 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Articles
- Categorizing high-grade serous ovarian carcinoma into clinically relevant subgroups using deep learning–based histomic clusters
- Byungsoo Ahn, Eunhyang Park
- J Pathol Transl Med. 2025;59(2):91-104. Published online February 18, 2025
- DOI: https://doi.org/10.4132/jptm.2024.10.23
- 8,041 View
- 276 Download
- 1 Web of Science
- 2 Crossref
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background
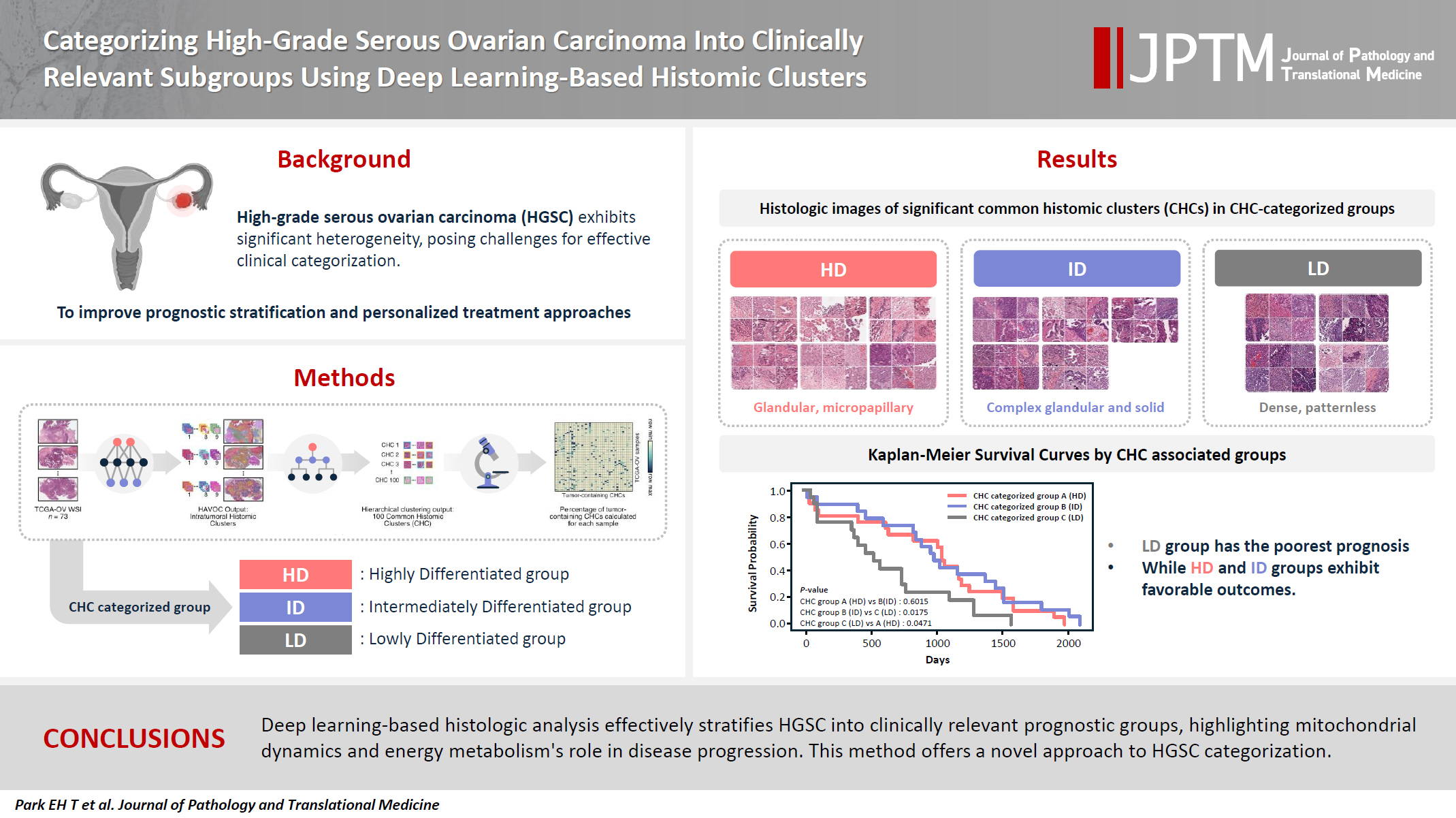
High-grade serous ovarian carcinoma (HGSC) exhibits significant heterogeneity, posing challenges for effective clinical categorization. Understanding the histomorphological diversity within HGSC could lead to improved prognostic stratification and personalized treatment approaches. Methods: We applied the Histomic Atlases of Variation Of Cancers model to whole slide images from The Cancer Genome Atlas dataset for ovarian cancer. Histologically distinct tumor clones were grouped into common histomic clusters. Principal component analysis and K-means clustering classified HGSC samples into three groups: highly differentiated (HD), intermediately differentiated (ID), and lowly differentiated (LD). Results: HD tumors showed diverse patterns, lower densities, and stronger eosin staining. ID tumors had intermediate densities and balanced staining, while LD tumors were dense, patternless, and strongly hematoxylin-stained. RNA sequencing revealed distinct patterns in mitochondrial oxidative phosphorylation and energy metabolism, with upregulation in the HD, downregulation in the LD, and the ID positioned in between. Survival analysis showed significantly lower overall survival for the LD compared to the HD and ID, underscoring the critical role of mitochondrial dynamics and energy metabolism in HGSC progression. Conclusions: Deep learning-based histologic analysis effectively stratifies HGSC into clinically relevant prognostic groups, highlighting the role of mitochondrial dynamics and energy metabolism in disease progression. This method offers a novel approach to HGSC categorization. -
Citations
Citations to this article as recorded by
- Ovarian Cancer: Epidemiology, Disease Mechanisms, New Diagnosis and Treatment Strategies, and Research Directions
Zunera Khalid, Weirong Fan, Farah Nazir, Yixiang Xing, Tengchuan Jin
iNew Medicine.2026;[Epub] CrossRef - Learning Disabilities in the 21st Century: Integrating Neuroscience, Education, and Technology for Better Outcomes
Syed Mohammed Basheeruddin Asdaq, Ahmad H. Alhowail, Syed Imam Rabbani, Naira Nayeem, Syed Mohammed Emaduddin Asdaq, Faiqa Nausheen
SAGE Open.2025;[Epub] CrossRef
- Ovarian Cancer: Epidemiology, Disease Mechanisms, New Diagnosis and Treatment Strategies, and Research Directions
- Serous Adenocarcinoma of Fallopian Tubes: Histological and Immunohistochemical Aspects
- Natalia Hyriavenko, Mykola Lyndin, Kateryna Sikora, Artem Piddubnyi, Ludmila Karpenko, Olha Kravtsova, Dmytrii Hyriavenko, Olena Diachenko, Vladyslav Sikora, Anatolii Romaniuk
- J Pathol Transl Med. 2019;53(4):236-243. Published online April 11, 2019
- DOI: https://doi.org/10.4132/jptm.2019.03.21
- 9,699 View
- 133 Download
- 4 Web of Science
- 6 Crossref
-
Abstract
PDF
- Background
Although primary cancer of the fallopian tubes is a relatively rare type of tumor in female reproductive organs, its mortality is quite high. It is important to identify molecular and biological markers of this malignancy that determine its specific phenotype.
Methods
The study was carried out on samples received from 71 female patients with primary cancer of the fallopian tubes. The main molecular and biological properties, including hormone status (estrogen receptor [ER], progesterone receptor [PR]), human epidermal growth factor receptor (HER2)/neu expression, proliferative potential (Ki-67), apoptosis (p53, Bcl-2), and pro-angiogenic (vascular endothelial growth factor) quality of serous tumors were studied in comparison with clinical and morphological characteristics.
Results
ER and PR expression is accompanied by low grade neoplasia, early clinical disease stage, and absence of lymphogenic metastasis (p < .001). HER2/neu expression is not typical for primary cancer of the fallopian tubes. Ki-67 expression is characterized by an inverse correlation with ER and PR (p < .05) and is associated with lymphogenic metastasis (p < .01). p53+ status correlates with high grade malignancy, tumor progression, metastasis, negative ER/PR (p < .001), and negative Bcl-2 status (p < .05). Positive Bcl-2 status is positively correlated with ER and PR expression and low grade malignancy.
Conclusions
Complex morphologic (histological and immunohistochemical) study of postoperative material allows estimation of the degree of malignancy and tumor spread to enable appropriate treatment for each case. -
Citations
Citations to this article as recorded by- Clinical and Morphological Analysis of Odontogenic Tumors and Tooth Developmental Anomalies
Yе.V. Kuzenko, S.M. Hermanchuk, O.O. Mykhno, D.H. Tsepochko, O.V. Kuzenko, A.Yu. Olishkevych
Kharkiv Dental Journal.2025; : 275. CrossRef - Rare non-serous fallopian tube cancers: institutional experience and literature review
Dmitrii Sumtsov, Georgyi Sumtsov, Nataliia Hyriavenko, Mykola Lyndin, Kateryna Sikora, Nataliia Kalashnik, Svitlana Smiian, Igor Gladchuk
Wiener Medizinische Wochenschrift.2024; 174(9-10): 199. CrossRef - UŞAQLIQ BORULARININ BİRİNCİLİ XƏRÇƏNGİ: DİAQNOSTİKASI VƏ MÜALİCƏSİNİN NƏTİCƏLƏRİ
D.G. Sumtsov, G.O. Sumtsov, N.I. Hyriavenko, S.A. Smiian, N.V. Kalashnyk, K.O. Sikora, N.M. Rozhkovska, I.Z. Gladchuk
Azerbaijan Medical Journal.2023; (4): 75. CrossRef - FEATURES OF ENDOMETRIUM STRUCTURE IN ALCOHOL-ABUSING HIV-INFECTED INDIVIDUALS
M. Lytvynenko
Inter Collegas.2021; 8(1): 52. CrossRef - Concurrent Clostridial Enteritis and Oviductal Adenocarcinoma with Carcinomatosis in an Adult Alpaca (Vicugna pacos)
Mandy Womble, Megan E. Schreeg, Allison Hoch, Enoch B. de Souza Meira, Derek Foster, Christopher Premanandan, Tatiane T. Negrão Watanabe
Journal of Comparative Pathology.2021; 189: 52. CrossRef - Problems of primary fallopian tube cancer diagnostics during and after surgery
D.G. Sumtsov, I.Z. Gladchuk, G.O. Sumtsov, N.I. Hyriavenko, M.S. Lyndin, V.V. Sikora, V.M. Zaporozhan
REPRODUCTIVE ENDOCRINOLOGY.2021; (59): 66. CrossRef
- Clinical and Morphological Analysis of Odontogenic Tumors and Tooth Developmental Anomalies
Brief Case Report
- The Limitations of Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology in the Diagnosis of Pancreatic Serous Cystadenoma: A Brief Case Report
- Heae Surng Park, Sun Och Yoon, Beom Jin Lim, Joo Hee Kim, Soon Won Hong
- Korean J Pathol. 2014;48(5):405-408. Published online October 27, 2014
- DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.5.405
- 9,210 View
- 63 Download
Case Report
- Simultaneous Pancreatic Serous Microcystic Adenoma and Intraductal Papillary Mucinous Tumor of the Pancreas: A Case Report.
- Hyoung Jong Kwak, Young Kon Kim, Baik Hwan Cho, Woo Sung Moon
- Korean J Pathol. 2011;45:S29-S31.
- DOI: https://doi.org/10.4132/KoreanJPathol.2011.45.S1.S29
- 3,934 View
- 24 Download
-
Abstract
PDF
- Serous cystadenomas of the pancreas account for approximately a third of pancreatic cystic neoplasms. Their coexistence with a second tumor is extremely rare. We now report a case of a serous microcystic adenoma combined with an intraductal papillary mucinous tumor of the pancreas in a 69-year-old man. Abdominal computed tomography scans demonstrated an incidental cystic mass in the body with cystic dilatation of the duct in the head of the pancreas. Central pancreatectomy with pancreatico-jejunostomy, and cyst excision of the pancreatic head were performed. Histologic examination demonstrated a serous microcystic cystadenoma in the body coexisting with an intraductal papillary mucinous adenoma in the head of the pancreas. This case study highlights the importance of careful intra-operative and pathologic examination for synchronous pancreatic tumors.
Original Article
- Cytologic Features of Endometral Papillary Serous Carchinoma.
- Gu Kong, Eun Kyoung Hong, Jung Dal Lee
- J Pathol Transl Med. 1990;1(2):121-128.
- 2,346 View
- 22 Download
-
Abstract
PDF
- Endometrial papillary serous carcinoma (EPSC) is a distinct variant of endometrial adenocarcinoma that histologically resembles ovarian serous papillary adenocarcinoma and has an aggressive clinical course. Usually, the tumor is diagnosed at the advanced stage. The tumor has well confused with metastatic ovarian tumor of identical histology. Diagnosis of EPSC should be considered when the cervico-vaginal smear reveals numerous papillary clusters of tumor cells with macronucleoli and psammoma bodies. Recently, we have experienced two cases of EPSC diagnosed on cervico-vaginal smears, which revealed characteristic cytologic features including numerous papillary clusters of tumor cells with macronucleoli. The cytologic diagnoses were confirmed on histologic sections.
Case Report
- Carcinosarcoma in Recurrent Lesion of Serous Cystadenocarcinoma of the Ovary: A case report.
- Kyu Yun Jang, Woo Sung Moon, Dong Geun Lee
- Korean J Pathol. 1999;33(3):221-224.
- 2,189 View
- 11 Download
-
Abstract
PDF
- Neoplasms showing both carcinomatous and sarcomatous features are well established, and have been reported in practically every organ where carcinoma can occur. But the difference in terminology and difficulties in histopathologic interpretation have hampered adequate understanding of these neoplasms. We report a case of carcinosarcoma in the recurrent form of serous cystadenocarcinoma of the ovary. The patient was a 64-year-old female who underwent total hysterectomy and bilateral salpingoophorectomy three years ago, due to perforated papillary serous cysta denocarcinoma of the right ovary. Recurrent pelvic masses contained both carcinomatous and sarcomatous components. Morphological transition between carcinomatous and sarcomatous components, and epithelial characteristics in the sarcomatous component by immunohistochemistry were recognized. We postulate the histopathogenetic mechanism based on the phenotypic conversion of carcinoma into sarcoma in the carcinosarcoma.
In Vitro
- Ovarian Serous Borderline Tumors with Peritoneal Implants: A clinicopathologic and flow cytometric DNA analysis of 5 cases.
- Kyu Rae Kim, Kwang Yul Cha, Soon Hee Jung, Woo Hee Jung, Dong Hee Choi, Jong Wook Kim
- Korean J Pathol. 1993;27(2):143-151.
- 2,631 View
- 21 Download
-
Abstract
PDF
- Five cases of ovarian serous borderline tumor associated with multiple peritoneal implants were analysed. The age of 5 patients ranged from 34 to 45(mean: 39) years at the time of diagnosis. Two patients presented with secondary infertility underwent hyperstimulation of the ovary under the in vitro fertilization program. One patient was presented with abdominal pain and the remaining two with lower abdominal mass accompanied by abdominal pain. Serous surface papilloma of borderline malignancy, involving one or both ovaries, was present in all 5 cases and papillary serous cystic tumor of borderline malignancy was associated simultaneously in one or both ovaries in all cases. Marked adhesions between the pelvic organs, and multiple granularities and nodularities of the omentum and peritoneum were noted. Microscopically, the peritoneal lesions were composed of noninvasive implants of tumor cells and pasmmoma bodies on the surface of entire pelvic and abdominal organs. Flow cytometric analysis of nuclear DNA content from paraffin-embedded tissue fo primary ovarian tumor classified as aneuploidy in 3 cases and as diploidy in 2 cases. The DNA index of the aneuploid tumors ranged from 1.21 to 1.37. Four patients underwent hysterectomy, bilateral salpingo-oophorectomy and partial omentectomy in which two were followed by chemotherapy and one case underwent bilateral salpingo-oophorectomy.
Original Articles
- Differential Diagnosis of Ovarian Mucinous, Serous, and Endometrioid Adenocarcinoma in Peritoneal Washing Cytology .
- Shi Nae Lee, In Ae Park
- J Pathol Transl Med. 2000;11(2):83-88.
- 3,841 View
- 78 Download
-
Abstract
PDF
- This study presents the cytologic features of peritoneal washings, with particular emphasis on the cytologic discrimination among serous, mucinous, and endometrioid adenocarcinoma of the ovary. We selected histologically confirmed 27 cases of peritoneal washing : 8 cases of serous cystadenocarcinomas, 5 cases of mucinous cystadenocarcinomas, and 14 cases of endometrioid adenocarcinomas. The most frequent cytologic pattern of three tumors was clusters. Ball pattern was found in serous cystadenocarcinoma(36%) and acinar pattern in endometrioid adenocarcinoma (36%). Mucinous adenocarcinoma showed mucoid background(100%) and endometrioid adenocarcinoma revealed inflammatory background(43%). The cytoplasmic vacuoles were noted in 80%, 13%, and 43% of mucinous, serous, and endometrioid adenocarcinoma, respectively. The endometrioid adenocarcinoma showed prominent nucleoli(64%). In conclusion, the cytologic findings of mucinous cystadenocarcinoma were different from that of serous and endometrioid carcinomas, such as mucoid background, abundant cytoplasm with vacuolated cytoplasm, and peripherally located cytoplasm. Although endometrioid carcinoma showed acinar pattern and prominent nucleoli, the differential diagnosis between serous cystadenocarcinoma and endometrioid adenocarcinoma in peritoneal washing cytology was not always possible.
- A Multiinstitutional Consensus Study on the Pathologic Diagnosis of Endometrial Hyperplasia and Carcinoma.
- Kwang Sun Suh, Insun Kim, Moon Hyang Park, Geung Hwan Ahn, Jin Hee Sohn, In Ae Park, Hye Kyoung Yoon, Kyu Rae Kim, Hee Jung An, Dong Won Kim, Mi Jin Kim, Hee Jae Joo, Eun Kyung Kim, Young Hee Choi, Chong Woo Yoo, Kyung Un Choi, Sang Yeop Yi, Hye Sun Kim, Sung Ran Hong, Hee Jeong Lee, Sun Lee
- Korean J Pathol. 2008;42(2):87-93.
- 2,629 View
- 26 Download
-
Abstract
PDF
- BACKGROUND
The purpose of this study was to examine the reproducibility of both the diagnosis of endometrial hyperplasia (EH) or adenocarcinoma, and the histologic grading (HG) of endometrioid adenocarcinoma (EC).
METHODS
Ninety-three cases of EH or adenocarcinomas were reviewed independently by 21 pathologists of the Gynecologic Pathology Study Group. A consensus diagnosis was defined as agreement among more than two thirds of the 21 pathologists.
RESULTS
There was no agreement on the diagnosis in 13 cases (14.0%). According to the consensus review, six of the 11 EH cases (54.5%) were diagnosed as EH, 48 of the 57 EC cases (84.2%) were EC, and 5 of the 6 serous carcinomas (SC) (83.3%) were SC. There was no consensus for the 6 atypical EH (AEH) cases. On the HG of EC, there was no agreement in 2 cases (3.5%). According to the consensus review, 30 of the 33 G1 cases (90.9%) were G1, 11 of the 18 G2 cases (61.1%) were G2, and 4 of the 4 G3 cases (100.0%) were G3.
CONCLUSIONS
The consensus study showed high agreement for both EC and SC, but there was no consensus for AEH. The reproducibility for the HG of G2 was poor. We suggest that simplification of the classification of EH and a two-tiered grading system for EC will be necessary.
Case Reports
- Papillary Serous Cystadenoma of Borderline Malignancy Arising from a Paramesonephric Parovarian Cyst: A case report.
- Ji Han Jung, Youn Soo Lee, Seok Jin Kang, Byung Kee Kim, Sang In Shim
- Korean J Pathol. 1999;33(6):457-459.
- 2,339 View
- 22 Download
-
Abstract
PDF
- Primary malignant parovarian epithelial tumors are extremely rare, with only 56 cases previously reported in the world literature. Most parovarian epithelial tumors are of paramesonephric (Mullerian) origin. In this article, we report the first case in the Korean literature of papillary serous cystadenoma of borderline malignancy from paramesonephric parovarian cyst. This case presented here is of particular interest since this neoplasm is rare. A 48-year-old female underwent a hysterectomy with bilateral adnexectomy and pelvic lymph node dissection for a cystic tumor of the right parovarian area. The tumor, measuring 13 cm in diameter, was apart from the ovaries, fallopian tubes and uterus. The cyst wall had well-developed smooth muscle layers. The cyst was lined with mildly atypical ciliated and non-ciliated low columnar cells compatible with those of paramesonephric origin. From the inner surface of the cyst several cauliflower-like structures projected into the lumen. They were of a predominantly papillary architecture covered by atypical epithelial cells with piling-up and occasional glandular growth. No destructive stromal invasion was identified.
- Macrocystic Form of Serous Cystadenoma of the Pancreas: Two Cases Report.
- Ki Seok Jang, Hyo Jin Lee, Moon Hyang Park
- Korean J Pathol. 2004;38(6):423-426.
- 2,370 View
- 24 Download
-
Abstract
PDF
- The macrocystic form of serous cystadenoma of the pancreas is an uncommon benign neoplasm composed of few, relatively large cysts that are lined by uniform, glycogen-rich, cuboidal epithelial cells. We report here on two cases of pathologically proven macrocystic serous cystadenoma of the pancreas in a 45-year-old female patient and a 53-year-old female patient. Both these cysts were lined by low cuboidal epithelia without any evidence of mucin production. There was also no evidence of pancreatitis. These tumors were radiologically suspected as being mucinous cystic neoplasm or pseudocysts. Although the microscopic and immunohistochemical studies of the macrocystic variant are not different from the conventional serous microcystic cystadenoma, their unusual macroscopic features can lead to confusion for the clinicians and radiologists.
- Paratesticular Papillary Serous Tumor of Low Malignant Potential: A Case Report.
- Moon Il Park, Hun Soo Kim, Kwang Sun Suh, Dae Young Kang
- Korean J Pathol. 2004;38(6):427-429.
- 2,243 View
- 21 Download
-
Abstract
PDF
- Paratesticular papillary serous tumors have been rarely reported, and they often resemble ovarian serous tumors of borderline malignancy. We experienced a case of papillary serous tumor in the left paratestis of a 39-year-old man. This is the second case reported in the Korean literature. The tumor, which was found incidentally during an operation for a hydrocele, was composed of papillary structures lined by cuboidal to columnar epithelial cells that displayed low cytologic atypia and frequent psammoma bodies.
- Serous Cystadenoma of the Pancreas: A case report.
- Young Kyoung Bae, Woo Young Jang, Kyoung Chan Choi, Joon Hyuk Choi, Won Hee Choi
- Korean J Pathol. 1996;30(1):68-71.
- 2,695 View
- 30 Download
-
Abstract
PDF
- Serous cystadenoma of the pancreas, also known as microcystic adenoma or glycogen-rich cystadenoma, is an unusually benign tumor. It is usually large and composed microscopically of many small cysts lined by small, cuboidal or flattened cells containing abundant glycogen. It has been suggested that serous cystadenoma probably arise from the ductular cells or centroacinar cells. Herein, we report on a case of serous cystadenoma of the pancreas in a 55-year-old female. The tumor, measuring 13.5x11.5x10.0 cm, was located in the head of the pancreas and the cut surface revealed a sponge-like appearance due to innumerable tiny cysts containing clear serous fluid. Microscopic analysis showed cystic spaces lined by cuboidal cells with intracytoplasmic glycogen.
- Sex Cord Tumor with Annular Tubules and Serous Surface Papillary Carcinoma of the Ovary: A case report.
- Dae su Kim, Sang Yong Song, Geung hwan Ahn
- Korean J Pathol. 1999;33(8):627-630.
- 2,295 View
- 22 Download
-
Abstract
PDF
- Sex cord tumor with annular tubules (SCTAT) is a rare ovarian neoplasm which usually occurs in two forms. In patients associated with Peutz-Jeghers syndrome, the tumors are usually small, bilateral or multifocal, and show benign clinical course. However, tumors from patients without the syndrome are often large, usually unilateral, and rarely show malignant behavior. Serous surface papillary carcinoma (SSPC) is an aggressive neoplasm which involves peritoneal linings, including ovarian surface. Recently, we encountered a case of an unusual combination of SCTAT and SSPC in the ovary of a 55-year-old Korean woman presented with abdominal distention for one year. Systemic review and physical examination were within normal limit, except for abdominal discomfort and distention. There was no stigmata of Peutz-Jeghers syndrome in all diagnostic examinations, including gastroscopy and colonoscopy. Pelvic computed tomography showed adnexal mass with multiple peritoneal nodules. Exploration revealed uterine and ovarian surfaces covered with multiple, yellow-white papillary nodules. However, the sizes of both ovaries were within normal limit. Typical serous papillary carcinomas were identified in nodules from peritoneum and ovarian surfaces. Well-circumscribed columnar epithelial cell nests composed of ring-shaped tubules encircling hyalinized basement membrane-like materials were found in the ovary away from serous surface papillary carcinoma.
Original Articles
- Expression of Actin-bundling Protein Fascin and its Relationship with Altered E-cadherin and beta-catenin Expressions in Ovarian Serous Neoplasms.
- Eun Yoon Cho, YoonLa Choi, Seoung Wan Chae, Eo Jin Kim, Kyehyun Kim, Geung Hwan Ahn, Jin Hee Sohn
- Korean J Pathol. 2005;39(4):258-264.
- 2,489 View
- 18 Download
-
Abstract
PDF
- Background
: Fascin, an actin-bundling protein, has been found in specialized normal cells, including the neuronal, endothelial and dendritic cells, and its expression is known to be greatly increased in various human neoplasms. Methods : Immunohistochemical stainings for fascin, betacatenin, and E-cadherin were performed in normal ovary tissue (n=13), and in benign (n=14), borderline (n=32), and malignant (n=74) ovarian serous neoplasms. We evaluated the fascin expression, and its relationship with the betacatenin and E-cadherin expressions, as well as the clinicopathologic factors. Results : Fascin expression was detected in the majority of the borderline (100%, 32/32) and malignant tumors (90.5%, 67/74), but it was not seen in the normal ovarian surface epithelial cells and the benign tumors (p<0.001). Fascin expression was significantly correlated with the occurrence of peritoneal metastases in the carcinomas (p=0.043). A significant relationship between the expressions of fascin and betacatenin (p=0.046), as well as E-cadherin (p=0.035) was noted. There was no significant correlation with the tumor grade of carcinoma, the FIGO stage, tumor recurrence, tumor-related death and the survival rate. Conclusions : In ovarian serous neoplasms, the fascin expression may be closely linked with tumor progression and metastasis, and it was associated with the up-regulation of betacatenin and E-cadherin.
- Ovarian Borderline Epithelial Tumors.
- Geunghwan Ahn
- Korean J Pathol. 2005;39(5):291-300.
- 2,611 View
- 27 Download
-
Abstract
PDF
- Ovarian borderline epithelial tumors are abnormal proliferative epithelial lesions without obvious invasion of the stroma of the ovary, a finding distinguishing between borderline tumors and carcinoma. There have been controversies regarding the terminology and diagnostic feature of the tumors, even though these tumors have been accepted as a distinct entity in WHO classification of ovarian epithelial tumors. This review is limited to serous and mucinous borderline tumors which are the most common and about which many clinicopathological studies have been undertaken. It has been agreed that "micropapillary carcinoma" espoused by a group of pathologists is a micropapillary variant of serous borderline tumor in the borderline ovarian tumor workshop. Diagnostic criteria of invasive implants needs further study but invasion of underlying normal tissue was reported to be correlated well with prognosis. Other issues such as diagnostic criteria of microinvasion and multiplicity of serous borderline tumors have been presented. The sole diagnostic criteria agreed upon for the diagnosis of intraepithelial carcinoma in the mucinous borderline tumor was the presence of severe cytological atypia. It was also agreed that the ovarian tumors associated with pseudomyxoma peritonei are almost invariably from gastrointestinal tract, usually appendix. Stratification and complex intracystic growth without severe cytological atypia are considered to be characteristics of mucinous borderline tumors. Diagnostic criteria of microinvasion and two types of invasion, expansile and infiltrative invasion, have also been discussed.
- A Serous Papillary Cystadenoma of Low Malignant Potential in Paratesticular Tissue.
- Keum Min Park, Nam Bok Cho, Kye Yong Song
- Korean J Pathol. 1996;30(5):463-465.
- 2,484 View
- 15 Download
-
Abstract
PDF
- The serous papillary cystadenoma of low malignant potential in the paratesticular tissue is a tumor characterized by its resemblance to ovarian serous papillary tumor of low malignant potential. Several possible origins have been proposed but it is thought to originate from the Mullerian-type epithelium just like ovarian serous tumor of low grade malignancy. Because of the rarity of this tumor, the natural history and treatment have not been established. Herein we report on a serous papillary cystadenoma arising in the paratesticular tissue of a 12 year old . To our knowledge, this is the first reported case in the Korean literature. The size of this cystic tumor in this patient was 0.9x0.9x0.8 cm and had a sponge-like cut surface. The papillary structure was lined by both ciliated and nonciliated secretory cells, the same cellular structure as the salpinx. Areas with just a few mitoses and stratification of epithelial cells were noted, but invasion into the paratesticular tissue was absent, suggesting borderline malignancy. He is doing well after 5 months follow up. Prognosis of this scrotal tumor is thought to be better than the ovarian tumor of similar histology due to a better possibility of early detection.
Case Report
- Synchronous Invasive Ductal Carcinoma and Metastatic Ovarian Serous Papillary Adenocarcinoma in the Same Breast: A Case Report.
- Hyun Jung Kim, Sung jig Lim, Sehwan Han, Ji Young Kim, Kyeongmee Park
- Korean J Pathol. 2006;40(1):66-69.
- 2,294 View
- 18 Download
-
Abstract
PDF
- A 59-year-old woman displayed multiple palpable right breast masses along with ipsilateral cervical and axillary lymphadenopathy. She had a previous history of bilateral salpingo-oopho- rectomy for serous papillary adenocarcinoma two and half years ago. She underwent mastectomy for the lesions located in the upper inner breast quadrant. A 1 cm-sized primary ductal carcinoma was present; however, the other breast lesions and the metastatic axillary lymph nodes were confirmed as showing papillary serous adenocarcinoma, which were similar to the previous ovarian tumor. After the patient underwent postoperative adjuvant chemotherapy, of 8 cycles of doxorubicin and docetaxel, she has been stable during the clinical follow-up for 10 months with decreases in size of the metastatic nodules.
Original Articles
- Serous Cystadenoma of the Pancreas.
- Young Mee Cho, Gyung Yub Gong, Ghee Young Choe, Eun Sil Yu, In Chul Lee
- Korean J Pathol. 1994;28(5):522-527.
- 2,360 View
- 16 Download
-
Abstract
PDF
- Pathologists and others have been calling the serous cystadenoma of the pancreas "microcystic cystadenoma", following Compagno and Oertel's proposal in l978 because it usually consists of innumerable small cysts (less than 2cm). However, unilocular or predominantly macrocystic types of serous cystadenoma have been occasionally reported. Therefore, they present a difficulty in precise preoperative and intraoperative diagnosis for their simi1ar gross appearance to other cystic lesions of the pancreas. We discovered two cases of macrocystic and unilocular serous cystadenomas of the pancreas which were lined by cuboidal to flattened epithelial cells. They contained PAS positive and D-PAS negative intracytoplasmic glycogen granules. The unilocular, macrocystic and microcystic patterns may represent a morphologic spectrum of a pancreatic neoplasm. So we propose to use the term "serous cystadenoma" rather than microcystic cystadenoma.
- Distinction between Reactive Mesothelial and Carcinoma Cells in Serous Effusions by Mucin- and Immuno-cytochemical Panel .
- Byung Heon Kim
- J Pathol Transl Med. 1998;9(1):1-14.
- 4,010 View
- 107 Download
-
Abstract
PDF
- The cytologic distinction of carcinoma cells from reactive mesothelial cells can be difficult, especially in specimens containing abundant reactive mesothelial cells and inflammatory cells with scant carcinoma cells. This study evaluates the usefulness of mucin and immunocytochemistry for discrimination between reactive mesothelial cells and carcinoma cells, and sensitivity and specificity of these stains for the detection of metastatic carcinoma in serous effusions. Immunocytochemical panel including mucin cytochemistry with the periodic acid-Schiff(PAS) reaction after or without diastase digestion was undertaken on 127 serous effusion specimens with histologically confirmed diagnoses. The specimens including cell smears and cell blocks were stained with PAS and antibodies to carcinoembryonic antigen(CEA), epithelial membrane antigen(EMA), cytokeratin(CK), and vimentin. The sensitivities of these stains for metastatic carcinoma(127 cases) were 49%(46/94) in PAS, 48%(60/124) in CEA, 89%(97/109) in EMA, 88%(93/106) in CK, and 25%(20/81) in vimentin. The sensitivities of stains for reactive mesothelial cells(36 cases) were 19%(7/36) in EMA, 78%(28/36) in CK, and 75%(27/36) in vimentin. The PAS and CEA stains were not reacted with all cases of benign reactive serous effusions containing abundant reactive mesothelial cells. The specificities of stains for metastatic carcinoma(127 cases) were 100% in PAS, 100% in CEA, 81% in EMA, 22% in CK, and 25% in vimentin. The optimal combination of stains for use in a panel was PAS and CEA. Combined results from these two stains yielded an advanced sensitivity of 8% in PAS and 4% in CEA for metastatic carcinoma. EMA wasalso cosiderably useful for identification of carcinoma cells. CK and vimentin were not suitable for distinguishing between reactive mesothelial cells and carcinoma cells.
 First
First Prev
Prev


