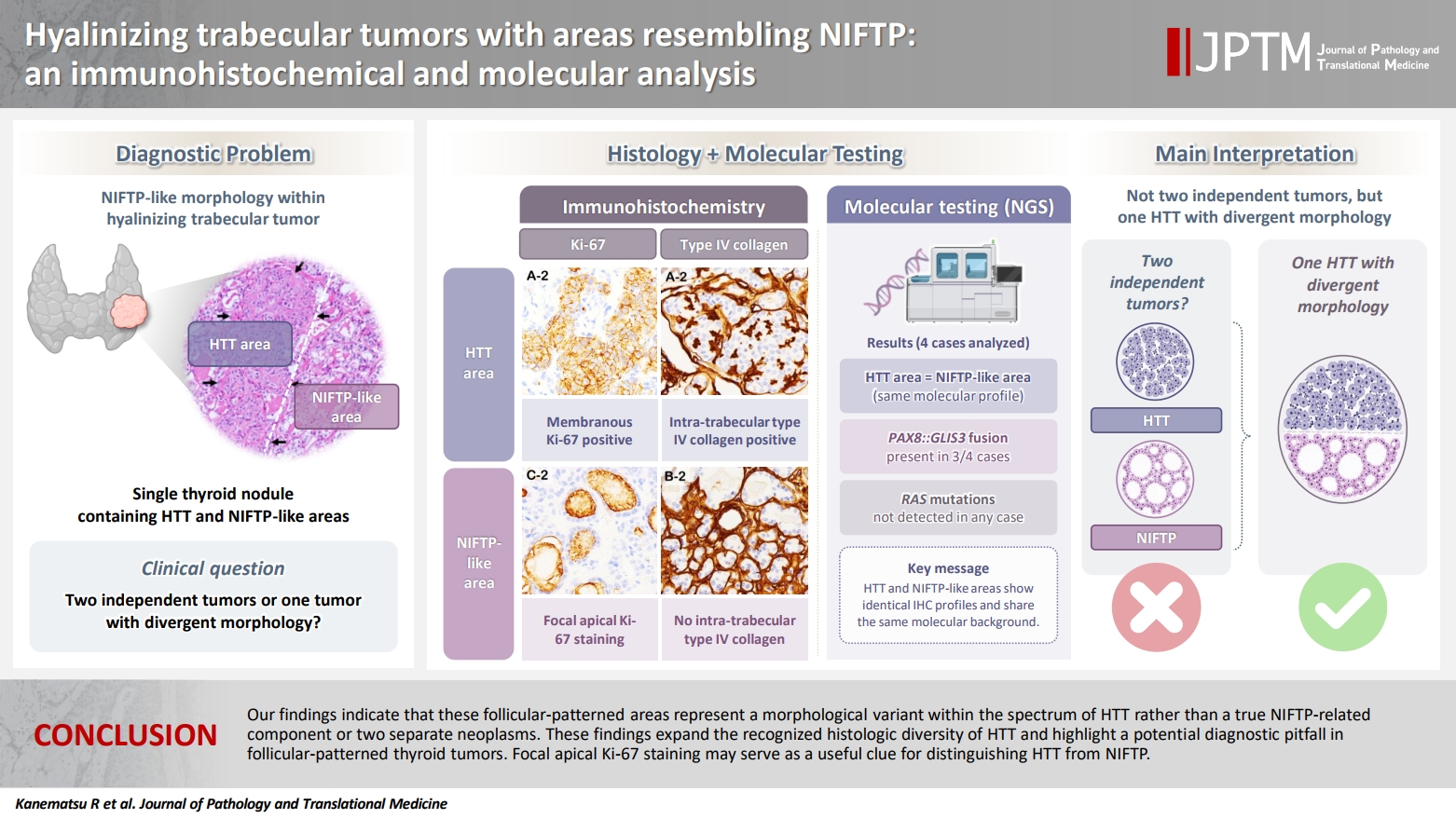
- Hyalinizing trabecular tumors with areas resembling noninvasive follicular thyroid neoplasm with papillary‑like nuclear features: an immunohistochemical and molecular analysis
- Risa Kanematsu, Mitsuyoshi Hirokawa, Ayana Suzuki, Miyoko Higuchi, Satomi Usuki, Hiroshi Kamma, Takashi Akamizu
- J Pathol Transl Med. 2026;60(4):436-443. Published online July 15, 2026
- DOI: https://doi.org/10.4132/jptm.2026.06.07
- 150 View
- 3 Download
-
 Abstract
Abstract
 PDF
PDF - Background
The coexistence of hyalinizing trabecular tumor (HTT) and areas with a morphology of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) within a single thyroid nodule has not been previously reported. We aimed to determine whether such tumors represent two independent neoplasms or a single tumor exhibiting divergent morphology. Methods: Ten tumors containing both HTT and NIFTP-like areas were examined. The term “NIFTP-like” was used strictly as a descriptive morphological designation for areas that fulfill the histologic criteria of NIFTP. Immunohistochemical analyses of Ki-67 (MIB-1) and type IV collagen and targeted molecular testing were performed. Ten NIFTPs, 10 follicular adenomas, and three HTTs were used as controls. Results: HTT components consistently showed characteristic membranous Ki-67 staining and intra-trabecular type IV collagen deposition, whereas NIFTP-like areas lacked these features, except for focal apical Ki-67 staining. Intranuclear cytoplasmic inclusions in HTT were positive for type IV collagen. NIFTPs showed neither membranous Ki-67 nor intra-trabecular type IV collagen. Molecular analysis demonstrated identical profiles between HTT components and NIFTP-like areas: three tumors harbored PAX8::GLIS3 fusions, and none showed RAS mutations. Pure HTT controls exhibited the same pattern. Conclusions: Our findings indicate that these follicular-patterned areas represent a morphological variant within the spectrum of HTT rather than a true NIFTP-related component or two separate neoplasms. These findings expand the recognized histologic diversity of HTT and highlight a potential diagnostic pitfall in follicular-patterned thyroid tumors. Focal apical Ki-67 staining may serve as a useful clue for distinguishing HTT from NIFTP.
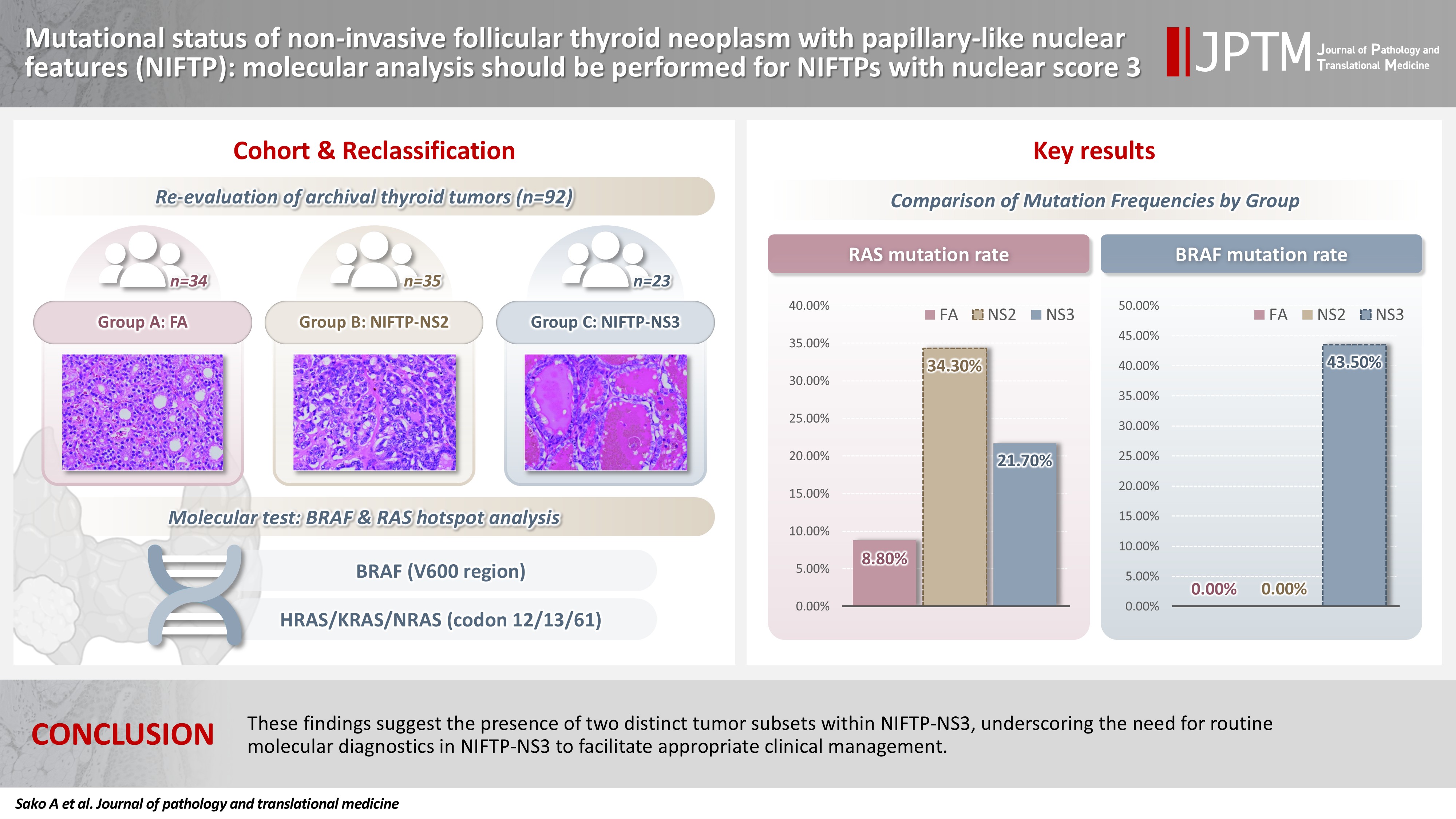
- Mutational status of non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP): molecular analysis should be performed for NIFTPs with nuclear score 3
- Ayaka Sako, Mitsuyoshi Hirokawa, Michiko Matsuse, Miyoko Higuchi, Akira Miyauchi, Takashi Akamizu, Atsushi Kawakami, Norisato Mitsutake
- J Pathol Transl Med. 2026;60(2):214-219. Published online February 23, 2026
- DOI: https://doi.org/10.4132/jptm.2025.12.06
- 2,110 View
- 221 Download
-
Abstract
PDF
- Background
The classification of non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) was introduced to prevent the overtreatment of indolent tumors that were formerly diagnosed as non-invasive encapsulated follicular variant papillary thyroid carcinomas (NIEFV-PTCs). Although NIFTP was initially estimated to account for 10%–20% of papillary thyroid carcinomas in Western populations, its incidence is substantially lower in Asian cohorts. However, a multi-institutional Japanese study revealed that 31.0% of tumors previously diagnosed as follicular adenomas (FAs) were reclassified as NIFTPs. NIFTP diagnosis requires a nuclear score (NS) of 2–3, and according to the recent World Health Organization criteria, molecular analysis is recommended, but not mandatory, to exclude high-risk subtypes, namely cases with the BRAFV600E mutation, particularly for NS3 tumors. Methods: We performed genetic analysis on 92 archival thyroid tumor samples, including 69 previously diagnosed as FA, of which 34 remained as FA upon re-evaluation (group A) and 35 were reclassified as NIFTP with NS2 (group B). Additional 23 tumors previously diagnosed as NIEFV-PTC were reclassified as NIFTP with NS3 (group C). Results: RAS mutations were detected in 8.8%, 34.3%, and 21.7% of the tumor samples in groups A, B, and C, respectively, whereas BRAF mutations were present in 43.5% of the tumor samples in group C only. Conclusions: These findings suggest the presence of two distinct tumor subsets within NIFTP-NS3, underscoring the need for routine molecular diagnostics in NIFTP-NS3 to facilitate appropriate clinical management.
 First
First Prev
Prev


