 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Articles
- Clinicopathological profile of high-grade differentiated thyroid carcinoma in Indonesian tertiary hospital
- Novita , Agnes Stephanie Harahap, Maria Francisca Ham, Alfianto Widiono, Chan Kwon Jung
- Received October 20, 2025 Accepted January 15, 2026 Published online April 23, 2026
- DOI: https://doi.org/10.4132/jptm.2026.01.15 [Epub ahead of print]
- 208 View
- 8 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background
High-grade differentiated thyroid carcinoma (HGDTC) is a recently recognized entity in the 2022 World Health Organization classification, representing a more aggressive subtype of differentiated thyroid carcinoma. Previously, high-grade features such as increased mitotic activity and tumor necrosis were often overlooked, despite being important independent prognostic factors. Although rare, HGDTC carries significant diagnostic, prognostic, and therapeutic implications. Data remain limited in Indonesia. Methods: This retrospective descriptive study reviewed 565 thyroid carcinoma cases diagnosed at Cipto Mangunkusumo Hospital from 2019 to 2024. Eleven cases (1.9%) met HGDTC criteria. Clinicopathological characteristics, histologic subtypes, Ki-67 proliferation index, molecular alterations, treatment modalities, and clinical outcomes were analyzed. Results: Patients had a mean age of 54.6 years, with a female-to-male ratio of 2.7:1. Papillary thyroid carcinoma was the main type (90.9%), with the tall cell subtype predominating. Mean tumor size was 6.4 cm. Lymphatic invasion, vascular invasion, and extrathyroidal extension were present in 54.5%, 18.2%, and 45.5% of cases, respectively. All tumors showed necrosis. Mean mitotic count was 3 per 2 mm². The Ki-67 index ranged from 5% to 45% (median, 14%). BRAFV600E and TERT promoter mutations were detected in 18.2% and 36.4% of cases, respectively, with co-mutations in 18.2%. Six cases (54.5%) had metastases at time of diagnosis. During a mean follow-up of 20.5 months, one patient (9.1%) developed new vertebral metastases and all patients (100%) remained alive. Conclusions: HGDTC presents with more aggressive characteristics and a worse prognosis. Accurate diagnosis, molecular profiling, and long-term monitoring are essential for optimal management.
- Lessons learned from the first 2 years of experience with thyroid core needle biopsy at an Indonesian national referral hospital
- Agnes Stephanie Harahap, Maria Francisca Ham, Retno Asti Werdhani, Erwin Danil Julian, Rafi Ilmansyah, Chloe Indira Arfelita Mangunkusumso, Tri Juli Edi Tarigan
- J Pathol Transl Med. 2025;59(3):149-160. Published online April 25, 2025
- DOI: https://doi.org/10.4132/jptm.2025.02.19

- 4,489 View
- 194 Download
-
Abstract
PDF
- Background
Core needle biopsy (CNB) improves diagnostic accuracy by providing precise tissue sampling for histopathological evaluation, overcoming the limitation of inconclusive fine-needle aspiration results. This study evaluated the diagnostic performance of CNB in assessing thyroid nodules, with additional analysis of the benefits of BRAF V600E and RAS Q61R immunohistochemical (IHC) markers.
Methods
This retrospective study enrolled patients with thyroid nodules who underwent CNB at Dr. Cipto Mangunkusumo Hospital, Jakarta, from July 2022 to July 2024. CNB diagnoses were classified using the Korean Thyroid Association Criteria. Diagnostic efficacy was evaluated for neoplastic and malignant lesions, both independently and with BRAF V600E and RAS Q61R IHC. The correlation between nodule size and postoperative diagnosis was also analyzed.
Results
A total of 338 thyroid nodule samples was included, and 52.7% were classified as CNB category II. In the 104 samples with postoperative diagnoses, category IV was the most prevalent (39.4%). CNB demonstrated a sensitivity of 74% and a specificity of 100% for neoplastic lesions and 23.8% sensitivity and 100% specificity for malignant lesions. Combining CNB with BRAF V600E and RAS Q1R IHC increased the sensitivity to 77% for neoplastic lesions and 28.8% for malignant lesions. Larger nodules (>3 cm) were significantly associated with neoplastic (p = .005) and malignant lesions (p = .004).
Conclusions
CNB performs well in identifying neoplastic lesions, with or without BRAF V600E and RAS Q61R IHC, but its low sensitivity for malignant lesions warrants caution. While CNB categories V–VI indicate malignancy, the possibility of malignancy in categories I–IV should not be overlooked.
Correspondence
- Erratum: Diagnostic challenges in the assessment of thyroid neoplasms using nuclear features and vascular and capsular invasion: a multi-center interobserver agreement study
- Agnes Stephanie Harahap, Mutiah Mutmainnah, Maria Francisca Ham, Dina Khoirunnisa, Abdillah Hasbi Assadyk, Husni Cangara, Aswiyanti Asri, Diah Prabawati Retnani, Fairuz Quzwain, Hasrayati Agustina, Hermawan Istiadi, Indri Windarti, Krisna Murti, Muhammad Takbir, Ni Made Mahastuti, Nila Kurniasari, Nungki Anggorowati, Pamela Abineno, Yulita Pundewi Setyorini, Kennichi Kakudo
- J Pathol Transl Med. 2025;59(3):201-201. Published online March 31, 2025
- DOI: https://doi.org/10.4132/jptm.2024.07.25.r
- Corrects: J Pathol Transl Med 2024;58(6):299
- 2,652 View
- 64 Download
Original Article
- Diagnostic challenges in the assessment of thyroid neoplasms using nuclear features and vascular and capsular invasion: a multi-center interobserver agreement study
- Agnes Stephanie Harahap, Mutiah Mutmainnah, Maria Francisca Ham, Dina Khoirunnisa, Abdillah Hasbi Assadyk, Husni Cangara, Aswiyanti Asri, Diah Prabawati Retnani, Fairuz Quzwain, Hasrayati Agustina, Hermawan Istiadi, Indri Windarti, Krisna Murti, Muhammad Takbir, Ni Made Mahastuti, Nila Kurniasari, Nungki Anggorowati, Pamela Abineno, Yulita Pundewi Setyorini, Kennichi Kakudo
- J Pathol Transl Med. 2024;58(6):299-309. Published online September 12, 2024
- DOI: https://doi.org/10.4132/jptm.2024.07.25
- Correction in: J Pathol Transl Med 2025;59(3):201
- 6,074 View
- 416 Download
- 1 Web of Science
- 1 Crossref
-
Abstract
PDFSupplementary Material
- Background
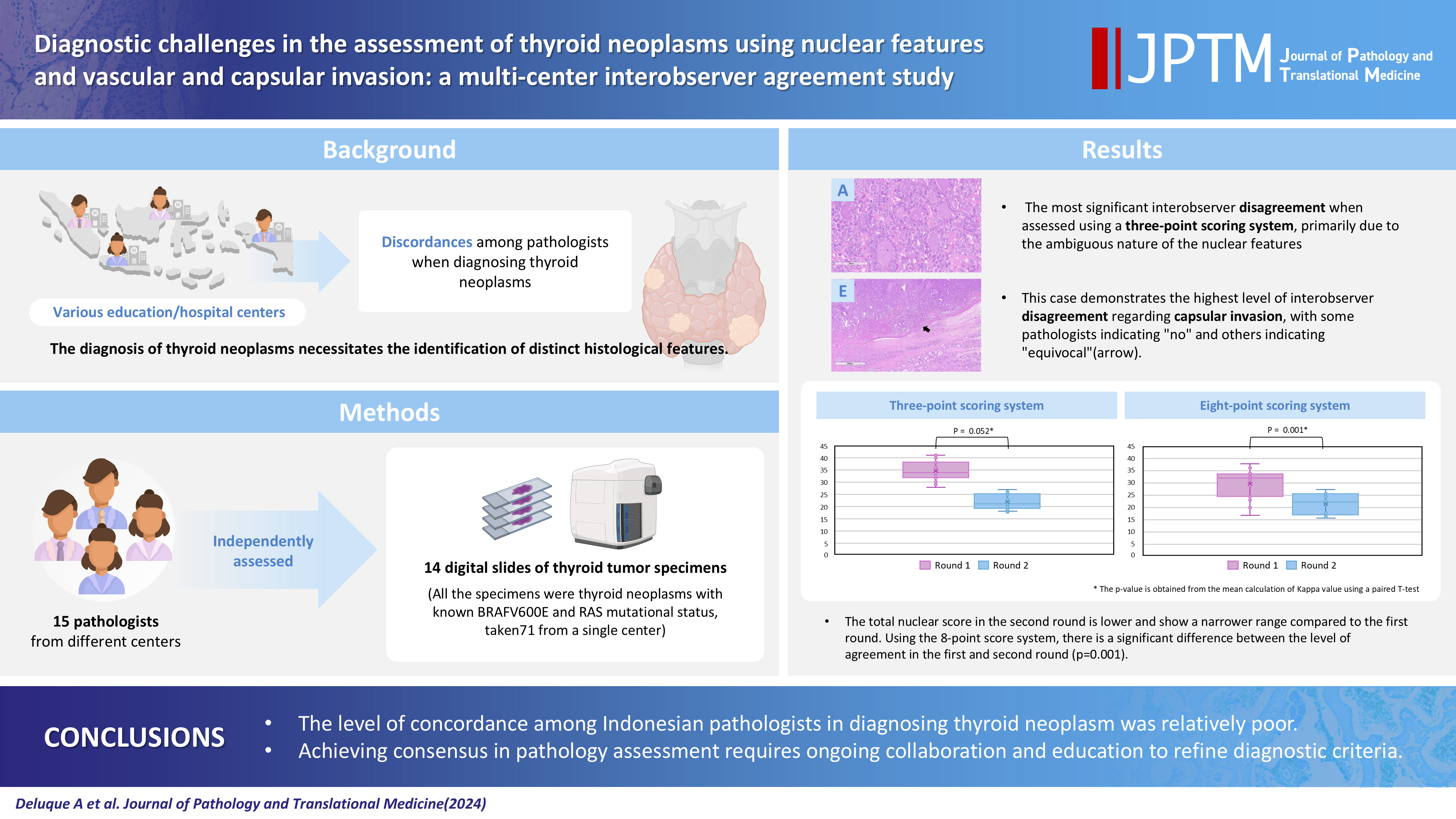
The diagnosis of thyroid neoplasms necessitates the identification of distinct histological features. Various education/hospital centers located in cities across Indonesia likely result in discordances among pathologists when diagnosing thyroid neoplasms.
Methods
This study examined the concordance among Indonesian pathologists in assessing nuclear features and capsular and vascular invasion of thyroid tumors. Fifteen pathologists from different centers independently assessed the same 14 digital slides of thyroid tumor specimens. All the specimens were thyroid neoplasms with known BRAFV600E and RAS mutational status, from a single center. We evaluated the pre- and post-training agreement using the Fleiss kappa. The significance of the training was evaluated using a paired T-test.
Results
Baseline agreement on nuclear features was slight to fair based on a 3-point scoring system (k = 0.14 to 0.28) and poor to fair based on an eight-point system (k = –0.02 to 0.24). Agreements on vascular (κ = 0.35) and capsular invasion (κ = 0.27) were fair, whereas the estimated molecular type showed substantial agreement (κ = 0.74). Following the training, agreement using the eight-point system significantly improved (p = 0.001).
Conclusions
The level of concordance among Indonesian pathologists in diagnosing thyroid neoplasm was relatively poor. Consensus in pathology assessment requires ongoing collaboration and education to refine diagnostic criteria. -
Citations
Citations to this article as recorded by
- Nuclear pseudoinclusion is associated with BRAFV600E mutation: Analysis of nuclear features in papillary thyroid carcinoma
Agnes Stephanie Harahap, Dina Khoirunnisa, Salinah, Maria Francisca Ham
Annals of Diagnostic Pathology.2025; 75: 152434. CrossRef
- Nuclear pseudoinclusion is associated with BRAFV600E mutation: Analysis of nuclear features in papillary thyroid carcinoma
 First
First Prev
Prev


