 E-submission
E-submission
Search
- Page Path
- HOME > Search
- Primary Merkel cell carcinoma of the salivary gland: a clinicopathologic study of four cases with a review of literature
- Gyuheon Choi, Joon Seon Song, Hee Jin Lee, Gi Hwan Kim, Young Ho Jung, Yoon Se Lee, Kyung-Ja Cho
- J Pathol Transl Med. 2025;59(3):171-179. Published online April 30, 2025
- DOI: https://doi.org/10.4132/jptm.2025.03.25
- 5,401 View
- 166 Download
- 1 Crossref
-
 Abstract
Abstract
 PDF
PDF - Background
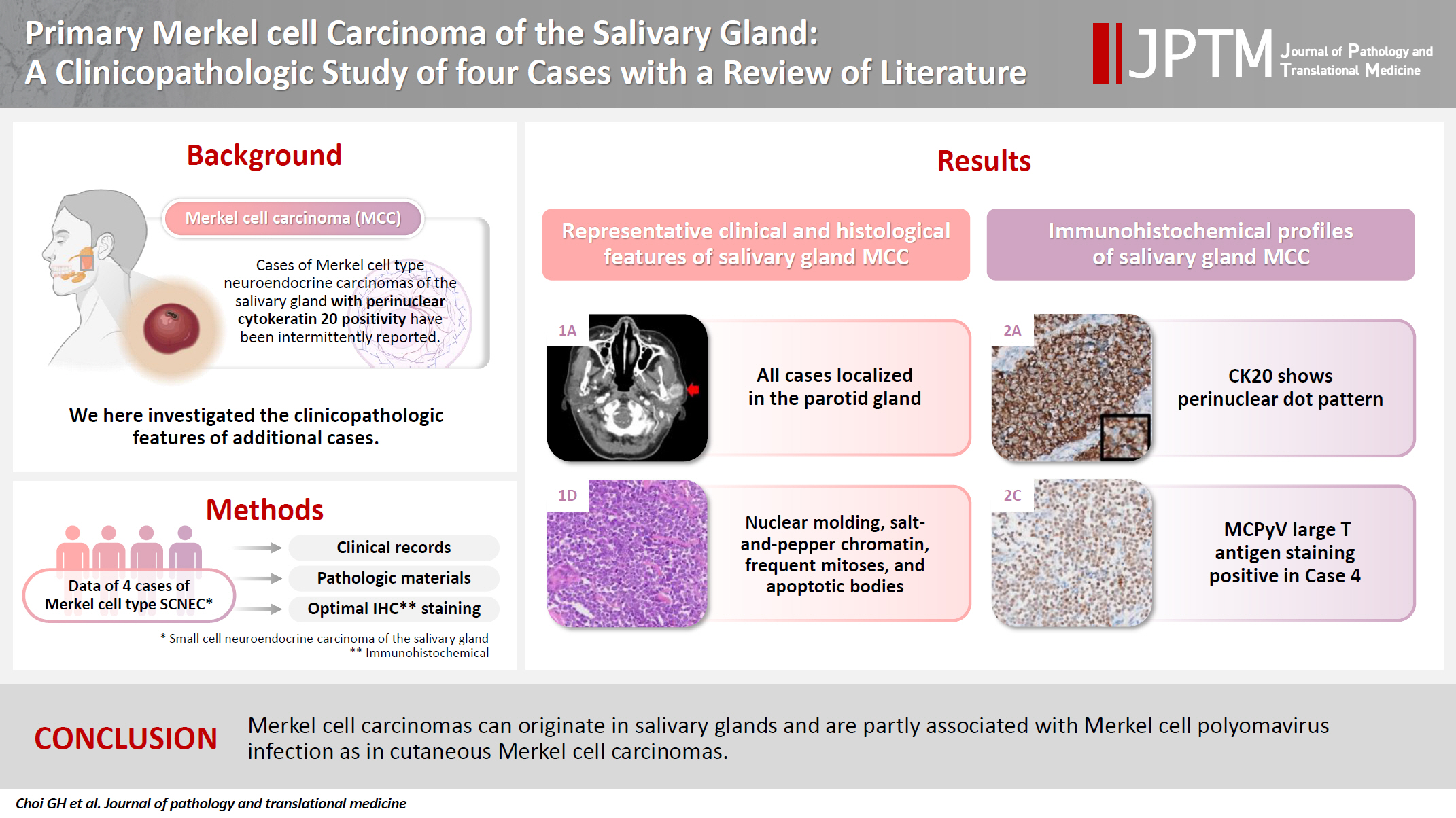
Primary Merkel cell carcinoma of the salivary gland is currently not listed in the World Health Organization classification. However, cases of Merkel cell type neuroendocrine carcinomas of the salivary gland with perinuclear cytokeratin 20 positivity have been intermittently reported. We here investigated the clinicopathologic features of additional cases.
Methods
Data of four cases of Merkel cell type small cell neuroendocrine carcinoma of the salivary gland were retrieved. To confirm the tumors’ primary nature, clinical records and pathologic materials were reviewed. Optimal immunohistochemical staining was performed to support the diagnosis.
Results
All tumors were located in the parotid gland. Possibilities of metastasis were excluded in all cases through a meticulous clinicopathological review. Tumor histology was consistent with the diagnosis of small cell neuroendocrine carcinoma. Tumors’ immunohistochemical phenotypes were consistent with Merkel cell carcinoma, including Merkel cell polyomavirus large T antigen positivity in two of the four cases.
Conclusions
Merkel cell carcinomas can originate in salivary glands and are partly associated with Merkel cell polyomavirus infection as in cutaneous Merkel cell carcinomas. -
Citations
Citations to this article as recorded by
- Parotid intranodal metastasis of Merkel cell carcinoma: a rare case report
Tong Gao, Dengshun Wang, Hongwei Yu, Yu’e Wang, Haibin Lu
BMC Oral Health.2025;[Epub] CrossRef
- Parotid intranodal metastasis of Merkel cell carcinoma: a rare case report
- Malignant potential of neuroendocrine microtumor of the pancreas harboring high-grade transformation: lesson learned from a patient with von Hippel-Lindau syndrome
- Jongwon Lee, Kyung Jin Lee, Dae Wook Hwang, Seung-Mo Hong
- J Pathol Transl Med. 2024;58(2):91-97. Published online March 13, 2024
- DOI: https://doi.org/10.4132/jptm.2024.02.13
- 6,213 View
- 223 Download
- 3 Web of Science
- 4 Crossref
-
Abstract
PDF
- Pancreatic neuroendocrine microtumor (PNEMT) is a neuroendocrine tumor (NET) < 0.5 cm in diameter, and it is considered benign. We report a PNEMT with high-grade transformation (HGT). A man in his 60s with von Hippel-Lindau syndrome underwent surgical resection of a NET. A second sub-centimeter nodule with a nodule-in-nodule pattern was discovered. The 0.4 cm outer nodule contained clear columnar cells with round nuclei and indistinct nucleoli, while the 0.1 cm inner nodule had eosinophilic cells with an increased nuclear to cytoplasmic ratio, vesicular nuclei, and prominent nucleoli. Tumor cells in the outer and inner nodules were synaptophysin and chromogranin positive. Only the inner nodule was p53 positive, while the outer nodule was exclusively positive for carbonic anhydrase 9 and vimentin. The Ki-67 labeling indices for the outer and inner nodules were 2.1% (grade 1) and 44.3% (grade 3), respectively. This nodule was determined to be a PNEMT with HGT. Our findings suggest that a PNEMT may not always be benign and can undergo HGT.
-
Citations
Citations to this article as recorded by- Intraductal papillary mucinous neoplasm unveiling incidental multifocal pancreatic neuroendocrine tumors: a challenging case report
Faten Limaiem, Mohamed Hajri, Nafaa Arfa
International Journal of Surgery Case Reports.2026; 138(5): 1634. CrossRef - Decoding Pancreatic Neuroendocrine Tumors: Molecular Profiles, Biomarkers, and Pathways to Personalized Therapy
Linda Galasso, Federica Vitale, Gabriele Giansanti, Giorgio Esposto, Raffaele Borriello, Irene Mignini, Alberto Nicoletti, Lorenzo Zileri Dal Verme, Antonio Gasbarrini, Maria Elena Ainora, Maria Assunta Zocco
International Journal of Molecular Sciences.2025; 26(16): 7814. CrossRef - Pancreatic neuroendocrine microtumors in the elderly: A retrospective study using cadaveric pancreatic tissue
Ting Yang, Ke Ren, Xiang-Quan Chen, Taku Toriumi, Yutaro Natsuyama, Jun Li, Aoi Sukeda, Toshitaka Nagao, Shuang-Qin Yi
World Journal of Gastrointestinal Oncology.2025;[Epub] CrossRef - Molecular Basis of Pancreatic Neuroendocrine Tumors
Alesia Maluchenko, Denis Maksimov, Zoia Antysheva, Julia Krupinova, Ekaterina Avsievich, Olga Glazova, Natalia Bodunova, Nikolay Karnaukhov, Ilia Feidorov, Diana Salimgereeva, Mark Voloshin, Pavel Volchkov
International Journal of Molecular Sciences.2024; 25(20): 11017. CrossRef
- Intraductal papillary mucinous neoplasm unveiling incidental multifocal pancreatic neuroendocrine tumors: a challenging case report
- Primary carcinoid tumor in the external auditory canal
- Dong Hae Chung, Gyu Cheol Han, Na Rae Kim
- J Pathol Transl Med. 2020;54(2):184-187. Published online November 13, 2019
- DOI: https://doi.org/10.4132/jptm.2019.11.07
- 10,526 View
- 167 Download
- 4 Web of Science
- 3 Crossref
-
Abstract
PDF
- A 39-year-old man visited the department of otolaryngology due to an ongoing hearing disturbance that had lasted for 1 year. Temporal bone computed tomography revealed soft tissue density nearly obliterating the left external auditory canal (EAC). The mass was composed of sheets of round tumor cells containing moderate amounts of fine granular cytoplasm and salt and pepper chromatin. Neither mitosis nor necrosis was found. The Ki-67 proliferation index was less than 2%. Cells were positive for CD56 and synaptophysin but negative for chromogranin, cytokeratin (CK) 20, and CK7. Based on these findings, the tumor was diagnosed as a carcinoid tumor, well differentiated neuroendocrine carcinoma, grade 1 (G1) according to current World Health Organization (WHO) classification of head and neck tumors; and a neuroendocrine tumor, G1 according to neuroendocrine neoplasm (NEN)-2018 WHO standard classification. He remained free of local recurrence and metastasis after 20 months of follow up. To date, only six cases of primary NENs in the EAC have been reported. Metastatic tumor should be included in the differential diagnoses. Because of its rarity, the prognosis and treatment have not yet been clarified.
-
Citations
Citations to this article as recorded by- First Report on a Rare Poorly Differentiated Neuroendocrine Tumour of the External Auditory Canal Involving Pinna
Akash Varshney, Amit Kumar Tyagi, Prashant Durgapal, Kajal Mahto, Akhilesh Chandra Yadav, Ankita Semwal
Indian Journal of Otolaryngology and Head & Neck Surgery.2025; 77(4): 1922. CrossRef - Incidental finding of a neuroendocrine neoplasm in a suspected ear canal exostosis
Alexander Wieck Fjaeldstad, Gerda Elisabeth Villadsen, Gitte Dam, Stephen Jacques Hamilton-Dutoit, Thomas Winther Frederiksen
Otolaryngology Case Reports.2022; 22: 100394. CrossRef - 68Ga-DOTATATE Uptake in Well-Differentiated Neuroendocrine Tumor of the External Auditory Canal
Özge Erol Fenercioğlu, Ediz Beyhan, Rahime Şahin, Mehmet Can Baloğlu, Tevfik Fikret Çermik
Clinical Nuclear Medicine.2022; 47(8): e552. CrossRef
- First Report on a Rare Poorly Differentiated Neuroendocrine Tumour of the External Auditory Canal Involving Pinna
- Combined Hepatocellular Carcinoma and Neuroendocrine Carcinoma with Ectopic Secretion of Parathyroid Hormone: A Case Report and Review of the Literature
- Hyun Jung Kwon, Ji-Won Kim, Haeryoung Kim, YoungRok Choi, Soomin Ahn
- J Pathol Transl Med. 2018;52(4):232-237. Published online May 25, 2018
- DOI: https://doi.org/10.4132/jptm.2018.05.17
- 10,029 View
- 160 Download
- 17 Web of Science
- 18 Crossref
-
Abstract
PDF
- Primary combined hepatocellular carcinoma (HCC) and neuroendocrine carcinoma is a rare entity, and so is hypercalcemia due to ectopic parathyroid hormone (PTH) secretion by tumor. A 44-year old man with hepatitis B virus associated chronic liver disease presented with a hepatic mass. Hemihepatectomy discovered the mass as combined HCC and poorly differentiated cholangiocarcinoma. During adjuvant chemoradiation therapy, he presented with nausea, and multiple systemic metastases were found. Laboratory tests revealed hypercalcemia with markedly elevated PTH and neuron specific enolase. Parathyroid scan showed normal uptake in parathyroid glands, suggestive of ectopic PTH secretion. Subsequently, immunohistochemistry of neuroendocrine marker was performed on the primary lesion, and confirmed the neuroendocrine differentiation in non-HCC component. The patient died 71 days after surgery. This report may suggest the possibility of ectopic PTH secretion by neuroendocrine carcinoma of hepatic origin causing hypercalcemia. Caution for neuroendocrine differentiation should be exercised when diagnosing poorly differentiated HCC.
-
Citations
Citations to this article as recorded by- Mixed glandular neuroendocrine carcinoma of the endometrium with hypercalcemic crisis
Mei Luo, Xiaoxia Yu, Zhongpei Chen, Zhenhan Li
The American Journal of the Medical Sciences.2025; 369(2): 281. CrossRef - Combined Neuroendocrine Carcinoma and Hepatocellular Carcinoma of the Liver: Systematic Literature Review Suggests Implementing Biological Characterization to Optimize Therapeutic Strategy
Daniela Sambataro, Sandro Bellavia, Paolo Di Mattia, Danilo Centonze, Carmela Emmanuele, Annalisa Bonasera, Giuseppe Caputo, Andrea Maria Onofrio Quattrocchi, Ernesto Vinci, Vittorio Gebbia, Maria Rosaria Valerio
Cancers.2025; 17(7): 1074. CrossRef - Surgical Resection of Primary Hepatic Mixed Neuroendocrine-Non-Neuroendocrine Neoplasm: A Report of Three Cases
Ryosuke Toyonaka, Osamu Aramaki, Nao Yoshida, Yusuke Mitsuka, Masanori Nakamura, Shu Inagaki, Kaiki Murai, Toshiyuki Ishige, Ryusuke Tsujimura, Sumie Ohni, Shinobu Masuda, Hiroharu Yamashita, Yukiyasu Okamura
The Japanese Journal of Gastroenterological Surgery.2025; 58(6): 331. CrossRef - Case report: mixed large-cell neuroendocrine and hepatocellular carcinoma of the liver
Xin Gao, Heng Wang, Zheyu Niu, Meng Liu, Xiaohan Kong, Hongrui Sun, Chaoqun Ma, Huaqiang Zhu, Jun Lu, Xu Zhou
Frontiers in Oncology.2024;[Epub] CrossRef - Mixed Primary Hepatocellular Carcinoma and Hepatic Neuroendocrine Carcinoma: Case Report and Literature Review
Woo Young Shin, Keon Young Lee, Kyeong Deok Kim
Medicina.2023; 59(2): 418. CrossRef - Comparison of Metastatic Patterns Among Neuroendocrine Tumors, Neuroendocrine Carcinomas, and Nonneuroendocrine Carcinomas of Various Primary Organs
Hyung Kyu Park, Ghee Young Kwon
Journal of Korean Medical Science.2023;[Epub] CrossRef - Immunohistochemical characterization of a steroid-secreting oncocytic adrenal carcinoma responsible for paraneoplastic hyperparathyroidism
Magalie Haissaguerre, Estelle Louiset, Christofer C Juhlin, Adam Stenman, Christophe Laurent, Hélène Trouette, Hervé Lefebvre, Antoine Tabarin
European Journal of Endocrinology.2023; 188(4): K11. CrossRef - A Case of a Rare Parathyroid Hormone (PTH)-Producing Neuroendocrine Tumor
Catherine Dianne Quinn, Fihr Chaudhary, Aron Gould-Simon, Baorong Chen, Harsimran Singh Bhandal, Uzair Chaudhary
American Journal of Case Reports.2022;[Epub] CrossRef - Neuroendocrine neoplasms of the biliary tree, liver and pancreas: a pathological approach
Claudio Luchini, Giuseppe Pelosi, Aldo Scarpa, Paola Mattiolo, Deborah Marchiori, Roberta Maragliano, Fausto Sessa, Silvia Uccella
Pathologica.2021; 113(1): 28. CrossRef - Contrast-Enhanced Ultrasound Findings of Hepatocellular Carcinoma With Neuroendocrine Carcinoma: A Case Report
Hong Wang, Dan Yang, Zhenru Wu, Yan Luo, Wenwu Ling
Frontiers in Medicine.2021;[Epub] CrossRef - Combined primary hepatic neuroendocrine carcinoma and hepatocellular carcinoma: case report and literature review
Akira Nakano, Kenichi Hirabayashi, Hiroshi Yamamuro, Taro Mashiko, Yoshihito Masuoka, Seiichiro Yamamoto, Soji Ozawa, Toshio Nakagohri
World Journal of Surgical Oncology.2021;[Epub] CrossRef - Hepatocellular carcinoma in patients with renal dysfunction: Pathophysiology, prognosis, and treatment challenges
Hsuan Yeh, Chung-Cheng Chiang, Tzung-Hai Yen
World Journal of Gastroenterology.2021; 27(26): 4104. CrossRef - Severe hypercalcaemia from ectopic intact parathyroid hormone secretion treated with continuous renal replacement therapy in a patient with two malignancies
Nathaniel Hocker, Maria Story, Alysa Lerud, Sarat Kuppachi
BMJ Case Reports.2021; 14(6): e242172. CrossRef - Parathyroid Carcinoma and Ectopic Secretion of Parathyroid hormone
Filomena Cetani, Elena Pardi, Claudio Marcocci
Endocrinology and Metabolism Clinics of North America.2021; 50(4): 683. CrossRef - Primary hepatic neuroendocrine cancer coexisted with hepatocellular carcinoma: a case report
Chikara Ebisutani, Seitetsu Yoon, Toshiki Hyodo, Takafumi Watanabe, Hirofumi Okada, Yutaka Shirakawa, Yoshio Sakamoto, Shigeya Hirohata
Kanzo.2020; 61(3): 122. CrossRef - Two-in-one: A pooled analysis of primary hepatic neuroendocrine carcinoma combined/collided with hepatocellular carcinoma
Jia-Xi Mao, Fei Teng, Ke-Yan Sun, Cong Liu, Guo-Shan Ding, Wen-Yuan Guo
Hepatobiliary & Pancreatic Diseases International.2020; 19(4): 399. CrossRef - Primary hepatic neuroendocrine carcinoma coexisting with distal cholangiocarcinoma
Qi Xin, Rong Lv, Cheng Lou, Zhe Ma, Gui-Qiu Liu, Qin Zhang, Hai-Bo Yu, Chuan-Shan Zhang
Medicine.2020; 99(26): e20854. CrossRef - Mixed hepatocellular carcinoma-neuroendocrine carcinoma—A diagnostic and therapeutic challenge
Nusrat Jahan, Irfan Warraich, Edwin Onkendi, Sanjay Awasthi
Current Problems in Cancer: Case Reports.2020; 1: 100020. CrossRef
- Mixed glandular neuroendocrine carcinoma of the endometrium with hypercalcemic crisis
- Multiple Neuroendocrine Tumors in Stomach and Duodenum in a Multiple Endocrine Neoplasia Type 1 Patient
- Bohyun Kim, Han-Kwang Yang, Woo Ho Kim
- J Pathol Transl Med. 2018;52(2):126-129. Published online December 21, 2017
- DOI: https://doi.org/10.4132/jptm.2017.09.16
- 10,304 View
- 145 Download
- 1 Web of Science
- 1 Crossref
-
Abstract
PDF
- A 67-year-old woman with a history of subtotal parathyroidectomy, distal pancreatectomy, and total splenectomy 23 years prior underwent surgical gastric resection for neuroendocrine tumors of the stomach and duodenum. Meticulous examination of the entire stomach and duodenum revealed multiple scattered, minute neuroendocrine tumors. To the best of our knowledge, this is the first case report of a patient diagnosed with gastroduodenal neuroendocrine tumors associated with multiple endocrine neoplasia type 1 (MEN 1) in whom complete histologic mapping of the whole gastrectomy specimen was performed. The presence of MEN 1–associated neuroendocrine tumors in the stomach is very rare, but should be considered in patients diagnosed with MEN 1 who present with a new tumor in the stomach.
-
Citations
Citations to this article as recorded by- A Case of Asymptomatic Multiple Endocrine Neoplasia Type I with Thymic Carcinoid
Suk Ki Park, Moon Won Lee, In Sub Han, Young Joo Park, Sung Yong Han, Joon Woo Park, Bong Eun Lee, Gwang Ha Kim, Sang Soo Kim
The Korean Journal of Helicobacter and Upper Gastrointestinal Research.2019; 19(1): 65. CrossRef
- A Case of Asymptomatic Multiple Endocrine Neoplasia Type I with Thymic Carcinoid
- Combined Adenosquamous and Large Cell Neuroendocrine Carcinoma of the Gallbladder
- Jiyoon Jung, Yang-Seok Chae, Chul Hwan Kim, Youngseok Lee, Jeong Hyeon Lee, Dong-Sik Kim, Young-Dong Yu, Joo Young Kim
- J Pathol Transl Med. 2018;52(2):121-125. Published online October 5, 2017
- DOI: https://doi.org/10.4132/jptm.2017.08.20
- 9,969 View
- 155 Download
- 12 Web of Science
- 10 Crossref
-
Abstract
PDF
- Large cell neuroendocrine carcinoma (LCNEC) of the gallbladder is extremely rare and usually combined with other type of malignancy, mostly adenocarcinoma. We report an unusual case of combined adenosquamous carcinoma and LCNEC of the gallbladder in a 54-year-old woman. A radical cholecystectomy specimen revealed a 4.3×4.0 cm polypoid mass in the fundus with infiltration of adjacent liver parenchyma. Microscopically, the tumor consisted of two distinct components. Adenosquamous carcinoma was predominant and abrupt transition from adenocarcinoma to squamous cell carcinoma was observed. LCNEC showed round cells with large, vesicular nuclei, abundant mitotic figures, and occasional pseudorosette formation. The patient received adjuvant chemotherapy. However, multiple liver metastases were identified at 3-month follow-up. Metastatic nodules were composed of LCNEC and squamous cell carcinoma components. Detecting LCNEC component is important in gallbladder cancer, because the tumor may require a different chemotherapy regimen and show early metastasis and poor prognosis.
-
Citations
Citations to this article as recorded by- Postoperative gastric cancer accompanied by large-cell neuroendocrine carcinoma: A case report
Zhiqin Chen, Jiang Liu, Jin Liu, Yinhang Wu, Jian Liu
Medicine.2025; 104(41): e44367. CrossRef - Does the size of the neuroendocrine-carcinoma component determine the prognosis of gallbladder cancer?
Ya-Fei Hu, Jun-Ke Wang, Wen-Jie Ma, Hai-Jie Hu, Han-Fei Gu, Fei Liu, Tian-Run Lv, Si-Qi Yang, Yu-Shi Dai, Rui-Qi Zou, Yan-Wen Jin, Fu-Yu Li
Frontiers in Endocrinology.2024;[Epub] CrossRef - Az epehólyag adenosquamosus daganata
Fanni Hegedűs, Anita Sejben
Orvosi Hetilap.2024; 165(49): 1945. CrossRef - Comparison of Metastatic Patterns Among Neuroendocrine Tumors, Neuroendocrine Carcinomas, and Nonneuroendocrine Carcinomas of Various Primary Organs
Hyung Kyu Park, Ghee Young Kwon
Journal of Korean Medical Science.2023;[Epub] CrossRef - Clinical features and outcomes analysis of Gallbladder neuroendocrine carcinoma
Man Jiang, Yijing Zhang
Journal of Cancer Research and Therapeutics.2023; 19(4): 910. CrossRef - Primary mixed large cell neuroendocrine carcinoma and adenocarcinoma of the gallbladder: A case report and literature review
Tingting Yu, Shike Li, Zhuo Zhang
Asian Journal of Surgery.2022; 45(11): 2336. CrossRef - Mixed neuroendocrine-non-neuroendocrine neoplasm of the gallbladder: case report and literature review
Xu Ren, Hong Jiang, Kan Sun, Xufu Qin, Yongping Qu, Tian Xia, Yan Chen
Diagnostic Pathology.2022;[Epub] CrossRef - Neuroendocrine Neoplasms of the Gallbladder: A Clinicopathological Analysis of 13 Patients and a Review of the Literature
Pengyan Wang, Jingci Chen, Ying Jiang, Congwei Jia, Junyi Pang, Shan Wang, Xiaoyan Chang, Oronzo Brunetti
Gastroenterology Research and Practice.2021; 2021: 1. CrossRef - Gallbladder Mixed Neuroendocrine-Non-neuroendocrine Neoplasm (MiNEN) Arising in Intracholecystic Papillary Neoplasm: Clinicopathologic and Molecular Analysis of a Case and Review of the Literature
Amedeo Sciarra, Edoardo Missiaglia, Mounir Trimech, Emmanuel Melloul, Jean-Philippe Brouland, Christine Sempoux, Stefano La Rosa
Endocrine Pathology.2020; 31(1): 84. CrossRef - Mixed neuroendocrine-non-neuroendocrine carcinoma of gallbladder: case report
Adam Skalický, Lucie Vištejnová, Magdaléna Dubová, Tomáš Malkus, Tomáš Skalický, Ondřej Troup
World Journal of Surgical Oncology.2019;[Epub] CrossRef
- Postoperative gastric cancer accompanied by large-cell neuroendocrine carcinoma: A case report
- Loss of Progesterone Receptor Expression Is an Early Tumorigenesis Event Associated with Tumor Progression and Shorter Survival in Pancreatic Neuroendocrine Tumor Patients
- Sung Joo Kim, Soyeon An, Jae Hoon Lee, Joo Young Kim, Ki-Byung Song, Dae Wook Hwang, Song Cheol Kim, Eunsil Yu, Seung-Mo Hong
- J Pathol Transl Med. 2017;51(4):388-395. Published online June 8, 2017
- DOI: https://doi.org/10.4132/jptm.2017.03.19
- 10,161 View
- 139 Download
- 21 Web of Science
- 21 Crossref
-
Abstract
PDF
- Background
Pancreatic neuroendocrine tumors (PanNETs) are the second most common pancreatic neoplasms and there is no well-elucidated biomarker to stratify their detection and prognosis. Previous studies have reported that progesterone receptor (PR) expression status was associated with poorer survival in PanNET patients.
Methods
To validate previous studies, PR protein expression was assessed in 21 neuroendocrine microadenomas and 277 PanNETs and compared with clinicopathologic factors including patient survival.
Results
PR expression was gradually decreased from normal islets (49/49 cases, 100%) to neuroendocrine microadenoma (14/21, 66.6%) to PanNETs (60/277, 21.3%; p < .001). PanNETs with loss of PR expression were associated with increased tumor size (p < .001), World Health Organization grade (p = .001), pT classification (p < .001), perineural invasion (p = .028), lymph node metastasis (p = .004), activation of alternative lengthening of telomeres (p = .005), other peptide hormonal expression (p < .001) and ATRX/DAXX expression (p = .015). PanNET patients with loss of PR expression (5-year survival rate, 64.1%) had significantly poorer recurrence-free survival outcomes than those with intact PR expression (90%) by univariate (p = .012) but not multivariate analyses. Similarly, PanNET patients with PR expression loss (5-year survival rate, 76%) had significantly poorer overall survival by univariate (p = .015) but not multivariate analyses.
Conclusions
Loss of PR expression was noted in neuroendocrine microadenomas and was observed in the majority of PanNETs. This was associated with increased grade, tumor size, and advanced pT and pN classification; and was correlated with decreased patient survival time by univariate but not multivariate analyses. Loss of PR expression can provide additional information on shorter disease-free survival in PanNET patients. -
Citations
Citations to this article as recorded by- Sexual dimorphism and estrogens in neuroendocrine neoplasms
Magdalena Strachowska, Damian Jacenik
Biochimica et Biophysica Acta (BBA) - Reviews on Cancer.2026; 1881(4): 189613. CrossRef - Low Expression of Cell Adhesion Molecule 1 in Resected Gastroenteropancreatic Neuroendocrine Tumors: Relationship With Lymph Node and Distant Metastasis
Ken Miyabe, Michinobu Umakoshi, Yukitsugu Kudo‐Asabe, Kei Koyama, Takahiro Ishinari, Ayana Takahashi, Hikaru Tsukita, Yukinobu Ito, Makoto Yoshida, Masato Takahashi, Tatsuo Sugiyama, Masato Sageshima, Hiroshi Nanjo, Yoshinori Murakami, Akiteru Goto
Pathology International.2026;[Epub] CrossRef - Female sex is associated with improved outcomes after surgery for pancreatic neuroendocrine neoplasms
Fabiola A. Bechtiger, Jörg Kaiser, Ingmar F. Rompen, Ulf Hinz, Magdalena Lewosinska, Carl-Stephan Leonhardt, Mohammed Al-Saeedi, Martin Loos, Markus W. Büchler, Thomas Hank
European Journal of Surgical Oncology.2026; 52(8): 111954. CrossRef - Incidence and Prognostic Implications of Lymphovascular Invasion in Node‐Negative Pancreatic Neuroendocrine Tumors: Results From the US Neuroendocrine Study Group
Kota Sahara, Diamantis I. Tsilimigras, Yuki Homma, Jun Kawashima, Shishir K. Maithel, Flavio Rocha, Sharon Weber, Ryan Fields, Kamran Idrees, George A. Poultsides, Cliff Cho, Itaru Endo, Timothy M. Pawlik
Journal of Surgical Oncology.2025; 131(3): 465. CrossRef - Impact of sex hormones on development and progression in NEN: a new therapeutic target?
Roberta Modica, Alessia Liccardi, Elena Zago, Nevena Mikovic, Franz Sesti, Sofia Ballarini, Renata Simona Auriemma, Annamaria Colao
Endocrine-Related Cancer.2025;[Epub] CrossRef - Sex Differences in the Survival of Patients with Neuroendocrine Neoplasms: A Comparative Study of Two National Databases
Mohamed Mortagy, Marie Line El Asmar, Kandiah Chandrakumaran, John Ramage
Cancers.2024; 16(13): 2376. CrossRef - Association Between Female Sex and Better Survival in Gastroenteropancreatic Neuroendocrine Tumors
Jeremy Chang, Mohammed O. Suraju, Catherine G. Tran, Carlos H.F. Chan, Po Hien Ear, James R. Howe, Scott K. Sherman
Journal of Surgical Research.2024; 302: 53. CrossRef - Venous invasion and lymphatic invasion are correlated with the postoperative prognosis of pancreatic neuroendocrine neoplasm
Sho Kiritani, Junichi Arita, Yuichiro Mihara, Rihito Nagata, Akihiko Ichida, Yoshikuni Kawaguchi, Takeaki Ishizawa, Nobuhisa Akamatsu, Junichi Kaneko, Kiyoshi Hasegawa
Surgery.2023; 173(2): 365. CrossRef - Combined Infiltrative Macroscopic Growth Pattern and Infiltrative Microscopic Tumor Border Status Is a Novel Surrogate Marker of Poor Prognosis in Patients With Pancreatic Neuroendocrine Tumor
Bokyung Ahn, Joo Young Kim, Seung-Mo Hong
Archives of Pathology & Laboratory Medicine.2023; 147(1): 100. CrossRef - HORMONET: a phase II trial of tamoxifen for estrogen/progesterone receptor-positive neuroendocrine tumors
Milton J. Barros, Jonathan Strosberg, Taymeyah Al-Toubah, Victor Hugo F. de Jesus, Lais Durant, Celso A. Mello, Tiago C. Felismino, Louise De Brot, Rodrigo G. Taboada, Mauro D. Donadio, Rachel P. Riechelmann
Therapeutic Advances in Medical Oncology.2023;[Epub] CrossRef - Diagnostic and Prognostic Impact of Progesterone Receptor Immunohistochemistry: A Study Evaluating More Than 16,000 Tumors
Florian Viehweger, Lisa-Marie Tinger, David Dum, Natalia Gorbokon, Anne Menz, Ria Uhlig, Franziska Büscheck, Andreas M. Luebke, Claudia Hube-Magg, Andrea Hinsch, Doris Höflmayer, Christoph Fraune, Patrick Lebok, Sören Weidemann, Maximilian Lennartz, Frank
Analytical Cellular Pathology.2022; 2022: 1. CrossRef - Prognostic Nomograms to Predict Overall Survival and Cancer-Specific Survival of Patients With Pancreatic Neuroendocrine Tumors
Zuoli Song, Sumei Wang, Yujing Wu, Jinjuan Zhang, Shuye Liu
Pancreas.2021; 50(3): 414. CrossRef - Pancreatic High-Grade Neuroendocrine Neoplasms in the Korean Population: A Multicenter Study
Haeryoung Kim, Soyeon An, Kyoungbun Lee, Sangjeong Ahn, Do Youn Park, Jo-Heon Kim, Dong-Wook Kang, Min-Ju Kim, Mee Soo Chang, Eun Sun Jung, Joon Mee Kim, Yoon Jung Choi, So-Young Jin, Hee Kyung Chang, Mee-Yon Cho, Yun Kyung Kang, Myunghee Kang, Soomin Ahn
Cancer Research and Treatment.2020; 52(1): 263. CrossRef - Systemic distribution of progesterone receptor subtypes in human tissues
Teeranut Asavasupreechar, Ryoko Saito, Yasuhiro Miki, Dean P. Edwards, Viroj Boonyaratanakornkit, Hironobu Sasano
The Journal of Steroid Biochemistry and Molecular Biology.2020; 199: 105599. CrossRef - Progesteron receptor expression in insulin producing cells of neuroendocrine neoplasms
Tomoyoshi Tachibana, Atsuko Kasajima, Takeshi Aoki, Tomoaki Tabata, Keely McNamara, Samaneh Yazdani, Sato Satoko, Fumiyoshi Fujishima, Fuyuhiko Motoi, Michiaki Unno, Hironobu Sasano
The Journal of Steroid Biochemistry and Molecular Biology.2020; 201: 105694. CrossRef - Prognostic and predictive factors on overall survival and surgical outcomes in pancreatic neuroendocrine tumors: recent advances and controversies
Lingaku Lee, Tetsuhide Ito, Robert T Jensen
Expert Review of Anticancer Therapy.2019; 19(12): 1029. CrossRef - Immunohistochemistry, carcinomas of unknown primary, and incidence rates
Edward B. Stelow, Hadi Yaziji
Seminars in Diagnostic Pathology.2018; 35(2): 143. CrossRef - Carbonic anhydrase 9 expression in well-differentiated pancreatic neuroendocrine neoplasms might be associated with aggressive behavior and poor survival
Joo Young Kim, Sang Hwa Lee, Soyeon An, Sung Joo Kim, You-Na Sung, Ki-Byung Song, Dae Wook Hwang, Song Cheol Kim, Seung-Mo Hong
Virchows Archiv.2018; 472(5): 739. CrossRef - Prognostic value of progesterone receptor in solid pseudopapillary neoplasm of the pancreas: evaluation of a pooled case series
Feiyang Wang, Zibo Meng, Shoukang Li, Yushun Zhang, Heshui Wu
BMC Gastroenterology.2018;[Epub] CrossRef - Estrogens modulate progesterone receptor expression and may contribute to progesterone-mediated apoptotic β-cell death
Viviane Abreu Nunes
Endocrinology&Metabolism International Journal.2018;[Epub] CrossRef - Diagnostic and prognostic significance of immunohistochemistry in pancreatic tumors
Mohebat H. Gouda, Rasha M. El-Sawy, Gehan M. Elosaily
Egyptian Journal of Pathology.2018; 38(2): 311. CrossRef
- Sexual dimorphism and estrogens in neuroendocrine neoplasms
- Neuroendocrine Tumors of the Female Reproductive Tract: A Literature Review
- Yi Kyeong Chun
- J Pathol Transl Med. 2015;49(6):450-461. Published online October 13, 2015
- DOI: https://doi.org/10.4132/jptm.2015.09.20
- 21,471 View
- 286 Download
- 29 Web of Science
- 30 Crossref
-
Abstract
PDF
- Neuroendocrine tumors of the female reproductive tract are a heterogeneous group of neoplasms that display various histologic findings and biologic behaviors. In this review, the classification and clinicopathologic characteristics of neuroendocrine tumors of the female reproductive tract are described. Differential diagnoses are discussed, especially for non-neuroendocrine tumors showing high-grade nuclei with neuroendocrine differentiation. This review also discusses recent advances in our pathogenetic understanding of these disorders.
-
Citations
Citations to this article as recorded by- Mixed neuroendocrine-non-neuroendocrine neoplasm (MiNEN) of the cervix in a 38-year-old female: a case report and review of literature
Josh Matthew B. Chen, Denise B. Andal, Benedict Jose P. Canora, Claire Anne Therese M. Hemedez
Human Pathology Reports.2026; 43: 300815. CrossRef - Neuroendocrine Neoplasms of the Gastrointestinal Tract: Morphology, WHO 2022 Grading, and Prognostic Perspectives
Hussein Qasim, Shaima' Dibian, Mohammad Abu Shugaer, Karis Khattab, Mudhaffer Touqan, Matteo Luigi Giuseppe Leoni , Giustino Varrassi
Cureus.2026;[Epub] CrossRef - When Immunophenotype Is Not Identity: A Clinicopathological Review of Neuroendocrine Differentiation in Tumors of the Female Genital Tract
Catalin-Bogdan Satala, Alina-Mihaela Gurau, Gabriela Patrichi, Roxana-Cristina Mehedinti, Andy Radu Leibovici, Gabriela Gurau
Diagnostics.2026; 16(10): 1573. CrossRef - A rare case report of primary ovarian carcinoid presenting with constipation
Xiaofeng Deng, Qian Huang, Bangfang Xie, Hailong Huang, Jianguo Chen
Frontiers in Oncology.2025;[Epub] CrossRef - Clinical, pathological characteristics, and therapeutic outcomes of primary ovarian carcinoid tumors: a case series of 15 cases
Xinyue Dai, Suidan Chen, Simeng Yang
World Journal of Surgical Oncology.2025;[Epub] CrossRef - Smart Red Blood Cell Carriers: A Nanotechnological Approach to Cancer Drug Delivery
Ioannis Tsamesidis, Georgios Dryllis, Sotirios P. Fortis, Andreas Sphicas, Vasiliki Konstantinidou, Maria Chatzidimitriou, Stella Mitka, Maria Trapali, Petros Skepastianos, Anastasios G. Kriebardis, Ilias Pessach
Current Issues in Molecular Biology.2025; 47(9): 711. CrossRef - Imaging of Gynecologic Neuroendocrine Tumors: A Case-Based Pictorial Essay
Ana Paula Bavaresco, Ulysses S. Torres, Mayara S. Cruz, Vitor V.C. Machado, Cynthia L.P. Borborema, Giovanna S. Torre, Jhonata Soares Da Silva, Tulio A. Kawai, Gustavo R.A. Focchi, Eduardo O. Pacheco, Aley Talans, Daniel Bekhor, Ana Paula C. Moura, Lucas
Seminars in Ultrasound, CT and MRI.2025;[Epub] CrossRef - Challenges in Diagnosis and Management of Ovarian Neuroendocrine Carcinoma: A Case of Aggressive Disease With Multimodal Treatment Approach
Javeria Haider, Humera Mahmood, Muhammad Faheem, Shaista Khurshid, Abdullah, Biruk Demisse Ayalew, Humza Saeed
Clinical Case Reports.2025;[Epub] CrossRef - Neuroendocrine Marker Expression in Primary Non-neuroendocrine Epithelial Tumors of the Ovary: A Study of 551 Cases
Michaela Kendall Bártů, Kristýna Němejcová, Romana Michálková, Quang Hiep Bui, Jana Drozenová, Pavel Fabian, Oluwole Fadare, Jitka Hausnerová, Jan Laco, Radoslav Matěj, Gábor Méhes, Adam Šafanda, Naveena Singh, Petr Škapa, Zuzana Špůrková, Simona Stolnicu
International Journal of Gynecological Pathology.2024; 43(2): 123. CrossRef - Diagnostic and therapeutic challenge of neuroendocrine endometrial carcinoma: a case report
Hariyono Winarto, David Calvin, Fitriyadi Kusuma, Kartiwa Hadi Nuryanto, Yuri Feharsal, Dewita Nilasari, Hartono Tjahjadi
The Pan African Medical Journal.2024;[Epub] CrossRef - Neuroendocrine carcinoma of ovary: Hitherto rare entity in primary ovarian tumors
Md A. Osama, Seema Rao, Punita Bhardwaj, Geeta Mediratta, Sunita Bhalla, Sonia Badwal
Indian Journal of Pathology and Microbiology.2023; 66(4): 855. CrossRef - Mixed neuroendocrine–non-neuroendocrine neoplasm with mucinous adenocarcinoma and amphicrine carcinoma components in the bile duct: an autopsy case
Toji Murabayashi, Yoshihide Kanno, Takashi Odaira, Shinsuke Koshita, Takahisa Ogawa, Hiroaki Kusunose, Toshitaka Sakai, Keisuke Yonamine, Kazuaki Miyamoto, Fumisato Kozakai, Kazuki Endo, Yutaka Noda, Takashi Sawai, Kei Ito
Clinical Journal of Gastroenterology.2023; 16(2): 310. CrossRef - Coexistence of Papillary Thyroid Carcinoma and Strumal Carcinoid Arising from Struma Ovarii in Pregnant Women: a Case Report and Review
Myungsoo Im, Doohwa Kim, Soree Ryang, Bo Hyun Kim
International Journal of Thyroidology.2023; 16(1): 134. CrossRef - Role of radiotherapy in the management of rare gynaecological cancers
R. Morcet-Delattre, S. Espenel, P. Tas, C. Chargari, A. Escande
Cancer/Radiothérapie.2023; 27(8): 778. CrossRef - Small cell carcinoma of the ovary, pulmonary type: A role for adjuvant radiotherapy after carboplatin and etoposide?
Anase S. Asom, Ricardo R. Lastra, Yasmin Hasan, Lori Weinberg, Gini F. Fleming, Katherine C. Kurnit
Gynecologic Oncology Reports.2022; 39: 100925. CrossRef - MicroRNA and Metabolic Profiling of a Primary Ovarian Neuroendocrine Carcinoma Pulmonary-Type Reveals a High Degree of Similarity with Small Cell Lung Cancer
Stefano Miglietta, Giulia Girolimetti, Lorena Marchio, Manuela Sollazzo, Noemi Laprovitera, Sara Coluccelli, Dario De Biase, Antonio De Leo, Donatella Santini, Ivana Kurelac, Luisa Iommarini, Anna Ghelli, Davide Campana, Manuela Ferracin, Anna Myriam Perr
Non-Coding RNA.2022; 8(5): 64. CrossRef - Neuroendocrine Carcinomas of the Uterine Cervix, Endometrium, and Ovary Show Higher Tendencies for Bone, Brain, and Liver Organotrophic Metastases
Hyung Kyu Park
Current Oncology.2022; 29(10): 7461. CrossRef - Uterine carcinoma admixed with neuroendocrine carcinoma
Maria Victoria Olinca, Anca Potecă, Elvira Brătilă, Mihai Mitran
Ginecologia.ro.2022; 4(38): 32. CrossRef - The puzzle of gynecologic neuroendocrine carcinomas: State of the art and future directions
Giuseppe Caruso, Carolina Maria Sassu, Federica Tomao, Violante Di Donato, Giorgia Perniola, Margherita Fischetti, Pierluigi Benedetti Panici, Innocenza Palaia
Critical Reviews in Oncology/Hematology.2021; 162: 103344. CrossRef - Pitfalls and challenges in managing neuroendocrine carcinoma of gynecological origin: A case series and brief review
Lauren E. Farmer, Rutmi U. Goradia, Nisha A. Lakhi
Clinical Case Reports.2021;[Epub] CrossRef - Primary mixed large cell neuroendocrine and high grade serous carcinoma of the endometrium
Liesel Elisabeth Hardy, Zia Chaudry, King Wan, Chloe Ayres
BMJ Case Reports.2020; 13(9): e234977. CrossRef - Neuroendocrine carcinoma of the endometrium: Disease course, treatment, and outcomes
Kathryn Schlechtweg, Ling Chen, Caryn M. St. Clair, Ana I. Tergas, Fady Khoury-Collado, June Y. Hou, Alexander Melamed, Alfred I. Neugut, Dawn L. Hershman, Jason D. Wright
Gynecologic Oncology.2019; 155(2): 254. CrossRef - Peritoneal Fluid Cytology of Disseminated Large Cell Neuroendocrine Carcinoma Combined with Endometrioid Adenocarcinoma of the Endometrium
Yong-Moon Lee, Min-Kyung Yeo, Song-Yi Choi, Kyung-Hee Kim, Kwang-Sun Suh
Journal of Pathology and Translational Medicine.2019; 53(6): 407. CrossRef - Pro-Gastrin Releasing Peptide: A New Serum Marker for Endometrioid Adenocarcinoma
Mine Kiseli, Gamze Sinem Caglar, Asli Yarci Gursoy, Tolga Tasci, Tuba Candar, Egemen Akincioglu, Emre Goksan Pabuccu, Nurettin Boran, Gokhan Tulunay, Haldun Umudum
Gynecologic and Obstetric Investigation.2018; 83(6): 540. CrossRef - Tumeur neuroendocrine à petite cellule de l’endomètre : prise en charge originale
E. Galmiche, N. Hudry, P. Sagot, P. Ginod, S. Douvier
Gynécologie Obstétrique Fertilité & Sénologie .2017; 45(6): 381. CrossRef - Twist on a classic: vitamin D and hypercalcaemia of malignancy
Juan C Osorio, Masha G Jones, Nina Schatz-Siemers, Stephanie J Tang
BMJ Case Reports.2017; 2017: bcr-2017-220819. CrossRef - Mixed Neuroendocrine-Nonneuroendocrine Neoplasms (MiNENs): Unifying the Concept of a Heterogeneous Group of Neoplasms
Stefano La Rosa, Fausto Sessa, Silvia Uccella
Endocrine Pathology.2016; 27(4): 284. CrossRef - Neuroendocrine tumours in rare sites: differences in nomenclature and diagnostics—a rare and ubiquitous histotype
Elia Guadagno, Gaetano De Rosa, Marialaura Del Basso De Caro
Journal of Clinical Pathology.2016; 69(7): 563. CrossRef - Primary ovarian neuroendocrine tumor arising in association with a mature cystic teratoma: A case report
Nicolas M. Orsi, Mini Menon
Gynecologic Oncology Reports.2016; 17: 83. CrossRef - Benign Endometrial Polyp and Primary Endometrial Small Cell Neuroendocrine Carcinoma Confined to the Polyp: A Rare Association
Pembe Oltulu, Ceyhan Uğurluoğlu, Ayşenur Uğur, Sıdıka Fındık, Lema Tavlı
Journal of Clinical and Experimental Investigations.2016;[Epub] CrossRef
- Mixed neuroendocrine-non-neuroendocrine neoplasm (MiNEN) of the cervix in a 38-year-old female: a case report and review of literature
- Clinical and Prognostic Significances of Cytokeratin 19 and KIT Expression in Surgically Resectable Pancreatic Neuroendocrine Tumors
- Eun-Mi Son, Joo Young Kim, Soyeon An, Ki-Byung Song, Song Cheol Kim, Eunsil Yu, Seung-Mo Hong
- J Pathol Transl Med. 2015;49(1):30-36. Published online January 15, 2015
- DOI: https://doi.org/10.4132/jptm.2014.10.23
- 14,414 View
- 103 Download
- 22 Web of Science
- 21 Crossref
-
Abstract
PDF
- Background
Pancreatic neuroendocrine tumors (PanNETs) are malignant endocrine neoplasms that present diverse clinical behaviors. Therefore, identification of biomarkers of PanNETs is important for stratification of the prognosis of PanNET patients. Recently, cytokeratin 19 (CK19) and KIT expression were reported to have prognostic significance in PanNET patients. Methods: To identify their prognostic significance, CK19 and KIT protein expression were assessed in 182 surgically resected PanNETs and compared with clinicopathologic factors. Results: Of 182 PanNETs cases, CK19 and KIT expression was noted in 97 (53.3%) and 16 (8.8%) cases, respectively. PanNET patients with CK19 expression had larger tumors (p=.006), higher World Health Organization (WHO) grade (p=.002) and pT classification (p<.001), increased distant metastasis (p=.004), and lymphovascular (p=.012) and perineural (p=.019) invasion. Similarly, those with KIT expression had larger tumors (p=.030), higher WHO grade (p=.001), advanced pT classification (p<.001), distant metastasis (p=.001), and lymphovascular invasion (p=.014). The 5-year survival rate for PanNET patients with KIT expression was significantly lower (62%) than that of patients without KIT expression (77%, p=.011), as determined by univariate but not by multivariate analyses. Conclusions: CK19 and KIT expression correlate with higher metastatic potential and advanced disease stage, and KIT expression is associated with worse survival in PanNET patients. -
Citations
Citations to this article as recorded by- Case Report: Extra-adrenal retroperitoneal paraganglioma in a young adult cat diagnosed by imaging, pathology, and immunohistochemistry
Sang-June Sohn, Sohee Lim, Junghoon Park, Ulsoo Choi, Yeon-Jung Hong
Frontiers in Veterinary Science.2025;[Epub] CrossRef - Appendiceal mucinous tumour resulting in autoamputation of the appendix: A case report and literature review
Chenao Wang, Yufeng Liu, Yaqing Liu, Baicheng Li, Xingdong Hou, Bowei Lu, Zhao Chen, Shili Ning
Experimental and Therapeutic Medicine.2025; 31(2): 1. CrossRef - Expression profiles of cadherin 17 and claudin 18.2 in comparison with peptide hormonal expression in pancreatic neuroendocrine tumours: Implications for targeted immunotherapy
Kahoko Maeda, Takeshi Uehara, Waki Hosoda, Yasuhiro Kuraishi, Hiroyoshi Ota
Pathology - Research and Practice.2024; 262: 155537. CrossRef - Glypican-3 and Cytokeratin-19 Expression in Pancreatic Cancer in a Canadian Population
Carley Bekkers, Ravi Ramjeesingh, Thomas Arnason
Journal of Clinical Medicine.2024; 13(22): 6893. CrossRef - Combined Infiltrative Macroscopic Growth Pattern and Infiltrative Microscopic Tumor Border Status Is a Novel Surrogate Marker of Poor Prognosis in Patients With Pancreatic Neuroendocrine Tumor
Bokyung Ahn, Joo Young Kim, Seung-Mo Hong
Archives of Pathology & Laboratory Medicine.2023; 147(1): 100. CrossRef -
Tumor-associated nonmyelinating Schwann cell–expressed
PVT1
promotes pancreatic cancer kynurenine pathway and tumor immune exclusion
Chengcao Sun, Youqiong Ye, Zhi Tan, Yuan Liu, Yajuan Li, Wei Hu, Ke Liang, Sergey D. Egranov, Lisa Angela Huang, Zhao Zhang, Yaohua Zhang, Jun Yao, Tina K. Nguyen, Zilong Zhao, Andrew Wu, Jeffrey R. Marks, Abigail S. Caudle, Aysegul A. Sahin, Jianjun Gao,
Science Advances.2023;[Epub] CrossRef - Diagnostic and prognostic impact of cytokeratin 19 expression analysis in human tumors: a tissue microarray study of 13,172 tumors
Anne Menz, Rifka Bauer, Martina Kluth, Clara Marie von Bargen, Natalia Gorbokon, Florian Viehweger, Maximilian Lennartz, Cosima Völkl, Christoph Fraune, Ria Uhlig, Claudia Hube-Magg, Noémi De Wispelaere, Sarah Minner, Guido Sauter, Simon Kind, Ronald Simo
Human Pathology.2021; 115: 19. CrossRef - The molecular biology of pancreatic neuroendocrine neoplasms: Challenges and translational opportunities
Kate Young, Naureen Starling, Anguraj Sadanandam
Seminars in Cancer Biology.2020; 61: 132. CrossRef - Pancreatic acinar cell carcinomas and mixed acinar-neuroendocrine carcinomas are more clinically aggressive than grade 1 pancreatic neuroendocrine tumours
Joo Young Kim, Jacqueline A. Brosnan-Cashman, Jiyoon Kim, Soyeon An, Kyoung-Bun Lee, Haeryoung Kim, Do Youn Park, Kee-Taek Jang, Young-Ha Oh, Ralph H. Hruban, Christopher M. Heaphy, Seung-Mo Hong
Pathology.2020; 52(3): 336. CrossRef - Morphologic Variants of Pancreatic Neuroendocrine Tumors: Clinicopathologic Analysis and Prognostic Stratification
Yue Xue, Michelle D. Reid, Burcin Pehlivanoglu, Rebecca C. Obeng, Hongmei Jiang, Bahar Memis, Shu K. Lui, Juan Sarmiento, David Kooby, Shishir K. Maithel, Bassel El-Rayes, Olca Basturk, Volkan Adsay
Endocrine Pathology.2020; 31(3): 239. CrossRef - Histological grades and prognostic markers of well-differentiated pancreatic neuroendocrine tumor (WDPNET)
Yongchao Li, Daniel Rowan, Claire P. Williamson, Meiyun Fan, Ali G. Saad, Lizhi Zhang
Journal of Pancreatology.2020; 3(4): 188. CrossRef - Clinical and histopathologic prognostic implications of the expression of cytokeratins 8, 10, 13, 14, 16, 18 and 19 in oral and oropharyngeal squamous cell carcinoma
Rima A. Safadi, Niveen I. Abdullah, Rolla F. Alaaraj, Dima H. Bader, Darshan D. Divakar, Abed A. Hamasha, Maher A. Sughayer
Archives of Oral Biology.2019; 99: 1. CrossRef - Prognostic and predictive factors on overall survival and surgical outcomes in pancreatic neuroendocrine tumors: recent advances and controversies
Lingaku Lee, Tetsuhide Ito, Robert T Jensen
Expert Review of Anticancer Therapy.2019; 19(12): 1029. CrossRef - Carbonic anhydrase 9 expression in well-differentiated pancreatic neuroendocrine neoplasms might be associated with aggressive behavior and poor survival
Joo Young Kim, Sang Hwa Lee, Soyeon An, Sung Joo Kim, You-Na Sung, Ki-Byung Song, Dae Wook Hwang, Song Cheol Kim, Seung-Mo Hong
Virchows Archiv.2018; 472(5): 739. CrossRef - CD133 expression in well-differentiated pancreatic neuroendocrine tumors: a potential predictor of progressive clinical courses
Yasuhiro Sakai, Seung-Mo Hong, Soyeon An, Joo Young Kim, Denis Corbeil, Jana Karbanová, Kyoko Otani, Kohei Fujikura, Ki-Byung Song, Song Cheol Kim, Masayuki Akita, Yoshihide Nanno, Hirochika Toyama, Takumi Fukumoto, Yonson Ku, Takanori Hirose, Tomoo Itoh,
Human Pathology.2017; 61: 148. CrossRef - Prognostic and predictive biomarkers in neuroendocrine tumours
David L. Chan, Stephen J. Clarke, Connie I. Diakos, Paul J. Roach, Dale L. Bailey, Simron Singh, Nick Pavlakis
Critical Reviews in Oncology/Hematology.2017; 113: 268. CrossRef - Loss of Progesterone Receptor Expression Is an Early Tumorigenesis Event Associated with Tumor Progression and Shorter Survival in Pancreatic Neuroendocrine Tumor Patients
Sung Joo Kim, Soyeon An, Jae Hoon Lee, Joo Young Kim, Ki-Byung Song, Dae Wook Hwang, Song Cheol Kim, Eunsil Yu, Seung-Mo Hong
Journal of Pathology and Translational Medicine.2017; 51(4): 388. CrossRef - Prognostic significance of cytokeratin 19 expression in pancreatic neuroendocrine tumor: A meta-analysis
Dong Cen, Jiang Chen, Zheyong Li, Jie Zhao, Xiujun Cai, Aamir Ahmad
PLOS ONE.2017; 12(11): e0187588. CrossRef - A retrospective cohort study of pancreatic neuroendocrine tumors at single institution over 15 years: New proposal for low- and high-grade groups, validation of a nomogram for prognosis, and novel follow-up strategy for liver metastases
Liangtao Ye, Huilin Ye, Quanbo Zhou, Zhihua Li, Qing Lin, Langping Tan, Wenchao Gao, Zhiqiang Fu, Shangyou Zheng, Rufu Chen
International Journal of Surgery.2016; 29: 108. CrossRef - Correlating and Combining Genomic and Proteomic Assessment withIn VivoMolecular Functional Imaging: Will This Be the Future Roadmap for Personalized Cancer Management?
Bhakti Basu, Sandip Basu
Cancer Biotherapy and Radiopharmaceuticals.2016; 31(3): 75. CrossRef - Recent Updates on Neuroendocrine Tumors From the Gastrointestinal and Pancreatobiliary Tracts
Joo Young Kim, Seung-Mo Hong
Archives of Pathology & Laboratory Medicine.2016; 140(5): 437. CrossRef
- Case Report: Extra-adrenal retroperitoneal paraganglioma in a young adult cat diagnosed by imaging, pathology, and immunohistochemistry
- A Ciliated Cyst with Müllerian Differentiation Arising in the Posterior Mediastinum
- So Jung Lee, Chung Su Hwang, Do Youn Park, Gi Young Huh, Chang Hun Lee
- Korean J Pathol. 2014;48(5):401-404. Published online October 27, 2014
- DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.5.401
- 10,564 View
- 82 Download
- 11 Crossref
-
PDF
-
Citations
Citations to this article as recorded by- Rare Posterior Mediastinal Müllerian Cyst Resected by VATS: Case Report and Literature Review
Małgorzata Edyta Wojtyś, Wiktoria Skórka, Miłosz Podsiadło, Konrad Ptaszyński, Katarzyna Rodak, Dominik Jakubowski, Tomasz Grodzki
Journal of Clinical Medicine.2026; 15(7): 2773. CrossRef - Cyst of Hattori: literature review and case presentation
R. B. Berdnikov, K. A. Andryuschenko, N. S. Zavarov, E. M. Petrunina, A. V. Bazhenov, A. S. Romakhin
PULMONOLOGIYA.2025; 35(4): 553. CrossRef - Cyst of Hattori: A Rare Cyst in the Posterior Mediastinum
Matthew D. Turner, Elicia Goodale, Barry C. Gibney, Maria Cecilia D. Reyes
International Journal of Surgical Pathology.2023; 31(4): 431. CrossRef - A large retroperitoneal Mullerian cyst: case report and review of the literature
Elena Parmentier, Jody Valk, Paul Willemsen, Caroline Mattelaer
Acta Chirurgica Belgica.2021; 121(4): 278. CrossRef - A case of resected Mullerian cyst in posterior mediastinum
Yoshiyuki Susaki, Noriyoshi Sawabata
The Journal of the Japanese Association for Chest Surgery.2020; 34(2): 137. CrossRef - Serosal Inclusion Cysts and Arteriovenous Fistulas in Paraprostatic Area of a Dog
Daisuke KOJIMA, Kyoko KOJIMA, Kazumi OTA, Yoshihiko KOJIMA
Journal of the Japan Veterinary Medical Association.2020; 73(9): 511. CrossRef - A surgical case of Mullerian cyst in the posterior mediastinum
Yusuke Kita, Yoshimasa Tokunaga, Taku Okamoto
The Journal of the Japanese Association for Chest Surgery.2019; 33(1): 68. CrossRef - CT and MRI characteristics for differentiating mediastinal Müllerian cysts from bronchogenic cysts
M. Kawaguchi, H. Kato, A. Hara, N. Suzui, H. Tomita, T. Miyazaki, H. Iwata, M. Matsuo
Clinical Radiology.2019; 74(12): 976.e19. CrossRef - A case of Mullerian cyst arising in the posterior mediastinum
Masahiro Adachi, Isao Sano, Shintaro Hashimoto, Ryoichiro Doi, Hideki Taniguchi, Kazuto Shigematsu
The Journal of the Japanese Association for Chest Surgery.2018; 32(6): 713. CrossRef - Two resected cases of Mullerian cyst in the posterior mediastinum
Shotaro Hashimoto, Masato Hisano, Masato Morimoto
The Journal of the Japanese Association for Chest Surgery.2018; 32(7): 818. CrossRef - Posterior mediastinal Müllerian cyst: a rare cause of pain in a young woman
Rebecca Weedle, Keith Conway, Igor Saftic, Alan Soo
Asian Cardiovascular and Thoracic Annals.2017; 25(6): 466. CrossRef
- Rare Posterior Mediastinal Müllerian Cyst Resected by VATS: Case Report and Literature Review
- Altered Expression of PTEN and Its Major Regulator MicroRNA-21 in Pulmonary Neuroendocrine Tumors
- Hyoun Wook Lee, Seung Yeon Ha, Mee Sook Roh
- Korean J Pathol. 2014;48(1):17-23. Published online February 25, 2014
- DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.1.17
- 10,032 View
- 46 Download
- 11 Crossref
-
Abstract
PDF
Background Phosphatase and tensin homolog on chromosome ten (PTEN) is one of the most frequently inactivated tumor suppressors in various tumor types. MicroRNA-21 (miR-21) may affect tumor progression by post-transcriptional repression of expression of tumor suppressors, such as PTEN. This study was conducted to evaluate the significance of PTEN expression in pulmonary neuroendocrine (NE) tumors and to analyze the relationship between PTEN and miR-21 expressions.
Methods Expressions of PTEN and miR-21 were investigated by immunohistochemistry and real time reverse transcription-polymerase chain reaction, respectively, in 75 resected pulmonary NE tumors (23 typical carcinoids [TCs], nine atypical carcinoids [ACs], 22 large cell NE carcinomas [LCNECs], and 21 small cell lung carcinomas [SCLCs]).
Results Loss of PTEN expression was observed in four of 23 TCs (17.4%), four of nine ACs (44.4%), 16 of 22 LCNECs (72.7%) and nine of 21 SCLCs (42.9%) (p=.025). The expression level of miR-21 was significantly higher in high-grade NE carcinomas than in carcinoid tumors (p<.001). PTEN expression was inversely correlated with miR-21 expression (p<.001).
Conclusions This study suggests that aberrant expression of PTEN in relation to miR-21 may represent an important step in the development and progression of pulmonary NE tumors.
-
Citations
Citations to this article as recorded by- Mechanisms of skin wound healing regulated by fibroblast-derived exosomes
Ye Qiu, Xingying Zhu, Xiaoqian Yang, Jiaming Wan
Biochemistry and Biophysics Reports.2025; 44: 102371. CrossRef - Role of microRNAs in regulating cell proliferation, metastasis and chemoresistance and their applications as cancer biomarkers in small cell lung cancer
Monu Pandey, Abhirup Mukhopadhyay, Surender K. Sharawat, Sachin Kumar
Biochimica et Biophysica Acta (BBA) - Reviews on Cancer.2021; 1876(1): 188552. CrossRef - Neuroendocrine Tumors Are Enriched in Cowden Syndrome
Alison Greidinger, Susan Miller-Samuel, Veda N. Giri, Michele Sue-Ann Woo, Saranya Akumalla, Charnita Zeigler-Johnson, Scott W. Keith, Daniel P. Silver
JCO Precision Oncology.2020; (4): 551. CrossRef - Prognostic and predictive role of the PI3K–AKT–mTOR pathway in neuroendocrine neoplasms
P. Gajate, T. Alonso-Gordoa, O. Martínez-Sáez, J. Molina-Cerrillo, E. Grande
Clinical and Translational Oncology.2018; 20(5): 561. CrossRef - Genetic and epigenetic drivers of neuroendocrine tumours (NET)
Annunziata Di Domenico, Tabea Wiedmer, Ilaria Marinoni, Aurel Perren
Endocrine-Related Cancer.2017; 24(9): R315. CrossRef - Expression of hsa-let-7b-5p, hsa-let-7f-5p, and hsa-miR-222-3p and their putative targets HMGA2 and CDKN1B in typical and atypical carcinoid tumors of the lung
Pietro Di Fazio, Moritz Maass, Silvia Roth, Christian Meyer, Joana Grups, Peter Rexin, Detlef K Bartsch, Andreas Kirschbaum
Tumor Biology.2017; 39(10): 101042831772841. CrossRef - The regulatory role of aberrant Phosphatase and Tensin Homologue and Liver Kinase B1 on AKT/mTOR/c-Myc axis in pancreatic neuroendocrine tumors
Tsung-Ming Chang, Yan-Shen Shan, Pei-Yi Chu, Shih Sheng Jiang, Wen-Chun Hung, Yu-Lin Chen, Hsiu-Chi Tu, Hui-You Lin, Hui-Jen Tsai, Li-Tzong Chen
Oncotarget.2017; 8(58): 98068. CrossRef - Pulmonary atypical carcinoid in a patient with Cowden syndrome
Hiroaki Tsunezuka, Kaori Abe, Junichi Shimada, Masayoshi Inoue
Interactive CardioVascular and Thoracic Surgery.2016; 22(6): 860. CrossRef - Differential miRNA-Expression as an Adjunctive Diagnostic Tool in Neuroendocrine Tumors of the Lung
Melanie Demes, Christoph Aszyk, Holger Bartsch, Joachim Schirren, Annette Fisseler-Eckhoff
Cancers.2016; 8(4): 38. CrossRef - microRNA‐21 promotes osteogenic differentiation of mesenchymal stem cells by the PI3K/β‐catenin pathway
Yu‐Bin Meng, Xue Li, Zhao‐Yang Li, Jin Zhao, Xu‐Bo Yuan, Yu Ren, Zhen‐Duo Cui, Yun‐De Liu, Xian‐Jin Yang
Journal of Orthopaedic Research.2015; 33(7): 957. CrossRef - Inhibition of NADPH oxidase protects against metastasis of human lung cancer by decreasing microRNA-21
Song Yan, Gang Liu, Changyan Pei, Wenqing Chen, Pei Li, Qiang Wang, Xintian Jin, Jiajia Zhu, Mengzhu Wang, Xiyu Liu
Anti-Cancer Drugs.2015; 26(4): 388. CrossRef
- Mechanisms of skin wound healing regulated by fibroblast-derived exosomes
- Proposal for a Standardized Pathology Report of Gastroenteropancreatic Neuroendocrine Tumors: Prognostic Significance of Pathological Parameters
- Mee-Yon Cho, Jin Hee Sohn, So Young Jin, Hyunki Kim, Eun Sun Jung, Mi-Jung Kim, Kyoung-Mee Kim, Woo Ho Kim, Joon Mee Kim, Yun Kyung Kang, Joon Hyuk Choi, Dae Young Kang, Youn Wha Kim, Eun Hee Choi
- Korean J Pathol. 2013;47(3):227-237. Published online June 25, 2013
- DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.3.227
- 16,634 View
- 148 Download
- 12 Crossref
-
Abstract
PDF
Background There is confusion in the diagnosis and biological behaviors of gastroenteropancreatic neuroendocrine tumors (GEP-NETs), because of independently proposed nomenclatures and classifications. A standardized form of pathology report is required for the proper management of patients.
Methods We discussed the proper pathological evaluation of GEP-NET at the consensus conference of the subcommittee meeting for the Gastrointestinal Pathology Study Group of the Korean Society of Pathologists. We then verified the prognostic significance of pathological parameters from our previous nationwide collection of pathological data from 28 hospitals in Korea to determine the essential data set for a pathology report.
Results Histological classification, grading (mitosis and/or Ki-67 labeling index), T staging (extent, size), lymph node metastasis, and lymphovascular and perineural invasion were significant prognostic factors and essential for the pathology report of GEP-NET, while immunostaining such as synaptophysin and chromogranin may be optional. Furthermore, the staging system, either that of the 2010 American Joint Cancer Committee (AJCC) or the European Neuroendocrine Tumor Society (ENETS), should be specified, especially for pancreatic neuroendocrine neoplasms.
Conclusions A standardized pathology report is crucial for the proper management and prediction of prognosis of patients with GEP-NET.
-
Citations
Citations to this article as recorded by- Analysis of Prognostic Risk Factors of Endoscopic Submucosal Dissection (ESD) and Curative Resection of Gastrointestinal Neuroendocrine Neoplasms
Yuan Si, ChaoKang Huang, JingBin Yuan, XianHui Zhang, QingQiang He, ZhiJin Lin, Ling He, ZhongXin Liu, Yuvaraja Teekaraman
Contrast Media & Molecular Imaging.2022;[Epub] CrossRef - Standardization of the pathologic diagnosis of appendiceal mucinous neoplasms
Dong-Wook Kang, Baek-hui Kim, Joon Mee Kim, Jihun Kim, Hee Jin Chang, Mee Soo Chang, Jin-Hee Sohn, Mee-Yon Cho, So-Young Jin, Hee Kyung Chang, Hye Seung Han, Jung Yeon Kim, Hee Sung Kim, Do Youn Park, Ha Young Park, So Jeong Lee, Wonae Lee, Hye Seung Lee,
Journal of Pathology and Translational Medicine.2021; 55(4): 247. CrossRef - Preoperative diagnosis of well‐differentiated neuroendocrine tumor in common hepatic duct by brush cytology: A case report
Jiwoon Choi, Kyong Joo Lee, Sung Hoon Kim, Mee‐Yon Cho
Diagnostic Cytopathology.2019; 47(7): 720. CrossRef - Primary renal well-differentiated neuroendocrine tumors: report of six cases with an emphasis on the Ki-67 index and mitosis
Bohyun Kim, Han-Seong Kim, Kyung Chul Moon
Diagnostic Pathology.2019;[Epub] CrossRef - Primary low‐grade neuroendocrine carcinoma of the skin: An exceedingly rare entity
Tiffany Y. Chen, Annie O. Morrison, Joe Susa, Clay J. Cockerell
Journal of Cutaneous Pathology.2017; 44(11): 978. CrossRef - Prognostic Validity of the American Joint Committee on Cancer and the European Neuroendocrine Tumors Staging Classifications for Pancreatic Neuroendocrine Tumors
Jae Hee Cho, Ji Kon Ryu, Si Young Song, Jin-Hyeok Hwang, Dong Ki Lee, Sang Myung Woo, Young-Eun Joo, Seok Jeong, Seung-Ok Lee, Byung Kyu Park, Young Koog Cheon, Jimin Han, Tae Nyeun Kim, Jun Kyu Lee, Sung-Hoon Moon, Hyunjin Kim, Eun Taek Park, Jae Chul Hw
Pancreas.2016; 45(7): 941. CrossRef - Early diagnosis and treatment of gastrointestinal neuroendocrine tumors
Hong Shen, Zhuo Yu, Jing Zhao, Xiu-Zhen Li, Wen-Sheng Pan
Oncology Letters.2016; 12(5): 3385. CrossRef - Recent Updates on Neuroendocrine Tumors From the Gastrointestinal and Pancreatobiliary Tracts
Joo Young Kim, Seung-Mo Hong
Archives of Pathology & Laboratory Medicine.2016; 140(5): 437. CrossRef - Pancreatic neuroendocrine tumors: Correlation between the contrast-enhanced computed tomography features and the pathological tumor grade
Koji Takumi, Yoshihiko Fukukura, Michiyo Higashi, Junnichi Ideue, Tomokazu Umanodan, Hiroto Hakamada, Ichiro Kanetsuki, Takashi Yoshiura
European Journal of Radiology.2015; 84(8): 1436. CrossRef - Tumeurs neuroendocrines du tube digestif et du pancréas : ce que le pathologiste doit savoir et doit faire en 2014
Jean-Yves Scoazec, Anne Couvelard
Annales de Pathologie.2014; 34(1): 40. CrossRef - Spectrum of Gastroenteropancreatic NENs in Routine Histological Examinations of Bioptic and Surgical Specimen: A Study of 161 Cases Collected from 17 Departments of Pathology in the Czech Republic
Václav Mandys, Tomáš Jirásek
Gastroenterology Research and Practice.2014; 2014: 1. CrossRef - p27 Loss Is Associated with Poor Prognosis in Gastroenteropancreatic Neuroendocrine Tumors
Hee Sung Kim, Hye Seung Lee, Kyung Han Nam, Jiwoon Choi, Woo Ho Kim
Cancer Research and Treatment.2014; 46(4): 383. CrossRef
- Analysis of Prognostic Risk Factors of Endoscopic Submucosal Dissection (ESD) and Curative Resection of Gastrointestinal Neuroendocrine Neoplasms
- Morphologic Analysis of Pulmonary Neuroendocrine Tumors
- Seung Seok Lee, Myunghee Kang, Seung Yeon Ha, Jungsuk An, Mee Sook Roh, Chang Won Ha, Jungho Han
- Korean J Pathol. 2013;47(1):16-20. Published online February 25, 2013
- DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.1.16
- 8,880 View
- 52 Download
- 2 Crossref
-
Abstract
PDF
Background Few studies on how to diagnose pulmonary neuroendocrine tumors through morphometric analysis have been reported. In this study, we measured and analyzed the characteristic parameters of pulmonary neuroendocrine tumors using an image analyzer to aid in diagnosis.
Methods Sixteen cases of typical carcinoid tumor, 5 cases of atypical carcinoid tumor, 15 cases of small cell carcinoma, and 51 cases of large cell neuroendocrine carcinoma were analyzed. Using an image analyzer, we measured the nuclear area, perimeter, and the major and minor axes.
Results The mean nuclear area was 0.318±0.101 µm2 in typical carcinoid tumors, 0.326±0.119 µm2 in atypical carcinoid tumors, 0.314±0.107 µm2 in small cell carcinomas, and 0.446±0.145 µm2 in large cell neuroendocrine carcinomas. The mean nuclear circumference was 2.268±0.600 µm in typical carcinoid tumors, 2.408±0.680 µm in atypical carcinoid tumors, 2.158±0.438 µm in small cell carcinomas, and 3.247±1.276 µm in large cell neuroendocrine carcinomas. All parameters were useful in distinguishing large cell neuroendocrine carcinoma from other tumors (p=0.001) and in particular, nuclear circumference was the most effective (p=0.001).
Conclusions Pulmonary neuroendocrine tumors showed nuclear morphology differences by subtype. Therefore, evaluation of quantitative nuclear parameters improves the accuracy and reliability of diagnosis.
-
Citations
Citations to this article as recorded by- Clinical Significance of Persistent Tumor in Bone Marrow during Treatment of High-risk Neuroblastoma
Young Bae Choi, Go Eun Bae, Na Hee Lee, Jung-Sun Kim, Soo Hyun Lee, Keon Hee Yoo, Ki Woong Sung, Hong Hoe Koo
Journal of Korean Medical Science.2015; 30(8): 1062. CrossRef - Morphologic Alteration of Metastatic Neuroblastic Tumor in Bone Marrow after Chemotherapy
Go Eun Bae, Yeon-Lim Suh, Ki Woong Sung, Jung-Sun Kim
Korean Journal of Pathology.2013; 47(5): 433. CrossRef
- Clinical Significance of Persistent Tumor in Bone Marrow during Treatment of High-risk Neuroblastoma
- Clinicopathological Analysis of 21 Thymic Neuroendocrine Tumors
- Soomin Ahn, Jae Jun Lee, Sang Yun Ha, Chang Ohk Sung, Jhingook Kim, Joungho Han
- Korean J Pathol. 2012;46(3):221-225. Published online June 22, 2012
- DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.3.221
- 12,332 View
- 95 Download
- 31 Crossref
-
Abstract
PDF
Background Thymic neuroendocrine carcinomas (NECs) are uncommon, for which there is no established information available because of a limited number of epidemiological study in Asia.
Methods We reviewed 21 cases of surgically resected thymic NECs, and evaluated their pathological and clinical features.
Results It showed male predominance (male/female ratio, 15/6) with wide age range from 20 to 72 years (mean age, 49 years). All 21 cases were divided into two types according to the World Health Organization criteria: atypical carcinoid (n=18) and large cell NEC (n=3). Three cases of atypical carcinoid (AC) were associated with ectopic Cushing's syndrome. All the patients (3/3) with large cell NEC (3/3) and 16.7% (3/18) of those with AC died of tumor progression. Common sites of metastasis included lung, lymph node, brain, lumbar spine, mediastinum, bone, and liver.
Conclusions In conclusion, thymic neuroendocrine tumors carry a poor prognosis. Regarding the tumor classification, our results showed that a vast majority of carcinoids in the thymus correspond to ACs. In addition, our results also indicate that typical carcinoid is a very rare entity. Some cases of AC exhibited a large size, solid pattern and they showed aggressive clinical behavior, which highlights the spectrum of histologic appearances of thymic NECs.
-
Citations
Citations to this article as recorded by- Pathology, molecular biology, medical oncology, and radiotherapy implications of lung neuroendocrine neoplasm classification: a multidisciplinary perspective
Giuseppe Pelosi, Alice Laffi, Gianpiero Catalano, Antonino Bruno, Mauro Papotti, Barbara Bassani, Fabrizio Bianchi, Eleonora Duregon, Tommaso Martino De Pas, Chiara Catania, Riccardo Ricotta, Riccardo Papa, Sergio Harari, Angelica Sonzogni, Ilaria Guerrie
Expert Review of Anticancer Therapy.2026; 26(2): 205. CrossRef - A Case of Stage IV Thymic Typical Carcinoid with Multiple Bone Metastases
Hisaya Chikaraishi, Tomohiro Maniwa, Hironobu Samejima, Masao Kobayashi, Julian Horiguchi, Ryu Kanzaki, Hidetoshi Satomi, Keiichiro Honma, Jiro Okami
Haigan.2025; 65(4): 286. CrossRef - Neuroendocrine neoplasms of the thymus
Paul D. Barone, Chen Zhang
Frontiers in Immunology.2024;[Epub] CrossRef - Thymic neuroendocrine tumours
Jan von der Thüsen
Diagnostic Histopathology.2023; 29(2): 114. CrossRef - The Utility of Fine Needle Aspiration (FNA) Biopsy in the Diagnosis of Mediastinal Lesions
Uma Kundu, Qiong Gan, Deepak Donthi, Nour Sneige
Diagnostics.2023; 13(14): 2400. CrossRef - Paediatric and adolescent ectopic Cushing's syndrome: systematic review
Chethan Yami Channaiah, Manjiri Karlekar, Vijaya Sarathi, Anurag Ranjan Lila, Shruthi Ravindra, Padma Vikram Badhe, Gaurav Malhotra, Saba Samad Memon, Virendra Ashokrao Patil, C S Pramesh, Tushar Bandgar
European Journal of Endocrinology.2023; 189(4): S75. CrossRef - Multiple endocrine neoplasia type 1 (MEN-1) and neuroendocrine neoplasms (NENs)
Grigoris Effraimidis, Ulrich Knigge, Maria Rossing, Peter Oturai, Åse Krogh Rasmussen, Ulla Feldt-Rasmussen
Seminars in Cancer Biology.2022; 79: 141. CrossRef - Multiple electrolyte disturbances as the presenting feature of multiple endocrine neoplasia type 1 (MEN-1)
Adrian Po Zhu Li, Sheela Sathyanarayan, Salvador Diaz-Cano, Sobia Arshad, Eftychia E Drakou, Royce P Vincent, Ashley B Grossman, Simon J B Aylwin, Georgios K Dimitriadis
Endocrinology, Diabetes & Metabolism Case Reports.2022;[Epub] CrossRef - Metastatic Thymic Carcinoid: Does Surgeon Have a Primary Role?
Kumud Gupta, Ravindra K. Dewan, Vinitha Viswambharan Nair, Rajat Saxena, Shaleen Prasad
The Indian Journal of Chest Diseases and Allied Sciences.2022; 56(4): 255. CrossRef - A resected case of large cell neuroendocrine carcinoma of the thymus
Masashi Umeda, Takahiko Misao, Tomoya Senoh, Yoshinobu Shikatani, Motoi Aoe
The Journal of the Japanese Association for Chest Surgery.2022; 36(7): 766. CrossRef - Treatment strategy and prognostic analysis of spinal metastases from thymomas: A retrospective study from a single center
Shuzhong Liu, Xi Zhou, An Song, Zhen Huo, Siyuan Yao, Yipeng Wang, Yong Liu
Clinical Neurology and Neurosurgery.2020; 196: 106056. CrossRef - Large Cell Neuroendocrine Carcinoma of the Mediastinum Successfully Treated with Systemic Chemotherapy after Palliative Radiotherapy
Takeaki Hidaka, Saki Okuzumi, Ako Matsuhashi, Hidenori Takahashi, Kazunori Hata, Seiichiro Shimizu, Yoshinobu Iwasaki
Internal Medicine.2019; 58(4): 563. CrossRef - Surgical management of spinal metastases of thymic carcinoma
Shuzhong Liu, Xi Zhou, An Song, Zhen Huo, William A. Li, Radhika Rastogi, Yipeng Wang, Yong Liu
Medicine.2019; 98(3): e14198. CrossRef - Resected thymic large cell neuroendocrine carcinoma
Shogo Ogata, Ryo Maeda, Masaki Tomita, Yuichiro Sato, Takanori Ayabe, Kunihide Nakamura
International Journal of Surgery Case Reports.2019; 60(C): 53. CrossRef - Metastatic or locally advanced mediastinal neuroendocrine tumours
Aadil Adnan, Shreyas Kudachi, Sudha Ramesh, Kumar Prabhash, Sandip Basu
Nuclear Medicine Communications.2019; 40(9): 947. CrossRef - Results of treatment for thymic neuroendocrine tumours: multicentre clinicopathological study†
Naoko Ose, Hajime Maeda, Masayoshi Inoue, Eiichi Morii, Yasushi Shintani, Hiroshi Matsui, Hirohito Tada, Tositeru Tokunaga, Kenji Kimura, Yasushi Sakamaki, Yukiyasu Takeuchi, Kenjiro Fukuhara, Hiroshi Katsura, Teruo Iwasaki, Meinoshin Okumura
Interactive CardioVascular and Thoracic Surgery.2018; 26(1): 18. CrossRef - Patterns of Failure Following Postoperative Radiation Therapy Based on “Tumor Bed With Margin” for Stage II to IV Type C Thymic Epithelial Tumor
Kyung Hwa Lee, Jae Myoung Noh, Yong Chan Ahn, Dongryul Oh, Jhingook Kim, Young Mog Shim, Jung-ho Han
International Journal of Radiation Oncology*Biology*Physics.2018; 102(5): 1505. CrossRef - Resected thymic large cell neuroendocrine carcinoma: report of a case
Hiromitsu Domen, Yasuhiro Hida, Masaaki Sato, Haruka Takahashi, Tatsuru Ishikawa, Yosuke Shionoya, Midori Hashimoto, Kaoru Nishiyama, Yuma Aoki, Kazuho Inoko, Syotaro Furukawa, Kazuomi Ichinokawa, Hidehisa Yamada
Surgical Case Reports.2018;[Epub] CrossRef - Successful treatment of malignant thymoma with sacrum metastases
Shuzhong Liu, Xi Zhou, An Song, Zhen Huo, William A. Li, Radhika Rastogi, Yipeng Wang, Yong Liu
Medicine.2018; 97(51): e13796. CrossRef - Incidental metastatic mediastinal atypical carcinoid in a patient with parathyroid adenoma: a case report
Zareen Kiran, Asma Ahmed, Owais Rashid, Saira Fatima, Faizan Malik, Saulat Fatimi, Mubassher Ikram
Journal of Medical Case Reports.2017;[Epub] CrossRef - Thymus neuroendocrine tumors with CTNNB1 gene mutations, disarrayed ß-catenin expression, and dual intra-tumor Ki-67 labeling index compartmentalization challenge the concept of secondary high-grade neuroendocrine tumor: a paradigm shift
Alessandra Fabbri, Mara Cossa, Angelica Sonzogni, Paolo Bidoli, Stefania Canova, Diego Cortinovis, Maria Ida Abbate, Fiorella Calabrese, Nazarena Nannini, Francesca Lunardi, Giulio Rossi, Stefano La Rosa, Carlo Capella, Elena Tamborini, Federica Perrone,
Virchows Archiv.2017; 471(1): 31. CrossRef - Thymic large cell neuroendocrine carcinoma – a rare and aggressive tumor: a case report
Efared Boubacar, Gabrielle Atsame-Ebang, Sani Rabiou, Ammor Fatimazahra, Asmae Mazti, Ibrahim S. Sidibé, Layla Tahiri, Nawal Hammas, Ouadnouni Yassine, Smahi Mohamed, Chbani Laila, El Fatemi Hinde
Journal of Medical Case Reports.2017;[Epub] CrossRef - Clinicopathological features of neoplasms with neuroendocrine differentiation occurring in the liver
Yoriko Nomura, Osamu Nakashima, Jun Akiba, Sachiko Ogasawara, Shogo Fukutomi, Rin Yamaguchi, Hironori Kusano, Masayoshi Kage, Koji Okuda, Hirohisa Yano
Journal of Clinical Pathology.2017; 70(7): 563. CrossRef - Retrosternal goiter and thymic carcinoid: A rare co-existence
Abdulsalam Yaseen Taha, Nezar A. Almahfooz, Hassanain H. Khudair
Journal of the Egyptian Society of Cardio-Thoracic Surgery.2017; 25(4): 369. CrossRef - A case of large-cell neuroendocrine carcinoma of the thymus involving a patient with long-term survival after surgery
Qiuming Kan, Kohei Tagawa, Teruaki Ishida, Mitsuyo Nishimura, Katsuhiko Aoyama
The Journal of the Japanese Association for Chest Surgery.2017; 31(7): 927. CrossRef - Neuroendokrine Neoplasien des Mediastinums
L. Brcic, M. Heidinger, H. Popper
Der Pathologe.2016; 37(5): 434. CrossRef - Outcome of primary neuroendocrine tumors of the thymus: A joint analysis of the International Thymic Malignancy Interest Group and the European Society of Thoracic Surgeons databases
Pier Luigi Filosso, Xiaopan Yao, Usman Ahmad, Yilei Zhan, James Huang, Enrico Ruffini, William Travis, Marco Lucchi, Andreas Rimner, Alberto Antonicelli, Francesco Guerrera, Frank Detterbeck
The Journal of Thoracic and Cardiovascular Surgery.2015; 149(1): 103. CrossRef - Clinical Significance of Persistent Tumor in Bone Marrow during Treatment of High-risk Neuroblastoma
Young Bae Choi, Go Eun Bae, Na Hee Lee, Jung-Sun Kim, Soo Hyun Lee, Keon Hee Yoo, Ki Woong Sung, Hong Hoe Koo
Journal of Korean Medical Science.2015; 30(8): 1062. CrossRef - Tumor genetics and survival of thymic neuroendocrine neoplasms: A multi‐institutional clinicopathologic study
Philipp Ströbel, Andreas Zettl, Konstantin Shilo, Wen‐Yu Chuang, Andrew G. Nicholson, Yoshihiro Matsuno, Anthony Gal, Rolf Hubert Laeng, Peter Engel, Carlo Capella, Mirella Marino, John Kwok-Cheung Chan, Andreas Rosenwald, William Travis, Teri J. Franks,
Genes, Chromosomes and Cancer.2014; 53(9): 738. CrossRef - Disseminated large cell neuroendocrine carcinoma associated with ectopic adrenocorticotropic hormone secretion
A Van der Walt, K Huddle, S Pather, A Korb
Journal of Endocrinology, Metabolism and Diabetes of South Africa.2014; 19(1): 40. CrossRef - Morphologic Alteration of Metastatic Neuroblastic Tumor in Bone Marrow after Chemotherapy
Go Eun Bae, Yeon-Lim Suh, Ki Woong Sung, Jung-Sun Kim
Korean Journal of Pathology.2013; 47(5): 433. CrossRef
- Pathology, molecular biology, medical oncology, and radiotherapy implications of lung neuroendocrine neoplasm classification: a multidisciplinary perspective
- Interobserver Variability in Diagnosing High-Grade Neuroendocrine Carcinoma of the Lung and Comparing It with the Morphometric Analysis
- Seung Yeon Ha, Joungho Han, Wan-Seop Kim, Byung Seong Suh, Mee Sook Roh
- Korean J Pathol. 2012;46(1):42-47. Published online February 23, 2012
- DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.1.42
- 10,636 View
- 51 Download
- 22 Crossref
-
Abstract
PDF
Background Distinguishing small cell lung carcinoma (SCLC) and large cell neuroendocrine carcinoma (LCNEC) of the lung is difficult with little information about interobserver variability.
Methods One hundred twenty-nine cases of resected SCLC and LCNEC were independently evaluated by four pathologists and classified according to the 2004 World Health Organization criteria. Agreement was regarded as "unanimous" if all four pathologists agreed on the classification. The kappa statistic was calculated to measure the degree of agreement between pathologists. We also measured cell size using image analysis, and receiver-operating-characteristic curve analysis was performed to evaluate cell size in predicting the diagnosis of high-grade neuroendocrine (NE) carcinomas in 66 cases.
Results Unanimous agreement was achieved in 55.0% of 129 cases. The kappa values ranged from 0.35 to 0.81. Morphometric analysis reaffirmed that there was a continuous spectrum of cell size from SCLC to LCNEC and showed that tumors with cells falling in the middle size range were difficult to categorize and lacked unanimous agreement.
Conclusions Our results provide an objective explanation for considerable interobserver variability in the diagnosis of high-grade pulmonary NE carcinomas. Further studies would need to define more stringent and objective definitions of cytologic and architectural characteristics to reliably distinguish between SCLC and LCNEC.
-
Citations
Citations to this article as recorded by- Case report: A patient with EGFR L861Q positive adenosquamous lung carcinoma transforming into large cell neuroendocrine cancer after treatment with Almonertinib
Kele Cheng, Yong Zhu, Ran Sang, Zhongsheng Kuang, Yang Cao
Frontiers in Oncology.2025;[Epub] CrossRef - Deep Learning–Based Retinoblastoma Protein Subtyping of Pulmonary Large-Cell Neuroendocrine Carcinoma on Small Hematoxylin and Eosin–Stained Specimens
Teodora E. Trandafir, Frank W.J. Heijboer, Farhan Akram, Jules L. Derks, Yunlei Li, Lisa M. Hillen, Ernst-Jan M. Speel, Zsolt Megyesfalvi, Balazs Dome, Andrew P. Stubbs, Anne-Marie C. Dingemans, Jan H. von der Thüsen
Laboratory Investigation.2025; 105(9): 104192. CrossRef - Treatment outcomes in patients with stage IV large cell neuroendocrine carcinoma: a nationwide registry study
Frank W.J. Heijboer, Jules L. Derks, Francien H. van Nederveen, Lisa M. Hillen, Michael A. den Bakker, Teodora Radonic, Ronald A.M. Damhuis, Ernst-Jan M. Speel, Jan H. von der Thüsen, Anne-Marie C. Dingemans
Lung Cancer.2025; 210: 108830. CrossRef - Updates on lung neuroendocrine neoplasm classification
Giulia Vocino Trucco, Luisella Righi, Marco Volante, Mauro Papotti
Histopathology.2024; 84(1): 67. CrossRef - Recent advancement of HDAC inhibitors against breast cancer
Syed Abdulla Mehmood, Kantrol Kumar Sahu, Sounok Sengupta, Sangh Partap, Rajshekhar Karpoormath, Brajesh Kumar, Deepak Kumar
Medical Oncology.2023;[Epub] CrossRef - Genomic Feature of a Rare Case of Mix Small-Cell and Large-Cell Neuroendocrine Lung Carcinoma: A Case Report
Youcai Zhu, Feng Zhang, Dong Yu, Fang Wang, Manxiang Yin, Liangye Chen, Chun Xiao, Yueyan Huang, Feng Ding
Frontiers in Oncology.2022;[Epub] CrossRef - Small-Cell Carcinoma of the Lung: What We Learned about It?
Luisella Righi, Marco Volante, Mauro Papotti
Acta Cytologica.2022; 66(4): 257. CrossRef - Hierarchical identification of a transcriptional panel for the histological diagnosis of lung neuroendocrine tumors
Juxuan Zhang, Jiaxing Deng, Xiao Feng, Yilong Tan, Xin Li, Yixin Liu, Mengyue Li, Haitao Qi, Lefan Tang, Qingwei Meng, Haidan Yan, Lishuang Qi
Frontiers in Genetics.2022;[Epub] CrossRef - Immunohistochemical Staining With Neuroendocrine Markers is Essential in the Diagnosis of Neuroendocrine Neoplasms of the Esophagogastric Junction
Dea N.M. Jepsen, Anne-Marie K. Fiehn, Rajendra S. Garbyal, Ulla Engel, Jakob Holm, Birgitte Federspiel
Applied Immunohistochemistry & Molecular Morphology.2021; 29(6): 454. CrossRef - Improving differential diagnosis of pulmonary large cell neuroendocrine carcinoma and small cell lung cancer via a transcriptomic, biological pathway-based machine learning model
Junhong Guo, Likun Hou, Wei Zhang, Zhengwei Dong, Lei Zhang, Chunyan Wu
Translational Oncology.2021; 14(12): 101222. CrossRef - Are Neuroendocrine Negative Small Cell Lung Cancer and Large Cell Neuroendocrine Carcinoma with WT RB1 two Faces of the Same Entity?
Dmitriy Sonkin, Anish Thomas, Beverly A Teicher
Lung Cancer Management.2019;[Epub] CrossRef - Ki-67 labeling index of neuroendocrine tumors of the lung has a high level of correspondence between biopsy samples and surgical specimens when strict counting guidelines are applied
Alessandra Fabbri, Mara Cossa, Angelica Sonzogni, Mauro Papotti, Luisella Righi, Gaia Gatti, Patrick Maisonneuve, Barbara Valeri, Ugo Pastorino, Giuseppe Pelosi
Virchows Archiv.2017; 470(2): 153. CrossRef - The Use of Immunohistochemistry Improves the Diagnosis of Small Cell Lung Cancer and Its Differential Diagnosis. An International Reproducibility Study in a Demanding Set of Cases
Erik Thunnissen, Alain C. Borczuk, Douglas B. Flieder, Birgit Witte, Mary Beth Beasley, Jin-Haeng Chung, Sanja Dacic, Sylvie Lantuejoul, Prudence A. Russell, Michael den Bakker, Johan Botling, Elisabeth Brambilla, Erienne de Cuba, Kim R. Geisinger, Kenzo
Journal of Thoracic Oncology.2017; 12(2): 334. CrossRef - Reply to Letter “The Use of Immunohistochemistry Improves the Diagnosis of Small Cell Lung Cancer and Its Differential Diagnosis. An International Reproducibility Study in a Demanding Set of Cases.”
Erik Thunnissen, Birgit I. Witte, Masayuki Noguchi, Yasushi Yatabe
Journal of Thoracic Oncology.2017; 12(6): e70. CrossRef - What clinicians are asking pathologists when dealing with lung neuroendocrine neoplasms?
Giuseppe Pelosi, Alessandra Fabbri, Mara Cossa, Angelica Sonzogni, Barbara Valeri, Luisella Righi, Mauro Papotti
Seminars in Diagnostic Pathology.2015; 32(6): 469. CrossRef - Unraveling Tumor Grading and Genomic Landscape in Lung Neuroendocrine Tumors
Giuseppe Pelosi, Mauro Papotti, Guido Rindi, Aldo Scarpa
Endocrine Pathology.2014; 25(2): 151. CrossRef - Grading the neuroendocrine tumors of the lung: an evidence-based proposal
G Rindi, C Klersy, F Inzani, G Fellegara, L Ampollini, A Ardizzoni, N Campanini, P Carbognani, T M De Pas, D Galetta, P L Granone, L Righi, M Rusca, L Spaggiari, M Tiseo, G Viale, M Volante, M Papotti, G Pelosi
Endocrine-Related Cancer.2014; 21(1): 1. CrossRef - Controversial issues and new discoveries in lung neuroendocrine tumors
Giuseppe Pelosi, Kenzo Hiroshima, Mari Mino-Kenudson
Diagnostic Histopathology.2014; 20(10): 392. CrossRef - BAI3, CDX2 and VIL1: a panel of three antibodies to distinguish small cell from large cell neuroendocrine lung carcinomas
Muhammad F Bari, Helen Brown, Andrew G Nicholson, Keith M Kerr, John R Gosney, William A Wallace, Irshad Soomro, Salli Muller, Danielle Peat, Jonathan D Moore, Lesley A Ward, Maxim B Freidin, Eric Lim, Manu Vatish, David R J Snead
Histopathology.2014; 64(4): 547. CrossRef - Neuroendocrine tumours—challenges in the diagnosis and classification of pulmonary neuroendocrine tumours
M A den Bakker, F B J M Thunnissen
Journal of Clinical Pathology.2013; 66(10): 862. CrossRef - Morphologic Analysis of Pulmonary Neuroendocrine Tumors
Seung Seok Lee, Myunghee Kang, Seung Yeon Ha, Jungsuk An, Mee Sook Roh, Chang Won Ha, Jungho Han
Korean Journal of Pathology.2013; 47(1): 16. CrossRef - Altered expression of microRNA miR‐21, miR‐155, and let‐7a and their roles in pulmonary neuroendocrine tumors
Hyoun Wook Lee, Eun Hee Lee, Seung Yeon Ha, Chang Hun Lee, Hee Kyung Chang, Sunhee Chang, Kun Young Kwon, Il Seon Hwang, Mee Sook Roh, Jeong Wook Seo
Pathology International.2012; 62(9): 583. CrossRef
- Case report: A patient with EGFR L861Q positive adenosquamous lung carcinoma transforming into large cell neuroendocrine cancer after treatment with Almonertinib
- Nuclear Image Analysis Study of Neuroendocrine Tumors
- Meeja Park, Taehwa Baek, Jongho Baek, Hyunjin Son, Dongwook Kang, Jooheon Kim, Hyekyung Lee
- Korean J Pathol. 2012;46(1):38-41. Published online February 23, 2012
- DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.1.38
- 9,261 View
- 41 Download
- 2 Crossref
-
Abstract
PDF
Background There is a subjective disagreement about nuclear chromatin in the field of pathology. Objective values of red, green, and blue (RGB) light intensities for nuclear chromatin can be obtained through a quantitative analysis using digital images.
Methods We examined 10 cases of well differentiated neuroendocrine tumors of the rectum, small cell lung carcinomas, and moderately differentiated squamous cell lung carcinomas respectively. For each case, we selected 30 representative cells and captured typical microscopic findings. Using an image analyzer, we determined the longest nuclear line profiles and obtained graph files and Excel data on RGB light intensities. We assessed the meaningful differences in graph files and Excel data among the three different tumors.
Results The nucleus of hematoxylin and eosin-stained tumor cells was expressed as a combination of RGB light sources. The highest intensity was from blue, whereas the lowest intensity was from green. According to the graph files, green showed the most noticeable change in the light intensity, which is consistent with the difference in standard deviations.
Conclusions The change in the light intensity for green has an important implication for differentiating between tumors. Specific features of the nucleus can be expressed in specific values of RGB light intensities.
-
Citations
Citations to this article as recorded by- Difference of the Nuclear Green Light Intensity between Papillary Carcinoma Cells Showing Clear Nuclei and Non-neoplastic Follicular Epithelia in Papillary Thyroid Carcinoma
Hyekyung Lee, Tae Hwa Baek, Meeja Park, Seung Yun Lee, Hyun Jin Son, Dong Wook Kang, Joo Heon Kim, Soo Young Kim
Journal of Pathology and Translational Medicine.2016; 50(5): 355. CrossRef - Comparison of diagnostic accuracy between CellprepPlus® and ThinPrep® liquid‐based preparations in effusion cytology
Yong‐Moon Lee, Ji‐Yong Hwang, Seung‐Myoung Son, Song‐Yi Choi, Ho‐Chang Lee, Eun‐Joong Kim, Hye‐Suk Han, Jin young An, Joung‐Ho Han, Ok‐Jun Lee
Diagnostic Cytopathology.2014; 42(5): 384. CrossRef
- Difference of the Nuclear Green Light Intensity between Papillary Carcinoma Cells Showing Clear Nuclei and Non-neoplastic Follicular Epithelia in Papillary Thyroid Carcinoma
- Composite Tumor of Adenocarcinoma and Small Cell Neuroendocrine Carcinoma of the Uterine Cervix: A Case Report.
- Hye Rim Park, Yong Woo Lee, Young Euy Park
- J Pathol Transl Med. 1990;1(1):111-120.
- 2,836 View
- 45 Download
-
Abstract
PDF
- Small cell neuroendocrine carcinoma of the uterine cervix is a distinct subtype of cervical cancer that appears analogous to oat cell carcinoma and carcinoid tumors of the lung. It has been assumed to be derived from the neural crest via argyrophilic cells in the normal endocervix. We have recently encountered a case of small cell neuroendocrine carcinoma of the uterine cervix coexisting with adenocarcinoma which was argyrophil negative. A 66-year-old multiparous woman was admitted because of vaginal bleeding for 2 months. Cervicovaginal smear revealed several scattered clusters and sheets of monotonous small cells with some peripheral palisading in the background of hemorrhage and necrosis. Radical hysterectomy specimen revealed and ulcerofungating tumor on endocervical canal which was composed of two components. Major component of the tumor was made up of monomorphic population of small oval-shaped tumor cells arranged in sheets and partly in acinar structeres or trabecular fashion. Other component was adenocarcinoma, endocervical well-differentiated type. Argyropilia was present on the Grimelius stain and immunohistochemical studies revealed diffuse positivity to neuron-specific enolase and carcinoembryonic antigen. Electron microscopic examination showed clusters of small round to oval cells, which had a few well-formed desmosomes and several membrane-bound, dense-core neurosectetory granules.
- Mixed Endocrine-Exocrine Carcinoma of Gallbladder Derived from Dysplasia.
- Min Jin Lhee, Ji Young Woo
- Korean J Pathol. 2011;45(5):537-541.
- DOI: https://doi.org/10.4132/KoreanJPathol.2011.45.5.537
- 3,834 View
- 19 Download
-
Abstract
PDF
- A rare case of multiple mixed endocrine-exocrine carcinoma (MEEC) of gallbladder in a 68-year-old man is described. The lesions were two separate nodules (17x13x7 mm and 17 mm in length) on the mucosa, which were composed of predominant neuroendocrine carcinoma (NEC) infiltrating into the adventitia and minor portion of adenocarcinoma (AC) or high grade dysplasia (HGD) on the surface. Surrounding mucosa showed areas of low grade dysplasia (LGD). Two nodal metastases out of 16 nodes were found containing NEC component. By immunohistochemistry, human mutL homolog 1 (hMLH1), p53, human mutS homolog 2 (hMSH2) and human mutS homolog 6 (hMSH6) showed diffuse strong positive reaction in HGD, AC and NEC, contrasting with weak positive reaction in LGD. On genetic analysis, all lesions of HGD, AC, and NEC except for LGD showed positive loss of heterozygosity in D5S346 locus. For microsatellite instability and K-ras mutation tests, all lesions showed negative results. Common immunophenotypes and molecular results among HGD, AC, and NEC suggested that NEC of this MEEC was derived from the dysplasia-AC sequence.
- Ovarian Large Cell Neuroendocrine Carcinoma Associated with Endocervical-like Mucinous Borderline Tumor: A Case Report and Literature Review.
- Jun Mo Kim, Hyeong Chan Shin, Mi Jin Kim
- Korean J Pathol. 2011;45(5):523-528.
- DOI: https://doi.org/10.4132/KoreanJPathol.2011.45.5.523
- 5,644 View
- 36 Download
- 4 Crossref
-
Abstract
PDF
- Ovarian large cell neuroendocrine carcinoma is a rare tumor that is usually associated with surface epithelial tumors. Mucinous tumors are most common surface epithelial component identified in reported cases. Ovarian mucinous tumor associated with large cell neuroendocrine carcinoma is almost always an intestinal type. However, large cell neuroendocrine carcinoma associated with pure mucinous borderline tumor of endocervical-like type has not been described previously. The present case report describes a large cell neuroendocrine carcinoma associated with endocervical-like mucinous borderline tumor of the ovary in a 35-year-old woman. The tumor was confirmed by histopathology and immunohistochemistry. A review of the pertinent literature is included.
-
Citations
Citations to this article as recorded by- The puzzle of gynecologic neuroendocrine carcinomas: State of the art and future directions
Giuseppe Caruso, Carolina Maria Sassu, Federica Tomao, Violante Di Donato, Giorgia Perniola, Margherita Fischetti, Pierluigi Benedetti Panici, Innocenza Palaia
Critical Reviews in Oncology/Hematology.2021; 162: 103344. CrossRef - Pathological features, clinical presentations and prognostic factors of ovarian large cell neuroendocrine carcinoma: a case report and review of published literature
Xiaohang Yang, Junyu Chen, Ruiying Dong
Journal of Ovarian Research.2019;[Epub] CrossRef - Primary pure large cell neuroendocrine carcinoma of the ovary
Chen-Hsien Lin, Yu-Chieh Lin, Mu-Hsien Yu, Her-Young Su
Taiwanese Journal of Obstetrics and Gynecology.2014; 53(3): 413. CrossRef - Pure Large Cell Neuroendocrine Carcinoma of Ovary: A Rare Clinical Entity and Review of Literature
P. N. Shakuntala, K. Uma Devi, K. Shobha, U. D. Bafna, M. Geetashree
Case Reports in Oncological Medicine.2012; 2012: 1. CrossRef
- The puzzle of gynecologic neuroendocrine carcinomas: State of the art and future directions
- SSTR2A Protein Expression in Neuroendocrine Neoplasms of the Colorectum.
- Young Eun Kim, Jeeyun Lee, Young Suk Park, Kyoung Mee Kim
- Korean J Pathol. 2011;45(3):276-280.
- DOI: https://doi.org/10.4132/KoreanJPathol.2011.45.3.276
- 4,628 View
- 25 Download
-
Abstract
PDF
- BACKGROUND
Expression studies of somatostatin receptor type 2A (SSTR2A) in neuroendocrine neoplasms (NENs) led to the development of clinically relevant diagnostic and therapeutic strategies. However, most of these strategies used in-house-developed antibodies and were focused on lung tumors. We evaluated commercially available SSTR2A antibodies in NENs of the colorectum to observe their subcellular localization and distribution within the resected tumor.
METHODS
The immunohistochemistry of 77 NENs located in the colorectum were studied using a commercially available antibody against SSTR2A.
RESULTS
Most neuroendocrine tumors (NET) grade (G)1 and G2 expressed the SSTR2A in the cytoplasm with apical or luminal localization. However, all neuroendocrine carcinomas (NEC) G3 were negative for SSTR2A.
CONCLUSIONS
Our data indicate that SSTR2A immunohistochemistry shows cytoplasmic staining with distinct subcellular localization in most NET G1 in the colorectum using a commercially available antibody. Low or no expression of SSTR2A in NET G2 and NEC G3 raises the possibility that SSTR2A may correlate with histologic differentiation and proliferative activity. Further validation studies in large case series are needed.
- Distinction of Pulmonary Large Cell Neuroendocrine Carcinoma from Small Cell Lung Carcinoma Using a Panel of Bcl-2, p63, and 34betaE12.
- Jun Zhe Li, Chan Choi, Yoo Duk Choi, Kook Joo Na
- Korean J Pathol. 2011;45(2):170-174.
- DOI: https://doi.org/10.4132/KoreanJPathol.2011.45.2.170
- 4,397 View
- 33 Download
- 1 Crossref
-
Abstract
PDF
- BACKGROUND
Making the distinction between large cell neuroendocrine carcinoma (LCNEC) and small cell lung carcinoma (SCLC) is difficult in some samples of biopsy tissues, but we have to separate LCNEC from SCLC because the two types of cancer may need different therapy and they have different prognostic implications. Thus far, there are no specific immunohistochemical markers that allow distinguishing these two kinds of tumors.
METHODS
We performed an immunohistochemical analysis to study the expressions of p63, Bcl-2, and 34betaE12 and to investigate whether these 3 molecules have correlations in LCNEC and SCLC. We also evaluated the expression of the neuroendocrine markers chromogranin, synaptophysin and CD56.
RESULTS
A statistical analysis was performed for p63, Bcl-2, and 34betaE12 in separate and combined panels. According to the combinations of p63, Bcl-2, and 34betaE12, there were frequent expressions of p63-/Bcl-2+ or Bcl-2+/34betaE12- in the SCLC, and there was a superior proportion of them in the SCLC rather than that in the LCNEC. The p63-/Bcl-2+ and Bcl-2+/34betaE12- antibody combinations showed higher specificities compared to any single antibody for diagnosing SCLC.
CONCLUSIONS
Bcl-2 and selective p63 or 34betaE12 made up a most useful panel of markers for making the differential diagnosis of LCNEC and SCLC. -
Citations
Citations to this article as recorded by- Evaluation of Serum LDH, p53 and BCL2 in Lung Cancer Patients
Pawar Komal, Rajvik Kruti, Vora Hemangini
Gujarat Cancer Society Research Journal.2020; 22(2): 22. CrossRef
- Evaluation of Serum LDH, p53 and BCL2 in Lung Cancer Patients
- CK20 Negative and CK7 Positive Merkel Cell Carcinoma of the Conjunctiva: Brief Case Report.
- Jung Ha Shin, Jae Young Park, Hyun Seung Kim, Ok Ran Shin, Kyo Young Lee
- Korean J Pathol. 2010;44(6):675-678.
- DOI: https://doi.org/10.4132/KoreanJPathol.2010.44.6.675
- 7,154 View
- 58 Download
-
Abstract
PDF
- Merkel cell carcinoma (MCC) is an uncommon but potentially aggressive neuroendocrine carcinoma of the skin. It typically develops on sun-exposed areas of the head and neck, particularly the eyelid, periorbital region, and extremities. We report a case of unusually located MCC, presenting as a conjunctival mass, which has only been reported once in the English literature. An 83-year-old male presented with a 0.8 x 0.7 cm sized mass protruding from the lower fornix of the right conjunctiva. The mass was excised. The tumor was located in the submucosa without connection to the overlying mucosa. Light microscopic findings showed a carcinoma with undifferentiated small round cells and the presence of cytokeratin (CK AE1/3, CK7) and neuroendocrine markers. We established a diagnosis of MCC. As reported in the literature, the majority of MCCs are positive for CK20 but negative for CK7. But, this case showed an uncommon cytokeratin immunohistochemical profile of positive for CK7 and negative for CK20, suggesting a new immunophenotypic MCC variant.
- A Case of Endocrine Mucin-Producing Sweat Gland Carcinoma Co-existing with Mucinous Carcinoma: A Case Report.
- Sunhee Chang, Sang Hwa Shim, Mee Joo, Hanseong Kim, Yong Kyu Kim
- Korean J Pathol. 2010;44(1):97-100.
- DOI: https://doi.org/10.4132/KoreanJPathol.2010.44.1.97
- 6,058 View
- 57 Download
- 9 Crossref
-
Abstract
PDF
- An endocrine mucin-producing sweat gland carcinoma (EMPSGC) is a rare skin tumor that most commonly occurs on the eyelids of elderly women. This tumor is morphologically analogous to endocrine ductal carcinoma in situ and solid papillary carcinoma of the breast. We describe one case of a 51-year-old male with an EMPSGC co-existing with mucinous carcinoma of the eyelid. The tumor was composed of dilated ducts with a smooth border and was partially filled with a papillary proliferation. Tumor cells were uniform, small-to-medium in size, and oval-to-polygonal with light eosinophilic cytoplasm. Nuclei were bland with diffusely stippled chromatin and inconspicuous nucleoli. Tumor cells expressed chromogranin, synaptophysin, estrogen and progesterone receptors, cytokeratin 7, and epithelial membrane antigen.
-
Citations
Citations to this article as recorded by- A Case of Endocrine Mucin-Producing Sweat Gland Carcinoma of the Eyelid
Ji Eon Kang, Sung Eun Kim, Suk-Woo Yang
Journal of the Korean Ophthalmological Society.2023; 64(2): 149. CrossRef - Endocrine mucin-producing sweat gland carcinoma: a systematic review and meta-analysis
Michael H. Froehlich, Keith R. Conti, Ivy I. Norris, Jordan J. Allensworth, Nicole A. Ufkes, Shaun A. Nguyen, Evelyn T. Bruner, Joel Cook, Terry A. Day
Journal of Dermatological Treatment.2022; 33(4): 2182. CrossRef - Next-generation sequencing analysis suggests varied multistep mutational pathogenesis for endocrine mucin-producing sweat gland carcinoma with comments on INSM1 and MUC2 suggesting a conjunctival origin
Joseph G. Mathew, Anita S. Bowman, Jad Saab, Klaus J. Busam, Kishwer Nehal, Melissa Pulitzer
Journal of the American Academy of Dermatology.2022; 86(5): 1072. CrossRef - Endocrine mucin‐producing sweat gland carcinoma and associated primary cutaneous mucinous carcinoma: Review of the literature
Rebecca Tian Mei Au, Manish M. Bundele
Journal of Cutaneous Pathology.2021; 48(9): 1156. CrossRef - An Update on Endocrine Mucin-producing Sweat Gland Carcinoma
Meghana Agni, Meisha L. Raven, Randy C. Bowen, Nora V. Laver, Patricia Chevez-Barrios, Tatyana Milman, Charles G. Eberhart, Steven Couch, Daniel D. Bennett, Daniel M. Albert, R. Nick Hogan, Paul O. Phelps, Hillary Stiefel, Norberto Mancera, Martin Hyrcza,
American Journal of Surgical Pathology.2020; 44(8): 1005. CrossRef - A Case of Endocrine Mucin-Producing Sweat Gland Carcinoma: Is it Still an Under-Recognized Entity?
Khaled A. Murshed, Mohamed Ben-Gashir
Case Reports in Dermatology.2020; 12(3): 255. CrossRef - Endocrine Mucin-Producing Sweat Gland Carcinoma, a Histological Challenge
Mary Anne Brett, Samih Salama, Gabriella Gohla, Salem Alowami
Case Reports in Pathology.2017; 2017: 1. CrossRef - Endocrine mucin‐producing sweat gland carcinoma occurring on extra‐facial site: a case report
Jia‐Huei Tsai, Tzu‐Lin Hsiao, Yi‐Ying Chen, Cheng‐Hsiang Hsiao, Jau‐Yu Liau
Journal of Cutaneous Pathology.2014; 41(6): 544. CrossRef - Endocrine Mucin-Producing Sweat Gland Carcinoma
Catharine A. Dhaliwal, Antonia Torgersen, Jonathan J. Ross, James W. Ironside, Asok Biswas
The American Journal of Dermatopathology.2013; 35(1): 117. CrossRef
- A Case of Endocrine Mucin-Producing Sweat Gland Carcinoma of the Eyelid
- Differential Expression of Glut1 in Pulmonary Neuroendocrine Tumors: Correlation with Histological Grade.
- Hyun Ju Lee, Seol Bong Yoo, Won Woo Lee, Doo Hyun Chung, Jeong Wook Seo, Jin Haeng Chung
- Korean J Pathol. 2009;43(3):201-205.
- DOI: https://doi.org/10.4132/KoreanJPathol.2009.43.3.201
- 5,569 View
- 39 Download
- 2 Crossref
-
Abstract
PDF
- BACKGROUND
Increased glucose uptake, a process that is mediated by glucose transporter (Glut1) proteins, is an important metabolic feature in a variety of cancer cells. The overexpression of Glut1 in human cancers is known to be related to a variety of histopathological parameters, including histological grade, proliferation rate, and lymphatic invasion. The principal objective of this study was to evaluate Glut1 expression in the spectrum of pulmonary neuroendocrine (NE) tumors including typical carcinoid tumor (TC), atypical carcinoid tumor (AC), large cell neuroendocrine carcinoma (LCNEC), and small cell carcinoma (SCC), and to characterize the relationship between Glut1 expression and the histologic grade of NE tumors.
METHODS
19 TC, 7 AC, 13 LCNEC, and 6 SCC patients were included in this study. The percentages of Glut1-positive tumor cells in these patients were determined. For statistical analysis, Glut1 expression was subdivided into a Glut1-low expression group (0-30%) and a Glut1-high expression group (31-90%).
RESULTS
In our subgroup analyses, the histological grade of pulmonary neuroendocrine (NE) tumors was significantly correlated with Glut1 expression; TC (n=19, 3.6+/-4.2%), AC (n=7, 20.0+/-4.9%), LCNEC (n=13, 60.0+/-21.1%), and SCC (n=6, 74.2+/-16.9%). Glut1-high expression was significantly associated with high-grade NE tumors such as LCNEC and SCC (n=19, 62.6+/-21.0%) (p=0.000).
CONCLUSIONS
The results of this study appear to indicate that Glut1 overexpression is a consistent feature of high-grade NE lung tumors. -
Citations
Citations to this article as recorded by- GLUT1: A novel tool reflecting proliferative activity of lung neuroendocrine tumors?
Nazim Benzerdjeb, Pascal Berna, Henri Sevestre
Pathology International.2017; 67(1): 32. CrossRef - Oncocytic carcinoid tumor of the lung with intense F-18 fluorodeoxyglucose (FDG) uptake in positron emission tomography–computed tomography (PET/CT)
Yuki Tanabe, Yoshifumi Sugawara, Rieko Nishimura, Kohei Hosokawa, Makoto Kajihara, Teruhiko Shimizu, Tadaaki Takahashi, Shinya Sakai, Shigeki Sawada, Motohiro Yamashita, Haruhiko Ohtani
Annals of Nuclear Medicine.2013; 27(8): 781. CrossRef
- GLUT1: A novel tool reflecting proliferative activity of lung neuroendocrine tumors?
- Gastric Adenocarcinoma with Coexistent Hepatoid Adenocarcinoma and Neuroendocrine Carcinoma: A Case Report.
- Aeri Kim, Sang Woon Kim, Sun Kyo Song, Young Kyung Bae
- Korean J Pathol. 2009;43(1):79-82.
- DOI: https://doi.org/10.4132/KoreanJPathol.2009.43.1.79
- 4,732 View
- 36 Download
- 2 Crossref
-
Abstract
PDF
- This report represents a very rare case of a gastric adenocarcinoma that was coexistent with hepatoid adenocarcinoma and neuroendocrine carcinoma. A 77-year-old man was admitted to our hospital due to a huge ulcerofungating mass identified at the proximal body of the stomach. After a pathological diagnosis of the tumor as a poorly differentiated adenocarcinoma was made, the patient underwent a total gastrectomy with lymph node dissection. Microscopically, the tumor consisted of three morphologically distinct components-tubular adenocarcinoma, hepatoid adenocarcinoma and neuroendocrine carcinoma. The hepatoid adenocarcinoma component resembled a hepatocellular carcinoma and produced alpha-fetoprotein. The neuroendocrine carcinoma component was positive for chromogranin and synaptophysin immunostains. This is an example of the diverse morphological and immunophenotypical differentiation of gastric carcinomas.
-
Citations
Citations to this article as recorded by- An Intestinal Type Gastric Neuroendocrine Tumor: A Case Report
Mohammad Abu-Jeyyab, Renata Kakish, Malak Alkatib, Leen Alshawabkeh, Rawan Bani Hamad, Mary Almadani, Ma'wia Santarisi, Mohammad Al-Jafari, Abdulqadir J. Nashwan
Case Reports in Oncology.2023; 16(1): 1113. CrossRef - Gastric adenocarcinoma is concurrent with metastatic neuroendocrine cancer treated with nivolumab and chemotherapy: A case report
Bing Yan, Meiqi Cui, Junhao You, Fang Li, Hui Liu
Molecular and Clinical Oncology.2018;[Epub] CrossRef
- An Intestinal Type Gastric Neuroendocrine Tumor: A Case Report
- Fine Needle Aspiration Cytologic Findings of Pulmonary Neuroendocrine Tumors.
- Jae Soo Koh
- J Pathol Transl Med. 2008;19(1):9-15.
- DOI: https://doi.org/10.3338/kjc.2008.19.1.9
- 3,099 View
- 18 Download
-
Abstract
PDF
- The major categories of neuroendocrine tumors of lung are typical carcinoid, atypical carcinoid, large cell neuroendocrine carcinoma, and small cell carcinoma. The histologic classification criteria of neuroendocrine tumors are well documented in the "WHO Classification of Tumors" based on mitotic figures and necrosis. Cytologic characteristics of neuroendocrine tumors are trabecular, acinar, and solid arrangement of tumor cells and occasional rosette formation. Nuclear chromatin patterns are characteristically described as "salt and pepper chromatin pattern". Many of cytologic classifications documented in the literature are before the "WHO Classification". In this review, the cytologic features of pulmonary neuroendocrine tumors are documented according to the WHO classification, and recent concepts of neuroendocrine tumors of lung are discussed.
- Gastric Collision Tumor (Adenocarcinoma and Neuro-endocrine Carcinoma): A Report of Two Cases.
- Ho Sung Park, Ja Myoung Chung, Woo Sung Moon, Myoung Jae Kang, Dong Geun Lee
- Korean J Pathol. 2001;35(1):76-79.
- 2,712 View
- 17 Download
-
Abstract
PDF
- Concurrence of adenocarcinoma and neuroendocrine carcinoma in the gastrointestinal tract has rarely been observed. We report two cases of gastric collision tumors (adenocarcinoma and neuroendocrine carcinoma) that developed in a 64-year-old man and a 71-year-old man. In both cases, there was a single ulcerative lesion in the stomach. Histologically, the gastric lesions were composed of two discrete lesions: tubular adenocarcinoma at the edge of an ulcer and neuroendocrine carcinoma in the ulcer base. We will discuss collision and composite tumors.
- Large Cell Neuroendocrine Carcinoma of the Lung 2 cases including one presented as an ovarian mass.
- Yun Jung Kim, Jung Weon Shim, Hye Kyung Ahn, Young Euy Park
- Korean J Pathol. 1997;31(3):257-262.
- 2,375 View
- 12 Download
-
Abstract
PDF
- Pulmonary tumors exhibiting neuroendocrine differentiation are classified as typical carcinoid, atypical carcinoid, and small cell lung carcinoma(SCLC). Travis et al. proposed a fourth category of large cell neuroendocrine carcinoma, which is characterized by light microscopic neuroendocrine appearance, cells of large size, polygonal shape, low nuclear cytoplasmic ratio, coarse nuclear chromatin, with prominent nucleoli high mitotic rate and frequent necrosis; and neuroendocrine features by immunohistochemistry or electron microscopy. High grade neuroendocrine carcinoma (LCAC-NE) revealed aggressive clinical course. We report two cases of neuroendocrine tumors of the lung characterized by a trabecular pattern of large pleomorphic cells with frequent mitoses and wide necrosis. The frequent metastatic sites of atypical carcinoid were liver, bone and brain. One of our case is presented, at first, as an ovarian mass, which shows multifocal rosettes and revealed metastasis from lung. Both cases expressed neuroendocrine differentiation by light microscopy and immunohistochemistry. However clinical neuroendocrine symptom were not present.
- Large Cell Neuroendocrine Carcinoma of the Lung: Report of three cases.
- Jai Hyang Go, Sun Ree Jung, Dong Hwan Shin, Woo Hee Jung
- Korean J Pathol. 1995;29(4):511-516.
- 2,302 View
- 12 Download
-
Abstract
PDF
- We report three cases of neuroendocrine tumors of the lung characterized by large pleomorphic cell with frequent mitosis, which show neuroendocrine differentiation by both light microscopy or electron microscopy and iminunohistochemistry. These tumors have been categorized as large cell neuroendocrine carcinoma by Travis et al.(1991) in contrast with non-small cell lung cancer with neuroendocrine differentiation. In the latter, neuroendocrine differentiation is not evident by light microscopy and must be demonstrated by imunohistochemstry or by electron microscopy. The prognosis of large cell neuroendocrine carcinoma, together with non-small cell lung cancer with neuroendocrine differentiation, appears to be worse than cancer without neuroendocrine differentiation and intermediate between atypical carcinoid and small cell lung cancer. Larger numbers of patients will be needed to demonstrate significant differences in survival.
- Neuroendocrine Differentiation in Adrenal Cortical Tumor of Chidhood: A case report.
- Sang Yong Song, Seung Sook Lee, Na Hye Myung, Je G Chi
- Korean J Pathol. 1993;27(2):175-180.
- 2,104 View
- 14 Download
-
Abstract
PDF
- Although neuroendocrine differentiation is a characteristic feature of tumors of the adrenal medulla, cortical tumors may also rarely be differentiated into medullary element. Recently we experienced such a case of adrenal cortical tumor having features of both cortical and medullary tumor. The patient was an 11-year-old girl who was incidentally found to have a left adrenal mass. Laboratory results showed elevated serum cortisol, aldosterone, renin, and epinephrine with high excretion of urinary metanephrine. Urine vanillyl mandelic acid and 17-ketosteroid remained within normal limits. Histologic featuresof a 6 cm round yellowish tumor were ambiguous to decide the orgin of this neoplasm. Cortical element predominated in the tumor with minor areas of pheochromocytomatous feature. Immunohistochemically, the tumor cells were positive for vimentin, neuron specific enolase, and epithelial membrane antigen. Ultrastructural examination revealed scattered membrane bound dense core granules in the tumor cells of medullary differentiation, measuring 150~500 nm in average diameter. Cortical tumor element showed corresponding ultrastructural features. These results indicate that this is a case of adrenal cortical tumor with features of neuroendocrine differentiation.
- Carcinoid Tumor of the Uterine Cercix: A light and electron microscopic study of two cases.
- Moon Hyang Park, Jung Dal Lee, Yoon Young Hwang
- Korean J Pathol. 1990;24(1):70-76.
- 2,205 View
- 12 Download
-
Abstract
PDF
- Two cases of carcinoid tumor of the uterine cervix were reported with emphasis on the histologic, cytologic, histochemical and electron microscopic appearance of tumor cells. Based on the light microscopic findings, one case was a well differentiated carcinoid with acinus formation, and the other was a poorly differentiated anaplastic type, being composed of small cells similar to those of oat cell carcinoma of the lung. Both tumors demonstrated scattered argyrophilic cells on Grimelius stain, and contained neurosecretory granules on electron microscopy. They were in stages II b and IV, respectively, at the time of presentation. The latter patient was treated with vinblastin, platinol and bleomycin, but died in 9 months after the initial diagnosis. The former was lost to follow-up study. Importance of distinction between this highly malignant tumor and other varieties of cervical cancer was emphasized.
- Pulmonary Adenocarcinoma of Fetal Type: Report of a case.
- Nam Hoon Cho, Kwang Gil Lee
- Korean J Pathol. 1990;24(3):287-293.
- 2,692 View
- 30 Download
-
Abstract
PDF
- Pulmonary adenocarcinoma of fetal type is a very uncommon tumor of the lung which simulates an early stage of lung differentiation. This is a primitive appearing epithelial tumor similar to the epithelial component of pulmonary blastoma but lacking the sarcomatous features. Since the report of Kradin et al, 8 more cases have been reported by a variety of name. These tumors are composed of glycogen-rich, non-ciliated tubular epithelial cells forming irregularly shaped tubules or arranged in a papillary pattern. A very remarkable findings of this tumor is the presence of endocrine cells which is confirmed by argyrophilia, immunohistochemistry or electron microscopy. We experienced a case of this tumor which showed hepatocytoid differentiation in addition to the characteristic histologic findings. Immunohistochemical studies performed on a resected tumor tissue showed immunoreactivity for alpha-fetoprotein, neuron-specific enolase and somatostatin, and endocrine type granules were found ultrastructurally. Although this tumor seems to have a relation with pulmonary blastoma in its histology, immunohistochemistry and ontogeny, a distinction between these should be attained because the average survival of the former group is longer as 23 months, while that of the latter is only 4 months.
- Neuroendocrine Carcinoma of the Gallbladder Arising as Double Tumor.
- Dae Hyun Baek, Seong Ki Min, Jin Man Kim, Kwang Sun Suh, Dae Young Kang
- Korean J Pathol. 1990;24(3):299-303.
- 2,197 View
- 12 Download
-
Abstract
PDF
- Pleomorphic (undifferentated) carcinoma is a rare histologic type of carcinomas of the gallbladder and an atypical carcinoid is thought to be an intermediated type between carcinoid tumor and small cell carcinoma. Dense core "neurosecretory" granules can be found in the above mentioned tumors. We experienced a case of a double tumor of the gallbladder in a 51-year old male patient. Grossly, a large solid mass, about 5.0 cm in diameter, was found in the fundic portion and the neck portion also had a small 1.5 cm-sized polypoid mass. Microscopically, these lesions had features of pleomorphic carcinoma and atypical carcinoid, respectively. Immunohistochemically, they manifested reactivity for neuron specific enolase. Ultrastructural study revealed neurosecretory granules in the cytoplasms of tumor cells of the fundic and neck masses. Although light microscopic features of these tumor masses are quite different, we consider that these tumors represent a spectrum of neuroendocrine differentiation.
- Urinary Cytologic Findings of Small Cell Neuroendocrine Carcinoma: A Case Report.
- Dong Hoon Kim, Dong Wook Kang, Kyung Hee Kim, Ju Heon Kim, Mee Ja Park
- J Pathol Transl Med. 2002;13(2):78-83.
- 2,261 View
- 20 Download
-
Abstract
PDF
- We report the cytologic features of a case of primary small cell carcinoma of the urinary bladder with high grade transitional cell and signet ring cell carcinomatous components. A 64-year-old male presented with gross hematuria for one week. Computed tomography revealed an ill-defined mass in the left lateral wall of the urinary bladder. Urinary cytology showed hypercellularity with predominantly isolated single cells and clustered cells. They have scanty cytoplasm and naked hyperchromatic nuclei with finely granular nuclear chromatin and rare nucleoli. The tumor cells occurred predominantly singe cells, but a few in clusters. Nuclear molding was prominent. No glandular formation or nesting was noted. The second tumor cells had high nuclear/cytoplasmic ratio, irregular nuclear membrane, and coarse granular chromatin. The background was inflamed and necrotic. The histologic findings of transurethral resection were mainly composed of small cell carcinoma, and partly transitional cell and signet ring cell carcinomatous components. Small cell neuroendocrine carcinoma have distinctive cytologic features to make a proper diagnosis.
- Merkel Cell Carcinoma: A case report associated with squamous cell carcinoma.
- Chang Hun Lee, Gyeong Yeob Gong, Kang Suek Suh, Sun Kyung Lee
- Korean J Pathol. 1991;25(2):164-171.
- 2,411 View
- 20 Download
-
Abstract
PDF
- Merkel cell carcinoma is a relatively uncommon, cutaneous, neuroendocrine neoplasm that was first recognized by Toker in 1972. Occasionally it is found concurrent with squamous cell carcinoma or basal cell carcinoma and in them cases, the coexistence of them is suggesive of presenting the effect of a common carcinogenic influence on two distinct precursor cells. Now the authors report a case of Merkel cell carcinoma associated with squamous cell carcinoma arising in the overlying epidermis, and a brief review of literatures is introduced. The patient was a 75-year-old female, who had noticed a reddish brown, ulcerated mass on the right buttock. It had progressively enlarged to become lemon-size during last 4 months. The right buttock mass excised measured 10x8x3 cm and was gray white, solid, with an ill-defined marigin. Histologically the tumor was located in the dermis and was lacking in connection with the epidermis in which invasive squamous cell carcinoma developed. The neoplastic cells were arranged in a diffuse, lymphoma-like pattern or trabecular arrangement and their cytologic details were reminiscent of small cell carcinoma of the lung, On electron microscopy the cells displayed many neurosecretory granules averaging about 100nm in diameter, intermediate filaments and desmosomes. Immunohistochemically a ball-like immunostaining for keratin, resembling an inclusion body, was seen, but other markers, including neuron-specific enolase, vimentin, S-100 protein and leukocyte common antigen, were unrewarded.
- The Prognostic Significance of Neuroendocrine Differentiation for Treating Prostatic Carcinoma in 699 Cases of Radical Prostatectomy.
- Tae Hoon Kang, Eun Shin, Baek Hee Kim, Gheeyoung Choe
- Korean J Pathol. 2008;42(6):381-388.
- 2,522 View
- 27 Download
-
Abstract
PDF
- BACKGROUND
Neuroendocrine differentiation of prostatic carcinoma is known to be associated with a poor prognosis, tumor progression and androgen-independency, and there is currently no successful therapy for this type of tumor. The purpose of this study is to evaluate the prognostic implications of neuroendocrine differentiation in prostatic carcinoma in Korean men. METHODS: Six hundreds and ninety nine consecutive cases of radical prostatectomy specimens were systematically processed for topographic mapping. Neuroendocrine differentiation was detected by immunohistochemistry by using antibody to chromogranin. We analyzed the relationship between neuroendocrine differentiation and the clinicopathological prognostic factors, as well as biochemical failure. The neuroendocrine differentiation was evaluated according to the presence of chromogranin-positive cells, the pattern of neuroendocrine cells and the number of neuroendocrine cells, respectively.
RESULTS
Neuroendocrine differentiation was detected in 150 out of 699 cases (21.5%). The presence of neuroendocrine differentiation as well as the pattern of neuroendocrine cells was correlated with biochemical failure and the other clinicopathological prognostic factors such as the Gleason score, the pathologic stage, the tumor volume, angiolymphatic invasion, perineural invasion, and the Ki-67 proliferative index (p<0.05). CONCLUSIONS: We suggest that neuroendocrine differentiation of prostatic carcinoma is a prognostic factor even in radical prostatectomy specimens for localized prostate cancer. Evaluation of the presence of neuroendocrine differentiation as well as the pattern of neuroendocrine cells is recommended in radical prostatectomy specimens.
- Uterine Cervical Large Cell Neuroendocrine Carcinoma Concurrent with High Grade Squamous Intraepithelial Neoplasia: A Case Report.
- Yun Kyung Kang, Jae Whoan Koh
- Korean J Pathol. 2008;42(6):389-392.
- 2,396 View
- 21 Download
-
Abstract
PDF
- Large cell neuroendocrine carcinoma (LCNEC) of the uterine cervix is a rare and aggressive malignancy. We report a case of uterine cervical LCNEC concurrent with high grade squamous intraepithelial neoplasia (HG-SIN). The LCNEC expressed chromogranin A and thyroid transcription factor 1 (TTF1). The HG-SIN was negative for these markers. Human papillomavirus (HPV) type 18 was positive in LCNEC whereas both type 16 and 18 were positive in HG-SIN by nested polymerase chain reaction. This case showed TTF1 positivity nonetheless diagnosed as a primary uterine cervical LCNEC confirmed by the detection of HPV genome within the tumor. It is critical to recognize LCNEC of the uterine cervix even in the small biopsy specimen because it is a distinctive clinicopathological entity with highly aggressive behavior and unfavorable outcome.
- Immunohistochemical Analysis of Insular Carcinoma of the Thyroid Gland.
- Hye Sook Min, Jin Ho Paik, Kyoung Bun Lee, Seong Hoe Park, Doo Hyun Chung
- Korean J Pathol. 2005;39(5):326-331.
- 3,095 View
- 43 Download
-
Abstract
PDF
- BACKGROUND
Insular thyroid carcinoma (ITC) is a relatively infrequent thyroid carcinoma that has distinctive histologic features. ITC shows an aggressive clinical course and the predominant presence of an insular component, which has been reported to be an independent factor of a poor prognosis. We retrospectively examined clinical details of the nine ITC patients, which represented 9 years of experience with ITC, and investigated the expressions of variable neuroendocrine and other immunohistochemical markers associated with well-differentiated thyroid carcinomas.
METHODS
We adopted an immunohistochemical approach and studied the expressions of synaptophysin, chromogranin A, CD56, NSE, S-100, RET, PPARgamma, calcitonin, galectin-3, and thyroglobulin in formalin-fixed, paraffin embedded tissue array slides of the 9 ITC patients, and investigated clinical features. Seven cases of follicular carcinoma and 4 cases of medullary carcinoma were also included as controls.
RESULTS
ITCs were positive for synaptophysin (44%, 4/9), CD56 (11%, 1/9), NSE (89%, 8/9), S100 (67%, 6/9), calcitonin (22%, 2/9), galectin-3 (78%, 7/9), and thyroglobulin (100%, 9/9), but completely negative for chromogranin A, RET, and PPARgamma.
CONCLUSION
ITCs express neuroendocrine markers in variable proportions and appear not to be associated with the oncoproteins of conventional thyroid carcinomas. Notably, its differential diagnosis from medullary carcinoma is required in cases showing focal calcitonin positivity.
- Immunohistochemical Study of Primary Large Cell Undifferentiated Carcinoma of the Lung.
- Hye Seung Han, Jeong Wook Seo, Eui Keun Ham
- Korean J Pathol. 1996;30(5):417-426.
- 2,455 View
- 26 Download
-
Abstract
PDF
- We performed a histopathologic and immunohistochemical study of 23 cases of surgically resected large cell undifferentiated carcinoma(LCUC) of the lung. The relative incidence of LCUC was 7.6% among the total resected cases of primary lung cancer over 7 years(1987-1993). The mean age of the patients was 56 years and 21 cases were male. The mean size of the mass was 5 cm and 11 cases were located peripherally. According to the histologic features, LCUC could be divided into three groups: squamous cell carcinoma-like(6 cases), adenocarcinoma-like(13 cases), and small cell carcinoma-like(4 cases) groups. The histologic differences were related to the variations of the immunohistochemical properties, but there were no differences in prognosis among these groups. Immunoreactivity to cytokeratin(CAM 5.2) was demonstrated in 22/23(96%). Carcinoembryonic antigen was positive in 13/23(57%). Neuron specific enolase and chromogranin were positive in 11/23(48%) and 5/23(22%), respectively. Vimentin was seen in 11/23(48%). From these observations, we could subclassify them by their immunologic phenotypes; exocrine features in 6/23(26%), neuroendocrine(NE) features in 4/23(17%), both exocrine and NE phenotypes in 7/23(30%), and 6 cases(26%) showed neither phenotype. The group with NE features showed a worse prognosis(P<0.05) and immunoreactivity for vimentin was also related to a worse prognosis(P<0.05). These findings imply that the immunohistochemical properties of LCUC are closely related to the histopathologic features. The groups, subdivided by histology and immunoreactivity, showed no prognostic difference except for the NE differentiation and reaction for vimentin.
- Immunohistochemical Expression of Neuron Specific Enolase-Positive Cells in Gastric Adenocarcinomas.
- Ghee Young Choe, Yong Il Kim
- Korean J Pathol. 1991;25(4):291-304.
- 2,144 View
- 13 Download
-
Abstract
PDF
- In order to correlate the frequency of neuroendocrine cells with pathologic parameters in gastric adenocarcinomas, immunoperoxidase staining for neuron specific enolase was performed on 250 consecutive cases of surgically resected gastric adenocarcinomas(201 advanced gastric carcinomas[AGCs], 49 early gastric carcinomas[EGCs] and 2 cases of gastric carcinoid tumors. Of the 252 cases of gastric carcinomas, pure exocrine carcinomas were 174 cases(69%), pure neuroendocrine(NE) carcinomas 2 cases(0.8%), mixed exocrine and NE carcinomas 32 cases(12.7%), and exocrine carcinomas with occasional NE cells 44 cases(17.5%). The frequency of gastric carcinomas with NSE-positive cells increased with age proportionally. NSE positivity was higher in polypoid or fungating tumors(AGC Borrmann type I, II, EGC I and IIa) than ulcerative or scirrhous tumors. There was no significant difference in frequency of NSE-positive cells by histologic type and differentiation of gastric adenocarcinomas. The above findings reflect that most gastric carcinomas are heterogeneous in their constituents and suggest that both exocrine and neuroendocrine carcinomas are the expression of the extreme ends of the exocrine-endocrine differentiation spectrum based on the assumption that they develop from the pluripotent stem cells differentiating into both exocrine endocrine carcinomas.
- Gastrointestinal Adenomatous Polyposis Associated with Small Cell Neuroendocrine Carcinoma of the Rectosigmoid: A case report.
- Wan Seop Kim, Eun Kyung Hong, Kang Sik Kim, Kwang Soo Lee, Jung Dal Lee
- Korean J Pathol. 1996;30(11):1040-1044.
- 2,154 View
- 16 Download
-
Abstract
PDF
- In adenomatous polyposis coli there are many colonic and extracolonic manifestations, and various combinations of these induce different clinical presentations and syndromes. We experienced a unique case of adenomatous polyposis of the large intestine and stomach in a 39-year-old man. In the colon, small cell neuroendocrine carcinoma rather than adenocarcinoma had developed, which did not contain adenomatous or carcinomatous foci. The adenomatous polyps in the colon were all small and sessile with no cancerous or precancerous change two years after the resection of the symptomatic gastric adenomas, even though the gastric adenomas were larger and showed dysplastic change. We think this case is another variant of adenomatous polyposis syndrome.
- The Clinicopathological Characteristics of Gastrointestinal Neuroendocrine Tumors; An Analysis of 65 Cases.
- Hyunjoo Lee, Jungwoo Choi, Jung Suk An, Hyunchul Kim, Bong Kyung Shin, Aeree Kim, Hankyeom Kim, Insun Kim
- Korean J Pathol. 2007;41(3):149-157.
- 2,519 View
- 27 Download
-
Abstract
PDF
- Background
: This study was designed to investigate gastrointestinal neuroendocrine tumors with an emphasis on their clinicopathological characteristics.
Methods
: Sixty-five cases were reviewed and classified as typical carcinoid (TC), atypical carcinoid (AC), large cell neuroendocrine carcinoma (LCNEC) and small cell carcinoma (SmCC). We performed immunohistochemistry to characterize the expression of the immunoreactivity for synaptophysin, chromogranin, gastrin, somatostatin, thyroid transcription factor-1, p53 and Ki-67.
Results
: Most commonly, the tumors were located in the rectum (54%), followed by the stomach (23%) and colon (9%). Histologically, the tumors were classified as 49 TCs, 4 ACs, 6 LCNECs and 6 SmCCs. Most tumors were stained positive for synaptophysin and/or chromogranin. Four LCNECs and one SmCC were p53-positive. The carcinoids revealed a low level (<5%) of reactivity for Ki-67, while > or =30% of the cells showed reactivity for Ki-67 in the majority of LCNECs and SmCCs. Six patients with metastatic carcinoids were older than those patients without metastasis (64 vs 48 years, respectively, p=0.004). Furthermore, the size of tumors was larger for the patients with metastatic carcinoids than for the patients with nonmetastatic carcinoids (2.3 vs 0.5 cm, respectively, p=0.005).
Conclusion
: Old age, large tumor size and muscle invasion are associated with high grade neuroendocrine tumor and lymph node metastasis for those patients with carcinoids.
 First
First Prev
Prev


