 E-submission
E-submission
Search
- Page Path
- HOME > Search
Case Study
- Intravascular NK/T-cell lymphoma: a case report and literature review
- Ji Min Na, Wookjae Jung, Minhye Kim, Yun-Hong Cheon, Jong Sil Lee, Dae Hyun Song, Jung Wook Yang
- J Pathol Transl Med. 2023;57(6):332-336. Published online November 14, 2023
- DOI: https://doi.org/10.4132/jptm.2023.10.30
- 7,536 View
- 240 Download
- 5 Web of Science
- 6 Crossref
-
 Abstract
Abstract
 PDF
PDF - Intravascular lymphoma is characterized by an exclusively intravascular distribution of tumor cells. Intravascular natural killer/T-cell lymphoma (IVNKTL) is extremely rare, highly aggressive, commonly Epstein-Barr virus (EBV)–positive, and predominantly affects the skin and central nervous system. Here we report a case of IVNKTL diagnosed in a 67-year-old female, presenting with persistent intermittent fever and skin rashes throughout the body. Incisional biopsy of an erythematous lesion on the chest exhibited aggregation of medium to large-sized atypical lymphoid cells confined to the lumen of small vessels that were positive for CD3, granzyme B, and CD56 on immunohistochemistry and EBV-encoded RNA in situ hybridization. EBV DNA was also detected in serum after diagnosis. With a review of 26 cases of IVNKTL to date, we suggest that active biopsy based on EBV DNA detection may facilitate early diagnosis of IVNKTL.
-
Citations
Citations to this article as recorded by
- Mimicry in the vasculature: a review of diagnostic clues in cutaneous intravascular lymphoid proliferations
MA Faraz, S Tu Zahra, F Ocampo-Gonzalez, SC Shalin, Aadil Ahmed
Diagnostic Histopathology.2026; 32(3): 155. CrossRef - Intravascular Lymphoma Associated with the Female Genital Tract—Diagnostic Considerations, Therapeutic Approaches, and Outcomes
Aleksandar Ristic, Marija Rovcanin, Ana Tomic, Aleksandar Rakic, Nebojsa Zecevic, Svetlana Jankovic
Diseases.2026; 14(3): 109. CrossRef - Adequacy of Single Random Skin Biopsy With Subcutaneous Sampling for the Diagnosis of Intravascular Lymphoma
Phitsinee Purngpiputtrakul, Panitta Sitthinamsuwan, Sanya Sukpanichnant, Penvadee Pattanaprichakul, Manasmon Chairatchaneeboon, Yingyong Chinthammitr, Pochamana Phisalprapa
Journal of Cutaneous Pathology.2026; 53(8): 731. CrossRef - Intravascular Lymphoma: A Unique Pattern Underlying a Protean Disease
Mario Della Mura, Joana Sorino, Filippo Emanuele Angiuli, Gerardo Cazzato, Francesco Gaudio, Giuseppe Ingravallo
Cancers.2025; 17(14): 2355. CrossRef - Cutaneous Intravascular Hematolymphoid Entities: A Review
Emily Hatheway Marshall, Bethany Brumbaugh, Allison Holt, Steven T. Chen, Mai P. Hoang
Diagnostics.2024; 14(7): 679. CrossRef - CD30- and CD56-positive atypical intravascular lymphocytes of the uterine cervix, mimicking intravascular lymphoma: A case report and review of the literature
Daisuke Yamashita, Munemichi Otani, Hayato Maruoka, Takuya Aoki, Shigeo Hara
Journal of Clinical and Experimental Hematopathology.2024; 64(4): 328. CrossRef
- Mimicry in the vasculature: a review of diagnostic clues in cutaneous intravascular lymphoid proliferations
Review
- Lymphoproliferative disorder involving body fluid: diagnostic approaches and roles of ancillary studies
- Jiwon Koh, Sun Ah Shin, Ji Ae Lee, Yoon Kyung Jeon
- J Pathol Transl Med. 2022;56(4):173-186. Published online July 4, 2022
- DOI: https://doi.org/10.4132/jptm.2022.05.16
- 14,786 View
- 339 Download
- 6 Web of Science
- 7 Crossref
-
Abstract
PDF
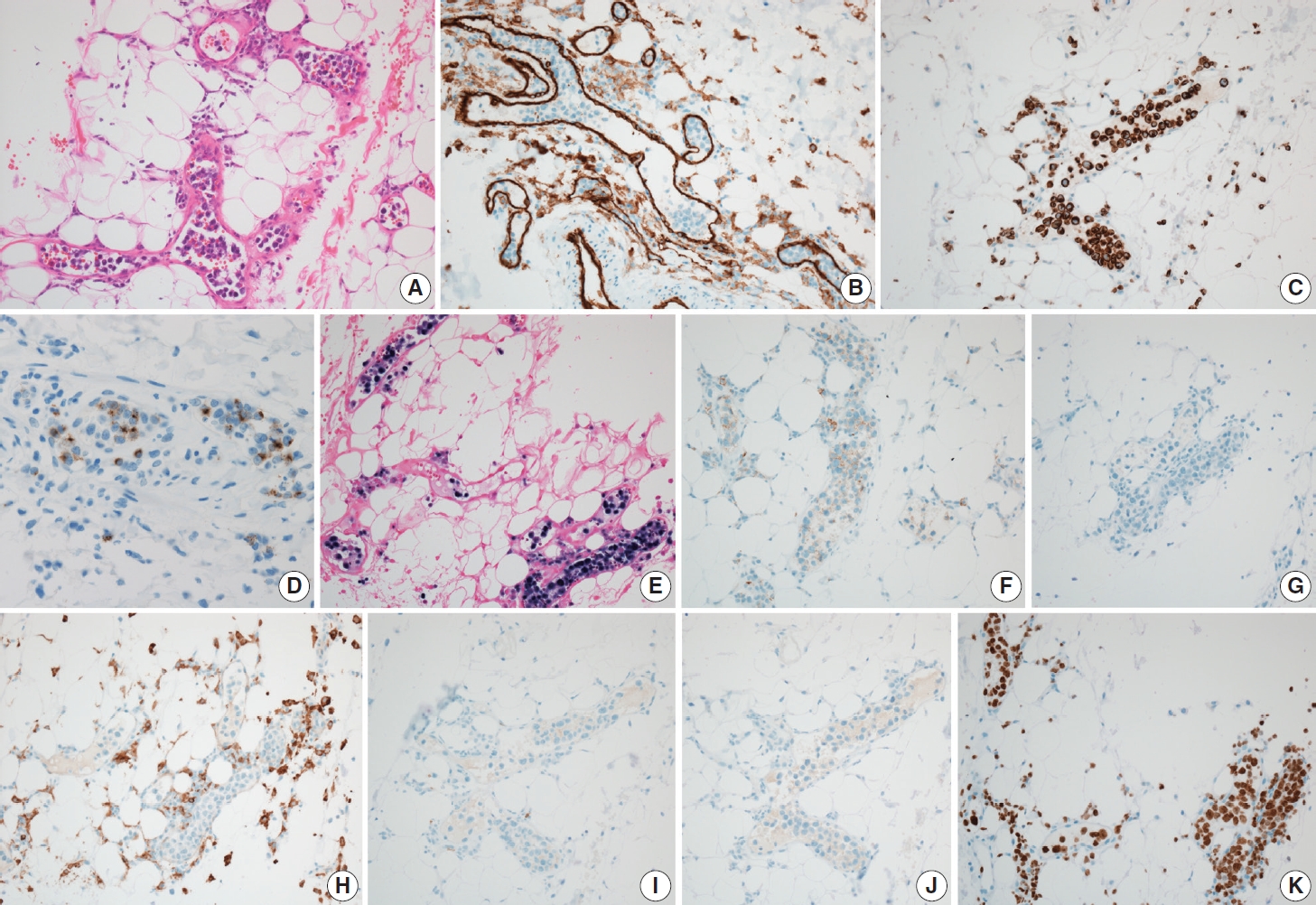
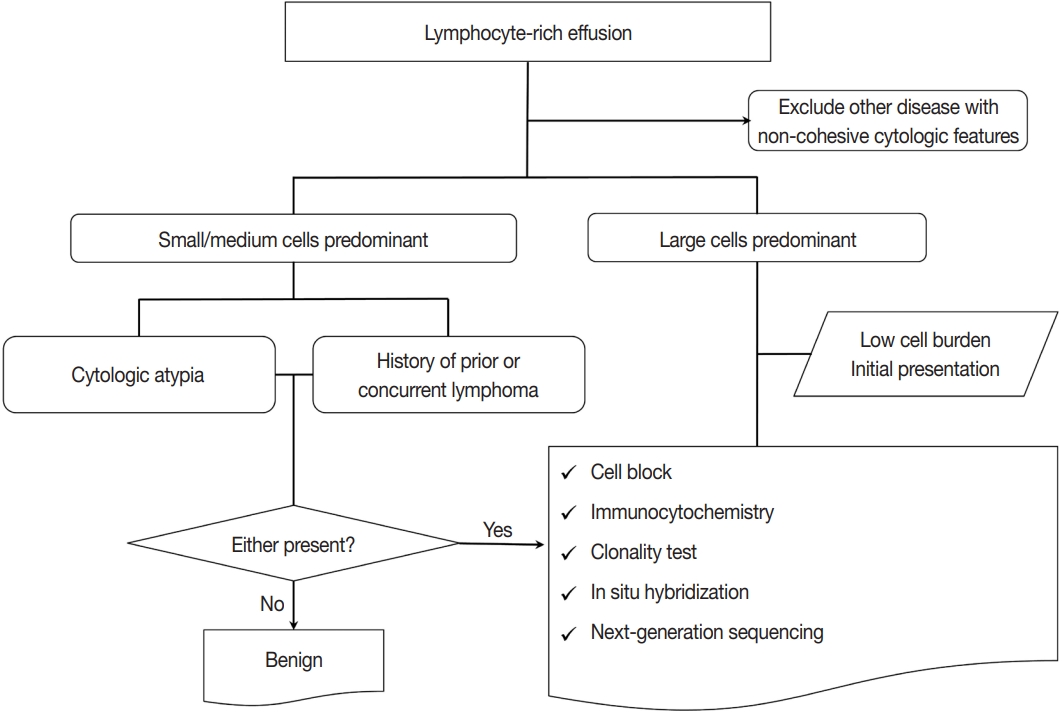
- Lymphocyte-rich effusions represent benign reactive process or neoplastic condition. Involvement of lymphoproliferative disease in body cavity is not uncommon, and it often causes diagnostic challenge. In this review, we suggest a practical diagnostic approach toward lymphocyte-rich effusions, share representative cases, and discuss the utility of ancillary tests. Cytomorphologic features favoring neoplastic condition include high cellularity, cellular atypia/pleomorphism, monomorphic cell population, and frequent apoptosis, whereas lack of atypia, polymorphic cell population, and predominance of small T cells usually represent benign reactive process. Involvement of non-hematolymphoid malignant cells in body fluid should be ruled out first, followed by categorization of the samples into either small/medium-sized cell dominant or large-sized cell dominant fluid. Small/medium-sized cell dominant effusions require ancillary tests when either cellular atypia or history/clinical suspicion of lymphoproliferative disease is present. Large-sized cell dominant effusions usually suggest neoplastic condition, however, in the settings of initial presentation or low overall cellularity, ancillary studies are helpful for more clarification. Ancillary tests including immunocytochemistry, in situ hybridization, clonality test, and next-generation sequencing can be performed using cytologic preparations. Throughout the diagnostic process, proper review of clinical history, cytomorphologic examination, and application of adequate ancillary tests are key elements for successful diagnosis.
-
Citations
Citations to this article as recorded by- Fluid Overload-Associated Large B-Cell Lymphoma Presenting as Isolated Pleural Effusion
Kevin Leeper, Lauren Borecky, Mojtaba Akhtari, Jun Wang
Hematology Reports.2026; 18(1): 13. CrossRef - Cytopathologic Diagnosis of Lymphomas in Serous Effusions, Cerebrospinal and Vitreous Fluid
Pamela Michelow, Liezel Coetzee, Rubina Razack
Acta Cytologica.2026; : 1. CrossRef - Diffuse Large B-Cell Lymphoma Masquerading as Recurrent Pleural Effusion and Melena: A Case Report and Literature Review
Priyal Mehta, Smitesh Padte, Udaya Kumar Damodaran, Aparna Parvathaneni, Jeffrey Scott, George Abraham
Cureus.2026;[Epub] CrossRef - The case of the sneaky lymphoma: solved by flow cytometry
Renu Singh, Md Ali Osama, Rachana Meena, Shailaja Shukla, Jagdish Chandra
Indian Journal of Thoracic and Cardiovascular Surgery.2025; 41(9): 1258. CrossRef - The urgency of Burkitt lymphoma diagnosis in fluid cytology—A tertiary care experience
Soundarya Ravi, Anu K. Devi, Prabhu Manivannan, Debasis Gochhait, Rakhee Kar, Neelaiah Siddaraju
Cytopathology.2024; 35(2): 275. CrossRef - Immunocytochemistry on frozen-embedded cell block for the diagnosis of hematolymphoid cytology specimen: a straightforward alternative to the conventional cell block
Youjeong Seo, Sanzida Alam Prome, Lucia Kim, Jee Young Han, Joon Mee Kim, Suk Jin Choi
Journal of Hematopathology.2024; 17(1): 1. CrossRef - Lymphoma presenting as the first finding in pleural fluid cytology: A rare cytologic presentation
Kafil Akhtar, Gowthami Nagendhran, Anjum Ara, Masheera Akhtar
IP Archives of Cytology and Histopathology Research.2024; 8(4): 250. CrossRef
- Fluid Overload-Associated Large B-Cell Lymphoma Presenting as Isolated Pleural Effusion
Original Article
- Clinicopathologic implication of PD-L1 gene alteration in primary adrenal diffuse large B cell lymphoma
- Ki Rim Lee, Jiwon Koh, Yoon Kyung Jeon, Hyun Jung Kwon, Jeong-Ok Lee, Jin Ho Paik
- J Pathol Transl Med. 2022;56(1):32-39. Published online November 16, 2021
- DOI: https://doi.org/10.4132/jptm.2021.10.05
- 6,548 View
- 170 Download
- 2 Web of Science
- 1 Crossref
-
Abstract
PDF
- Background
Primary adrenal (PA) diffuse large B cell lymphoma (DLBCL) was previously reported as an aggressive subset of DLBCL, but its genetic features were not sufficiently characterized. From our previous study of DLBCL with programmed death-ligand 1 (PD-L1) gene alterations, we focused on PD-L1 gene alterations in PA-DLBCL with clinicopathologic implications.
Methods
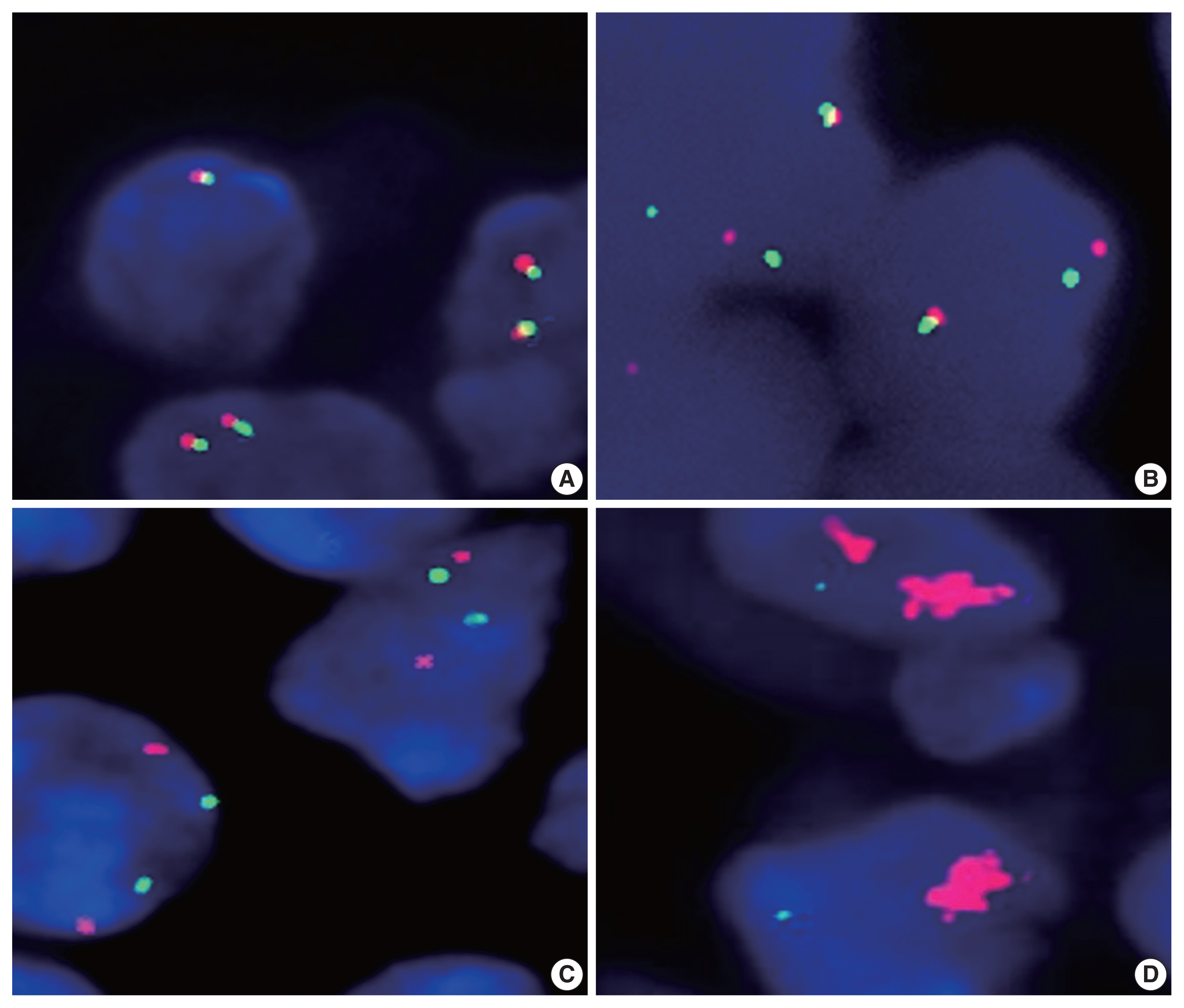
We performed fluorescence in situ hybridization for PD-L1 gene translocation and amplification in PA-DLBCL (n = 18) and comparatively analyzed clinicopathologic characteristics with systemic non-adrenal (NA)-DLBCL (n = 90).
Results
PA-DLBCL harbored distinctive features (vs. NADLBCL), including high international prognostic index score (3–5) (72% [13/18] vs. 38% [34/90], p = .007), poor Eastern Cooperative Oncology Group performance score (≥ 2) (47% [7/15] vs. 11% [10/90], p = .003), elevated serum lactate dehydrogenase (LDH) (78% [14/18] vs. 51% [44/87], p = .035) and MUM1 expression (87% [13/15] vs. 60% [54/90], p = .047). Moreover, PA-DLBCL showed frequent PD-L1 gene alterations (vs. NA-DLBCL) (39% [7/18] vs. 6% [5/86], p = .001), including translocation (22% [4/18] vs. 3% [3/87], p = .016) and amplification (17% [3/18] vs. 2% [2/87], p = .034). Within the PA-DLBCL group, PD-L1 gene–altered cases (vs. non-altered cases) tended to have B symptoms (p = .145) and elevated LDH (p = .119) but less frequent bulky disease (≥ 10 cm) (p = .119). In the survival analysis, PA-DLBCL had a poor prognosis for overall survival (OS) and progression-free survival (PFS) (vs. NA-DLBCL; p = .014 and p = .004). Within the PA-DLBCL group, PD-L1 translocation was associated with shorter OS and PFS (p < .001 and p = .012).
Conclusions
PA-DLBCL is a clinically aggressive and distinct subset of DLBCL with frequent PD-L1 gene alterations. PD-L1 gene translocation was associated with poor prognosis in PA-DLBCL. -
Citations
Citations to this article as recorded by- Case Report: Diagnostic value of spectral CT in primary adrenal lymphoma
Xiang Zhuang, Xi xi Jin, Li wen Feng, Hui Zhang
Frontiers in Oncology.2026;[Epub] CrossRef
- Case Report: Diagnostic value of spectral CT in primary adrenal lymphoma
Case Study
- Morphologic variant of follicular lymphoma reminiscent of hyaline-vascular Castleman disease
- Jiwon Koh, Yoon Kyung Jeon
- J Pathol Transl Med. 2020;54(3):253-257. Published online February 5, 2020
- DOI: https://doi.org/10.4132/jptm.2019.12.17
- 9,395 View
- 243 Download
- 5 Web of Science
- 4 Crossref
-
Abstract
PDF
- Follicular lymphoma (FL) with hyaline-vascular Castleman disease (FL-HVCD)-like features is a rare morphologic variant, with fewer than 20 cases in the literature. Herein, we report a case of FL-HVCD in a 37-year-old female who presented with isolated neck lymph node enlargement. The excised lymph node showed features reminiscent of HVCD, including regressed germinal centers (GCs) surrounded by onion skin-like mantle zones, lollipop lesions composed of hyalinized blood vessels penetrating into regressed GCs, and hyalinized interfollicular stroma. In addition, focal areas of abnormally conglomerated GCs composed of homogeneous, small centrocytes with strong BCL2, CD10, and BCL6 expression were observed, indicating partial involvement of the FL. Several other lymphoid follicles showed features of in situ follicular neoplasia. Based on the observations, a diagnosis of FL-HVCD was made. Although FLHVCD is very rare, the possibility of this variant should be considered in cases resembling CD. Identification of abnormal, neoplastic follicles and ancillary immunostaining are helpful for proper diagnosis.
-
Citations
Citations to this article as recorded by- Unicentric Castleman Disease: Illustration of Its Morphologic Spectrum and Review of the Differential Diagnosis
Siba El Hussein, Andrew G. Evans, Hong Fang, Wei Wang, L. Jeffrey Medeiros
Archives of Pathology & Laboratory Medicine.2024; 148(1): 99. CrossRef - Finding a Needle in the Haystack
Hung-Yu Lin, Yi-Jen Peng, Yi-Ying Wu, Ping-Ying Chang
Journal of Medical Sciences.2023; 43(6): 292. CrossRef - Analysis of immunophenotypic features in hyaline vascular type Castleman disease
Yu Chang, Yu Ma, Chen Chang, Wensheng Li
Diagnostic Pathology.2023;[Epub] CrossRef - In‐situ follicular neoplasia: a clinicopathological spectrum
Gurdip S Tamber, Myriam Chévarie‐Davis, Margaret Warner, Chantal Séguin, Carole Caron, René P Michel
Histopathology.2021; 79(6): 1072. CrossRef
- Unicentric Castleman Disease: Illustration of Its Morphologic Spectrum and Review of the Differential Diagnosis
Review
- Molecular Testing of Lymphoproliferative Disorders: Current Status and Perspectives
- Yoon Kyung Jeon, Sun Och Yoon, Jin Ho Paik, Young A Kim, Bong Kyung Shin, Hyun-Jung Kim, Hee Jeong Cha, Ji Eun Kim, Jooryung Huh, Young-Hyeh Ko
- J Pathol Transl Med. 2017;51(3):224-241. Published online May 10, 2017
- DOI: https://doi.org/10.4132/jptm.2017.04.09
- 24,946 View
- 729 Download
- 14 Web of Science
- 17 Crossref
-
Abstract
PDF
- Molecular pathologic testing plays an important role for the diagnosis, prognostication and decision of treatment strategy in lymphoproliferative disease. Here, we briefly review the molecular tests currently used for lymphoproliferative disease and those which will be implicated in clinical practice in the near future. Specifically, this guideline addresses the clonality test for B- and T-cell proliferative lesions, molecular cytogenetic tests for malignant lymphoma, determination of cell-of-origin in diffuse large B-cell lymphoma, and molecular genetic alterations incorporated in the 2016 revision of the World Health Organization classification of lymphoid neoplasms. Finally, a new perspective on the next-generation sequencing for diagnostic, prognostic, and therapeutic purpose in malignant lymphoma will be summarized.
-
Citations
Citations to this article as recorded by- Pediatric lymphoproliferative disorders – Emerging insights and management: A narrative review
Emmanuel Ifeanyi Obeagu
Medicine.2026; 105(4): e47367. CrossRef - Case series of mycosis fungoides with clinical features suggestive of seborrheic dermatitis
Alexa C. Kwang, Kacie R. Carlson, Christine J. Ko, Michael Girardi
JAAD Case Reports.2026;[Epub] CrossRef - Presence of minimal residual disease determined by next-generation sequencing is not a reliable prognostic biomarker in children with acute lymphoblastic leukemia
Elizabeta Krstevska Bozhinovikj, Nadica Matevska-Geshkovska, Marija Staninova Stojovska, Emilija Gjorgievska, Aleksandra Jovanovska, Nevenka Ridova, Irina Panovska Stavridis, Svetlana Kocheva, Aleksandar Dimovski
Leukemia & Lymphoma.2025; 66(6): 1121. CrossRef - Haematogenous seeding in mycosis fungoides and Sézary syndrome: current evidence and clinical implications
Robert Gniadecki, Emmanuella Guenova, Christiane Querfeld, Jan P Nicolay, Julia Scarisbrick, Lubomir Sokol
British Journal of Dermatology.2025; 192(3): 381. CrossRef - Exploring External Quality Control Methods for PCR–Polyacrylamide Gel Electrophoresis–Based Lymphocyte Receptor Gene Rearrangement Assays in Korea
Jieun Kim, Ho Hyun Song, Soobin Chae, GeonWoo Choi, Jeong Won Shin
Journal of Laboratory Medicine and Quality Assurance.2025; 47(2): 43. CrossRef - Laboratory analysis of 182 cases of B-cell lymphoproliferative disorders other than typical chronic lymphocytic leukemia: Single-center study
Shams Salah Mahdi, Nuha Abd Ali Al-Sarai
Iraqi Journal of Hematology.2025; 14(2): 218. CrossRef - Assessment of Bone Marrow Involvement in B‐Cell non‐Hodgkin Lymphoma Using Immunoglobulin Gene Rearrangement Analysis with Next‐Generation Sequencing
Min Ji Jeon, Eun Sang Yu, Dae Sik Kim, Chul Won Choi, Ha Nui Kim, Jung Ah Kwon, Soo‐Young Yoon, Jung Yoon
Journal of Clinical Laboratory Analysis.2024;[Epub] CrossRef - Thymus and lung mucosa-associated lymphoid tissue lymphoma with adenocarcinoma of the lung: a case report and literature review
Yu Pang, Daosheng Li, Yiqian Chen, Qinqin Liu, Yuheng Wu, Qingliang Teng, Yuyu Liu
World Journal of Surgical Oncology.2023;[Epub] CrossRef - Development and implementation of an automated and highly accurate reporting process for NGS-based clonality testing
Sean T. Glenn, Phillip M. Galbo, Jesse D. Luce, Kiersten Marie Miles, Prashant K. Singh, Manuel J. Glynias, Carl Morrison
Oncotarget.2023; 14(1): 450. CrossRef - A comparison of capillary electrophoresis and next-generation sequencing in the detection of immunoglobulin heavy chain H and light chain κ gene rearrangements in the diagnosis of classic hodgkin’s lymphoma
Juan-Juan Zhang, Yu-Xin Xie, Li-Lin Luo, Xuan-Tao Yang, Yi-Xing Wang, Yue Cao, Zheng-Bo Long, Wan-Pu Wang
Bioengineered.2022; 13(3): 5868. CrossRef - Lymphoproliferative disorder involving body fluid: diagnostic approaches and roles of ancillary studies
Jiwon Koh, Sun Ah Shin, Ji Ae Lee, Yoon Kyung Jeon
Journal of Pathology and Translational Medicine.2022; 56(4): 173. CrossRef - Diagnostic Workup of Primary Cutaneous B Cell Lymphomas: A Clinician's Approach
Giulia Tadiotto Cicogna, Martina Ferranti, Mauro Alaibac
Frontiers in Oncology.2020;[Epub] CrossRef - Kappa and lambda immunohistochemistry and in situ hybridization in the evaluation of atypical cutaneous lymphoid infiltrates
Alexandra C. Hristov, Nneka I. Comfere, Claudia I. Vidal, Uma Sundram
Journal of Cutaneous Pathology.2020; 47(11): 1103. CrossRef - Primary lung mucosa-associated lymphoid tissue lymphoma accompanied by multiple sclerosis
Ke-Ke Yu, Lei Zhu, Ji-Kai Zhao, Rui-Ying Zhao, Yu-Chen Han
Chinese Medical Journal.2019; 132(13): 1625. CrossRef - Diagnostic accuracy of SOX11 immunohistochemistry in mantle cell lymphoma: A meta-analysis
Woojoo Lee, Eun Shin, Bo-Hyung Kim, Hyunchul Kim, Riccardo Dolcetti
PLOS ONE.2019; 14(11): e0225096. CrossRef - Views of dermatopathologists about clonality assays in the diagnosis of cutaneous T‐cell and B‐cell lymphoproliferative disorders
Nneka Comfere, Uma Sundram, Maria Yadira Hurley, Brian Swick
Journal of Cutaneous Pathology.2018; 45(1): 39. CrossRef - A Next-Generation Sequencing Primer—How Does It Work and What Can It Do?
Yuriy O. Alekseyev, Roghayeh Fazeli, Shi Yang, Raveen Basran, Thomas Maher, Nancy S. Miller, Daniel Remick
Academic Pathology.2018; 5: 2374289518766521. CrossRef
- Pediatric lymphoproliferative disorders – Emerging insights and management: A narrative review
Original Article
- Polymorphic Reticulosis.
- Duck Hwan Kim, Jin Hee Sohn, Sung Suk Paeng, Kyung Ha Kang, Jung Il Suh
- Korean J Pathol. 1995;29(3):296-302.
- 3,091 View
- 22 Download
-
Abstract
PDF
- Polymorphic reticulosis(PMR) is a unique clinicopathological entity of unknown etiology, which commonly present as an aggressive, necrotizing lesion of the upper respiratory tract. It is a separate nosologic entity from Wegener's granulomatosis and idiopathic mildine destructive disease. The origin of the cells composing polymorphic reticulosis has been controversial. We reviewed 15 cases of polymorphic reticulosis with respect to clinical and histologic bases, and immunohistochemical studies were done using UCHLI (CD45RO), as a T cell marker, CD-20 as a B cell marker and alpha- I -antichymotrypsin as a histiocytic marker. Almost all cases showed characteristic histologic and immunohistochemical features similar to those of peripheral T cell lymphoma. Thus, this study indidcated that polymorphic reticulosis is a type of malignant lymphoma of T cell lineage.
Case Reports
- Non-Hodgkin's Lymphoma of the Uterine Cervix: 3 cases report.
- Chan Pil Park, Young Hyeh Ko, Jung Dal Lee, Moon Il Park, Kyung Tai Kim, Sam Hyun Cho
- Korean J Pathol. 1995;29(3):368-373.
- 2,546 View
- 20 Download
-
Abstract
PDF
- Three patients with primary non-Hodgkin's lymphoma of the uterine cervix are reported and the literature is reviewed. All the three patients in the current study presented with vaginal bleeding. They were found to have diffuse large cleaved cell lymphoma, one of which was multilobated variant with marked sclerosis. Histologically, differential diagnsis from undifferentiated small cell carcinoma, endometrial stromal sarcoma & other sarcomas was difficult and requires special stains including immunobistochemical study. Vaginal pap smears were diagnosed as 'class V; malignant lymphoma' in only one patient. Immunologically, two cases were beta-cell lineage and one case was T-cell lineage. All the patients were treated with chemotherapy only and showed good responses.
- A Case of Malignant Lymphoma Misdiagnosed as Focal Lymphoid Hyperplasia in the Esophagus.
- Sook Keum Chung, Young Hyeh Ko, Chan Keum Park, Jung Dal Lee
- Korean J Pathol. 1995;29(3):393-398.
- 2,782 View
- 31 Download
-
Abstract
PDF
- Esophageal involvement by malignant lymphoma is extremely rare. A case of follicular lymphoma of the esophagus, misdiagnosed as focal lymphoid hyperplasia (pseudolymphoma) in a 72-year-old man is presented. The esophagogram revealed diffuse narrowing of the lumen in the middle and distal portion without ulceration. The resected esophagus showed mural thickening without any remarkable mucosal change. Microscopically, the esophagus showed scattered follicular lymphoid aggregates in the submucosa, extending into periadventitial fat tissue. Most follicles were devoid of germinal center and consisted of loosely aggregated small cleaved cells without atypia. The surrounding stroma of the submucosa showed dense fibrosis entrapping the infiltrating small lymphocytes in a "indian-file" appearance. There were some reactive follicles with germinal center. In the lamina propria, many plasma cells and a few eosinophils were infiltrated. The gene rearrangement study showed rearranged band for Jk probe which confirmed monoclonal B-cell nature of infiltrated small lymphoid cells. The small cleaved lymphocytes arranged in follicles were positive for L26 and bcl-2 protein. This case demonstrated the necessity of immunophenotypic and gene rearrangement study in the diagnosis of pseudolymphoma in the digestive tract.
Original Articles
- Application of Gene Rearrangement Analysis for Diagnosis of Malignant Lymphoma.
- Kyung Soo Kim, Chan Choi
- Korean J Pathol. 1995;29(4):415-422.
- 2,303 View
- 14 Download
-
Abstract
PDF
- To evaluate the utility of gene rearrangement analysis, eight cases of malignant lymphoma, one case of Hodgkin's disease, two cases of angioiminunoblastic lymphadenopathy (AILD) and two cases of non-specific lymphadenitis were studied by immunohistochemical and genetic analysis. Southern blot analysis was perfon-ned by a using vacuum transfer system and a biotin labelled probe. This method was faster, safer, and more convenient than conventional methods. Gene rearrangement study showed rearranged novel bands in five of six cases of B cell lymphoma, in all cases of T cell lymphoma, and in all cases of AILD. No rearrangement of the B cell receptor(BCR) or of the T cell receptor(TCR) was seen in Hodgkin's disease or in nonspecific lymphadenitis. These results suggest that gene rearrangement analysis of BCR and TCR is a recommended method for the diagnosis of clonality in lymphoproliferative disorders. It would allow pathologists to differentiate lymphoma from polyclonal lymphoid proliferation and to provide information for cell lineage.
- Lymphoproliferativ Lesions of the Orbit and Conjunctiva: Histopathologic Study on 20 cases including 5 cases analyzed by Immunophenotyping.
- Chul Woo Kim, Na Hye Myong, Je G Chi
- Korean J Pathol. 1993;27(2):152-163.
- 2,331 View
- 16 Download
-
Abstract
PDF
- Lymphoid lesions of the orbit and conjunctiva may be divided histologically into three groups: monomorphous and cytologically atypical malignant lymphomas, benign reactive follicular hyperplasia or inflammatory pseudotumor, and borderline lymphoid lesions mainly composed of small, non-atypical lymphocytes with or without evidence of plasmacytic differentiation or germinal centers which are difficult to clarify its nature by histologic criteria alone. From 1984 to 1992 at Seoul National University Hospital, 20 cases of orbital lymphoid infiltrates were reviewed to find out histopathologic characteristics of malignant lymphomas and try to classify them properly. Also, we sought histologic findings helpful for differential diagnosis between malignant and borderline cases. Histologic examination of malignant lesions usually revealed the features of low-grade B cell lymphomas of mucosa-associated lymphoid tissue(MALT) origin, which predominantly consist of centrocyte-like(CCL) cells. Among 13 primary orbital lymphomas, six cases were classified as MALT lymphomas of Isaacson, six were more apt to be the type of immunocytoma by kiel classification, and remaining one showed mixed pattern of both types in areas. The one case of malignant lymphoma with diffuse large cell type was confirmed by secondary involvement of intestinal lymphoma. Five cases were confirmed by immunoglobulin k-light chain monoclonality on flow cytometry and immunofluorescence study. The histologic findings such as Dutcher bodies, hemosiderin, deposits and polykaryocytes tended to be more frequently encountered in malignant lymphoma rather than indeterminate lesions and were thought to be helpful ones in making differential diagnosis between malignant and benign lesions. With above findings, we assume that the principal neoplastic cells in the low grade lymphoma arising in the orbit and conjunctiva are CCL cells, which might be originated from the localized memory B cells, and also several kinds of B lymphocytes in on-going differentiation stages such as medium-sized monocytoid B cell, lymphoplasmacytoid cell, plasma cell, and mature small lymphocyte also contribute to the tumor progression.
Case Report
- Non-Hodgkin's Malignant Lymphoma Arising in the Appendix: A case report.
- Yun Sin Kim, Mi Sook Lee, Kwang Seok Lee Lee, Sung Chul Lim, Ho Jong Jeon
- Korean J Pathol. 1995;29(4):524-526.
- 2,299 View
- 20 Download
-
Abstract
PDF
- Primary malignant lymphoma of the appendix is an unconnnon neoplasm although the gastrointestinal tract is the most common extranodal site of malignant lymphoma. We report a case of primary malignant lymphoma of the appendix in a 54-year-old male, who presented with pain in the right lower abdomen. An appendectomy was performed. The appendix measured 9.5 cm in length and 5.5 cm in diameter. Cut sections showed a solitary circumferential mass in the appendiceal lumen. Light microscopic features were compatible with malignant lymphoma of diffuse large cell type(Working Formulation) and the immunophenotype was B cell type.
Original Article
- Morphometric Analysis of Malignant Lymphoma.
- In Sook Kim, Eun Kyung Hong, Jong Dal Lee
- Korean J Pathol. 1990;24(2):128-136.
- 2,205 View
- 15 Download
-
Abstract
PDF
- Nuclear morphology and size are important in the diagnosis and classification of non-Hodgkin's lymphoma. The recognition of morphologic features of the lymphoma cells and their interpretation are somewhat subjective and often difficult. We apply the morphometric study in touch imprints from 22 cases of non-Hodgkin's lymphoma classified by Working formulation. Determination of the exact size of the tumor cells and substantial diagnostic value of this method compared with histology are proposed. Morphometric parameters, including nuclear area, perimeter, maximal diameter (D-max), diameter of an equivalent circle for a measured area (D-circle), circularity factor (From PE) and regularity factor (Form AR) are measured, using Kontron, user-controlled image analyser (IBAS-1). The correlation between morphometric and histologic diagnosis is relatively good, except for 2 cases of Burkitt's lymphoma, measured as large cell and 2 cases of large cell lymphoma measured as medium cell. The most reliable parameter of the nuclear size is D-circle. The parameters for the nuclear shape, Form PE and Form AR, also reflect the nuclear cleavage and polymorphous pattern. The large cell group shows more wide standard deviation than small and medium cell groups, reflecting heterogeneity and variability in unclear size of large cell group. We suggests the morphometric analysis using touch imprints is complementary diagnostic tool for more accurate and reproducible diagnosis.
Case Report
- Fine Needle Aspiration Cytology of Primary Malignant Lymphoma of the Thyroid Gland: A Case Report.
- Mi Seon Kwon, Seung Sook Lee, Jae Soo Koh, Jin Haeng Chung, Kyo Young Lee
- J Pathol Transl Med. 2001;12(1):67-71.
- 2,493 View
- 10 Download
-
Abstract
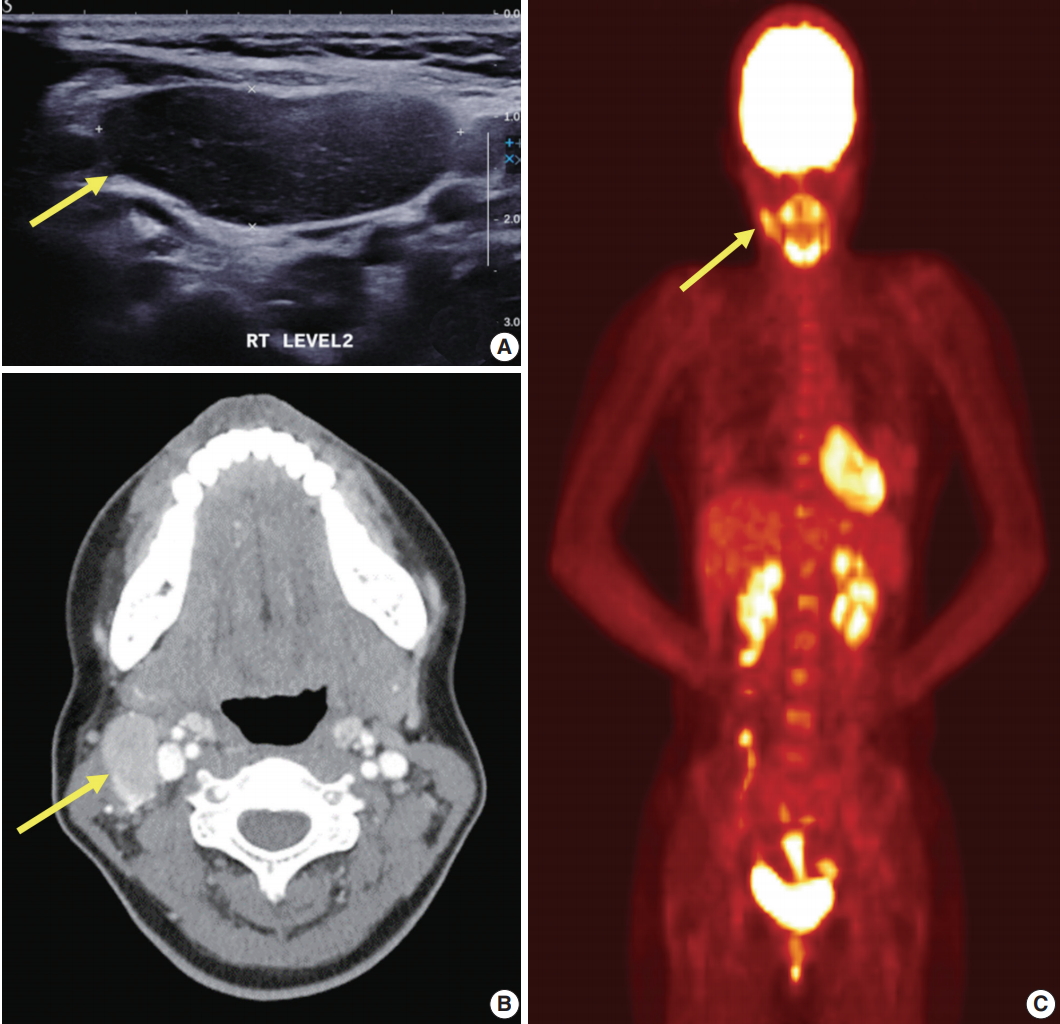
- Primary malignant lymphoma of the thyroid gland is uncommon malignancies. Its fine needle aspiration cytology (FNAC) findings are rarely described in the literature. This article highlights the FNAC diagnosis of primary malignant lymphoma of the thyroid gland. A 70-year-old female presented with a rapidly enlarging thyroid mass of five months' duration. FNAC smears showed low cellularity consisting of predominantly atypical enlarged lymphoid cells admixed with a few small lymphocytes, plasma cells, and oncocytic cells. Some disrupted lymphoid cells were also present. The tumor cells infiltrated into the thyroid follicular epithelium forming lymphoepithelial lesion. The cytologic appearance showed a diffuse mixture of cell types with only a few small, mature lymphocytes and many enlarged lymphoid cells. The enlarged lymphoid cells were atypical and pleomorphic with nuclear clefting and irregularities. Grossly, the left lobe of the thyroid was nearly replaced by a diffuse firm to soft solid mass with smooth tan fish-flesh homogeneous cut surface. Histological diagnosis was diffuse large B-cell lymphoma with areas of marginal zone B-cell lymphoma of MALT type.
Original Articles
- Sinusoidal Involvement of Malinant Lymphoma in Lymph Nodes Simulating Metastatic Carcinoma.
- Young Seak Kim, Mi Kyung Shin, In Sun Kim
- Korean J Pathol. 1991;25(1):45-49.
- 2,446 View
- 23 Download
-
Abstract
PDF
- We present a case of this distinctive variety of malignant lymphoma, which was diagnosed in the axillary lymph nodes of a 66-year-old woman. The patient was admitted to the GS department due to palpable mass on the right axillary area for two months. A 2 x 1 cm sized mass was also palpated on the cervical area. The laboratory and radiologic findings were unremarkable. Axillary dissection was done under the impression of metastatic carcinoma from breast. Received lymph nodes were multiple and variable in size, ranging from 0.5 cm to 5.0 cm in diameter. Histologically, the lymph nodes were partly effaced and involved by nodular and diffuse infiltrations of large lymphoid cells in the subcapsular and medullary sinuses. In diffuse areas, typical starry-sky pattern was seen. Immunohistochemically, the tumor cells were negative for broad-spectrum keratin, but positive for leukocyte antigen, ML, and B cell markers, L26, and 4KB5. T cell marker. UCHL1 was negative. On staining with histiocytic marker, Mac387 antibody, the tingible-body macrophages were only positive. Interstitial plasma cells and some of the tumor cells were positive for lambda light chain. Electron microscopic study, which was done on paraffin embedded tissue showed lymphoid-type of nuclei without cellular junction suggestive for carcinoma.
- Primary MALT(mucosa-associated lymphoid tissue) Type Lymphoma of the Liver.
- Do Youn Park, Jee Yeon Kim, Hyo Jeong Chae, Jin Sook Lee, Chang Hun Lee, Mee Young Sol, Kang Suek Suh, Sun Kyung Lee
- Korean J Pathol. 1997;31(12):1317-1319.
- 2,330 View
- 13 Download
-
Abstract
PDF
- Primary non-Hodgkin' lymphomas of the liver, an organ normally devoid of a native lymphoid tissue, are very rare. We recently experienced a case of a primary low-grade hepatic B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) type in a 36-year-old woman. The ultrasonography revealed a 5 cm sized mass in the right lobe of the liver. A right segmentectomy of the liver was done and showed a relatively well-circumscribed brownish yellow lobulated homogenous mass, measuring 5.5x4.5 cm in size. Histologic sections of liver mass revealed large lymphoid follicles with reactive germinal centers, follicular colonization by centrocyte-like cells (CCL cells), and lymphoepithelial lesions. The CCL cells were positive for B-cell (CD20), LCA (CD45RA), Bcl-2 oncoprotein, and lambda light chain.
Case Report
- Fine Needle Aspiration Cytology of Primay Malignant Lymphoma of the Breast: A Case Report.
- Hyun Joong Kim, Kyung Hwa Lee, Jo Heon Kim, Min Keun Shim, Ji Shin Lee, Chan Choi
- J Pathol Transl Med. 2004;15(2):112-115.
- 2,304 View
- 20 Download
-
Abstract
PDF
- Lymphoproliferative disorders, manifesting either as a primary lesion or as part of a generalized process, rarely involve the breast. The primary malignant lymphoma of the breast is rare. The cytologic features of this neoplasm have not been reported in Korea thus far. We described a case of primary malignant lymphoma of the breast, as diagnosed by fine needle aspiration cytology (FNAC) in an 84-year-old female. FNAC smears showed high cellularity. The main cytologic feature observed was a carpeting of monotonous, atypical, enlarged lymphoid cells. These lymphocytes showed relatively round elliptical nuclei with some indentation. One or more prominent nucleoli were seen. Biopy from the breast mass revealed diagnostic features of non-Hodgkin's lymphoma, diffuse large B-cell type.
Original Articles
- Histopathologic Study of Primary Gastrointestinal Lymphoma: Gross and immunohistochemical analysis of 30 cases.
- Hye Jae Cho, Jeong Eun Joo, Ill Hyang Ko
- Korean J Pathol. 1994;28(2):118-125.
- 2,180 View
- 25 Download
-
Abstract
PDF
- A histopathologic study including iramunohistochemical stains was made in 30 patients who were presented with gastrointestinal lymphoma. The occurrence was 13 in the stomach, 8 in the ileocecum, 7 in the small intestine and 2 in the colon. The disease more frequently affected males than females and the average ages were 53 years in the patients of gastric lymphoma and 44 years in the patients of intestinal lymphoma. Gastric lymphomas were usually presented with a single lesion, and the antrum and/or body were the most common sites. But intestinal lymphomas were presented with a single or multiple lesion, and the ileocecum was the most common site. The most common gross type of gastrointestinal lymphomas was the ulceroinfiltrating type and most are of the diffuse large noncleaved cell type of B-cell lymphoma, histologically. There were 2 cases of T-cell lymphoma presented in the intestine as the superficially ulcerative gross pattern and diffuse immunoblastic cell type. The distinct MALToma was seen in only one case of stomach but the feature was partially remained in each two cases of stomach and intestine. Their coexistent findings may suggest that diffuse large of immunoblastic component arises through blastic transformation of the low-grade M ALToma component.
- Histopathologic Analysis of Malignant Lymphoma Involving the Skin and Its Relationship with the Epstein-Barr Virus.
- Yun Hee Jin, Seong Ho Kim, Chan Kum Park
- Korean J Pathol. 2000;34(1):20-28.
- 2,176 View
- 13 Download
-
Abstract
PDF
- The author classified 38 cases of malignant lymphoma involving the skin primarily or secondarily by the new WHO classification with minor modifications and carried out RNA in situ hybridization and/or polymerase chain reaction (PCR) to investigate the role of Epstein-Barr virus (EBV). A case was follicular lymphoma of B cell origin and 37 cases were malignant lymphomas of T cell origin, including 15 cases of Mycosis fungoides/Sezary syndrome, five cases of subcutaneous panniculitis-like T cell lymphomas, a case of anaplastic large cell lymphoma, and four cases of primary cutaneous CD30 T cell lymphoproliferative disorders. There were eight cases of unspecified peripheral T cell lymphomas, in which four cases were composed of medium-sized cells, three cases of large cells, and a case of lymphoepithelioid cells. Four cases of nasal and nasal type NK/T cell lymphomas and three cases of unspecified peripheral T cell lymphomas showed EBV genome. The nasal and nasal type NK/T cell lymphomas, especially those involving the nasal cavity, showed close association with the EBV infection.
Case Report
- Primary Malignant Lymphoma of the Liver: Report of a case.
- Soo Kyong Chung, Chang Suck Kang, Won Il Kim, Sang In Shim, Sun Moo Kim
- Korean J Pathol. 1987;21(4):285-290.
- 2,285 View
- 11 Download
-
Abstract
PDF
- Primary extranodal lymphoma of the liver is very rare, approximately thirty-one cases having been reported in the literature. We report one case of primary malignant lymphoma of the liver in a 26-year-old female, who was presented with palpable abdominal mass on the epigastrium for about 40 days. Laboratory findings revealed no specific abnormalities. Peripheral lymph nodes or spleen were not palpable. An abdominal ultrasonogram revealed a huge mass involving the entire left lobe of the liver. Left lateral segmentectomy of the liver was done. The resected lateral portion of left lobe of the liver showed a large solitary mass, 12 cm in the greatest dimension, with a yellowish gray fleshy solid cut surface. Though light microscopic feature was compatible with primary malignant lymphoma, diffuse large cell type, intermediate grade by the working formulation, undifferentiated carcinomas including hepatocellular carcinoma, plasmacytoma, and pleomorphic sarcomas could not be completely ruled out. Thus, marker studies and electron microscopic examination were performed. Immunoperoxidase stains for common leukocyte antigen was positive, and the Leder stain for myeloid granule was negative. Electron microscopic stuids revealed findings of neoplastic lymphoid cells, consistent with malignant lymphoma. Primary lymphoma of the liver has only rarely been reported, and its natural history is unclear. Many of the reported cases have been large cell lymphomas, as in this case.
Original Articles
- Detection of Minimal Lesion and Identification of Clonality in Malignant Lymphoma.
- Young Shin Kim, Chang Suk Kang, Kyun gja Han, Kyo Young Lee, Yong Goo Kim, Won Il Kim, Sang In Shim
- Korean J Pathol. 1998;32(4):298-308.
- 2,235 View
- 12 Download
-
Abstract
PDF
- The bone marrow biopsy is an integral part of the staging process in patients with malignant lymphomas. Bone marrow(BM) involvement indicates stage IV disease, but there are always a lot of cases in which clear separation is not possible when based on morphology alone. Additional difficulties are caused by morphologic discordance between the BM and the primary lymphoma. Immunohistochemical stain, mRNA in situ hybridization (ISH) for light chain restriction and polymerase chain reaction (PCR) for IgH CDR3 and TCRgamma were performed to find a minimal lesion and the clonality in formalin fixed paraffin embedded tissues of 39 primary lymphomas and corresponding BM biopsy specimens. As a result, nine morphologically negative bone marrows of 18 lymphomas were positive by PCR (Group I). Among the 6 lymphoma cases with morphologically suspicious BM involvement (Group II), one was confirmed to be positive for marrow involvement by both mRNA ISH and PCR and the other four by PCR alone. The positive bone marrows of Group I and II revealed gene rearrangement at the same site as the primary lesion, suggesting the same clonality. Thirteen of 15 lymphomas with morphologically positive BM (Group III) had the same clonality in the primary lymphomas and the BM lesion. Three cases among the Group III with morphologic discordance also revealed the same clonality by PCR. This study shows that a combination of mRNA ISH and PCR in addition to an immunohistochemical stain improves the diagnostic sensitivity in the detection of BM involvement and identification of clonality. Among the three different methods used, PCR is the most sensitive in detecting a minimal lesion.
- Expression of Matrix Metalloproteinase and Tissue Inhibitors of Matrix Metalloproteinase in Malignant Lymphoma.
- Ah Won Lee, An Hi Lee, Chang Suk Kang, Byung Kee Kim
- Korean J Pathol. 2000;34(4):249-256.
- 2,242 View
- 14 Download
-
Abstract
PDF
- Matrix metalloproteinases (MMPs) and their inhibitors (tissue inhibitors of matrix metalloproteinases, TIMPs) play essential roles in the remodelling of the extracellular matrix. The balance between MMPs and TIMPs is altered in neoplasia, contributing to the invasive and metastatic properties of malignant tumors. Although MMP and TIMP are believed to play an important role in invasion and metastasis in malignant solid tumors, little is known about their involvement in malignant lymphoma. Immunohistochemical stains for MMP-1, MMP-2, MMP-9, TIMP-1 and TIMP-2 were performed using 56 paraffin blocks of the malignant lymphoma and the results were analyzed by using the tumor grade by Working Formulation. The expression of MMP-9 was noted in 45.5% of low grade, 86.1% of intermediate grade, and 100% of high grade malignant lymphoma. The incidence of MMP-9 expression in tumor cells was positively correlated with the grade of the malignant lymphoma (P<0.025). In nodal lymphomas, the incidence of the MMP-9 expression of the tumor cells was higher in malignant lymphoma with extracapsular invasion than those without extracapsular invasion (P=0.008). The incidence of TIMP-1 expression in the tumor cells and fibroblasts was positively correlated with the grade of the malignant lymphoma (P<0.025). In nodal lymphoma, the incidence of the TIMP-1 expression of the tumor cells was higher in malignant lymphoma with extracapsular invasion than those without extracapsular invasion (P=0.009). The incidences of the MMP-1, MMP-2, and TIMP-2 expression in malignant lymphoma were neither increased in the malignant lymphoma with extracapsular tumor invasion nor correlated with the grade by working formulation. There was no significant difference in the expression rate of MMP-1, MMP-2, MMP-9, TIMP-1, and TIMP-2 in nodal- and extra-nodal malignant lymphoma. The above results suggest that the expressions of MMP-9 and TIMP-1 are positively correlated with the grade and the presence of extranodal tumor invasion in malignant lymphomas.
Case Reports
- Richer's Syndrome: Report of a case.
- Su Kyeong Yeon, Chang Sug Kang, Han Jin Lee, Dong Uk Kim, Chun Chu Kim, Sang In Shim
- Korean J Pathol. 1994;28(4):420-426.
- 2,168 View
- 12 Download
-
Abstract
PDF
- Richer's syndrome is a development of a high grade malignant lymphoma in a patient with preexisting chronic 1ymphocytic leukemia, small lymphocytic lymphoma or Waldenstrom's macroglobulinemia. A rare case of Richer's syndrome arising in the spleen of a 35-year-old-man was studied by morphology, immunohistochemistry and gene rearrangement study. He has had weight loss and night sweat for last 6 months. Hepatosplenomegaly and abdominal lymphadenopathy were noted on CT scanning. Especially an ovoid radiolucent mass was found within the image of splenomegaly. Lymph nodes and liver biopsy, bone marrow aspiration and splenectomy were done. In the lymph nodes, liver and bone marrow, well differentiated small lymphocytic infiltrations were found but, in the spleen, pleomorphic, large cells with occasional multinucleated giant cells formed a nodular mass surrounded by diffuse, extensive infiltration of small well differentiated lymphocytes. The two distinctive areas in the spleen had positive staining for B-cell marker (HLA-DR and L26), negative staining for T-cell marker (UCLH1), and positive staining for IgM heavy chain and kappa light chain by immuohistochemical study. so this case was diagnosed as a diffuse large cell 1ymphoma transformed from small lymphocytic lymphoma. We made an another effort to clarify their clonality. Gene rearrangement method usingcomplementarity.determining region 3(CDR3) of immunoglobulin heavy chain (IgH) gene and T-cell receptor gamma (TCRgamma) gene by polymerase chain reaction (PCR) technique was done. The two lymphomas in the spleen demonstrated the same rearrangement pattern in both IgH and TCRgamma gene. We think these findings strongly suggest that the large cell lymphoma has the same clonality with that of the small lymphocytic lymphoma.
- Primary Malignant Lymphoma of the Gallbladder: A case of report.
- Jung Sun Kim, Chul Woo Kim, Yong Il Kim, Yong Bum Yoon, Yung Jue Bang
- Korean J Pathol. 1994;28(5):538-540.
- 2,316 View
- 13 Download
-
Abstract
PDF
- Lymphomatous involvement of the gallbladder is rarely identified and manifests mostly as a local involvement of disseminated disease. There have been reported only about 20 primary malignant lymphomas of the gallbladder without involvement of other sites. A 63-year-old woman presented with jaundice, epigastric pain, and weight olss of two months duration. There was no systemic lymphadenopathy elsewhere. Abdominal computed tomograph revealed a focal thickening of the gallbladder wall. The removed gallbladder contained a well circumscribed, 5x3 cm-sized, slightly elevated firm area with accentuated mucosal papillary excrescences near the neck protion. The lesion involved whole thickness of the wall, and was made up of diffuse atypical lymphoid cell infiltrates of variable size accompanying plasmacytoid differentiation in areas. Some large tumor cells were pleomorphic and contained prominent nucleoli. To our knowledge, this is the first case of primary malignant lymphoma of the gallbladder in Korean literature.
Original Articles
- Epstein-Barr Viral RNA(EBERs) Expression in Conventional Malignant Lymphoma and Polymorphic Reticulosis of Upper Aerodigestive Tract.
- Do Youn Park, Kang Suek Suh, Sun Kyung Lee
- Korean J Pathol. 1996;30(10):893-902.
- 2,188 View
- 12 Download
-
Abstract
PDF
- The author examined the immunophenotype and expression of Epstem-Barr virus RNA (EBERs) used in the situ hybridization technique in 20 cases of conventional malignant lymphoma and 28 cases of polymorphic reticulosis and malignant lymphoma with features of polymorphic reticulosis occured in the upper aerodigestive tract including the upper digestive tract(palatine tonsil), and upper respiratory tract(nasal cavity, paranasal sinus, nasopharynx). The results obtained were summarized as followings; 1. The favorable site of malignant lymphoma that occured in the upper aerodigestive tract was in the palatine tonsil(11 out of 20 cases, 55%), those of polymorphic reticulosis and malignant lymphoma with features of polymorphic reticulosis were nasal cavity and nasopharynx(19 out of 28 cases, 78%). 2. The immunophentype of malignant lymphoma that occured in the upper aerodigestive tract was mostly B-cell phenotype (15 out of 20 cases, 75%), and that of polymorphic reticulosis and malignant lymphoma with features of polymorphic reticulosis was predominantly T-cell phenotype(22 out of 28 cases, 79%). 3. The EBERs positivity of malignant lymphoma that occured in the upper aerodigestive tract was 25%(5 out of 20 cases), but that of polymorphic reticulosis and malignant lymphoma with features of polymorphic reticulosis was 57%(16 out of 28 cases). 4. The positive cases for EBERs revealed angiocentricity with necrosis(16 out of 21 cases, 76%), predominantly T-cell phenotype(19 out of 21 cases, 90%), and favorably involved the nasal cavity and nasopharynx(16 out of 21 cases, 76%). Based on the above results, it was concluded that polymorphic reticulosis and malignant lymphoma with features of polymorphic reticulosis that occurred in the upper respiratory tract was an EBV-positive angiocentric T-cell lymphoma favorably involving the nasal cavity and nasopharynx.
- Primary Central Nervous System Lymphomas; A Clinicopathologic Study of 18 Cases.
- Yu Kyung Jeong, Young Hyeh Ko, Dong Kyu Na, Yeon Lim Suh, Sang Yong Song, Dae Shik Kim, Mi Kyung Kim, Howe Jung Ree
- Korean J Pathol. 1998;32(9):670-679.
- 2,429 View
- 10 Download
-
Abstract
- The incidence of a primary central nervous system (CNS) lymphoma in western countries is about 1% of all the intracranial tumors and has increased 2.2% over the last decade. A similar pattern of increased frequency is observed in Korea. Although most CNS lymphomas in western countries are high grade tumors carrying poor prognosis, the clinicopathologic features of the Korean CNS lymphoma have not been well studied. We report clinicopathological features of 18 cases of histologically proven primary brain lymphoma. The mean age of the patients was 50 years and there was no sex difference. The clinical and radiological characteristics included multiple site of occurrence, infrequent extracranial spread, and frequent seeding via cerebrospinal fluid. No patients were immune-compromised host. Of 18 cases, 15 cases were of B-lineage and 2 cases were of T-lineage. According to REAL classification, there were 12 cases of diffuse large B cell lymphoma, two cases of B cell lymphomas of small lymphoid cell, and two cases of peripheral T cell lymphoma, unspecified. The remaining subtypes were not subclassified because of inadequate material. Pleomorphic cytologic features and necrosis of varying extent were frequent in the cases of diffuse large B-cell lymphoma. These results suggest that overall clinicopathologic features of primary malignant lymphomas of the central nervous system in Korea are similar to those of western countries.
Case Report
- Bronchus-Associated Lymphoid Tissue Lymphoma.
- Yoon Ju Kim, Sung Sook Paeng, Hee Jin Chang, Jung Il Suh
- Korean J Pathol. 1998;32(11):1035-1038.
- 2,387 View
- 10 Download
-
Abstract
- Malignant lymphoma arising from mucosa-associated lymphoid tissue (MALT) represents distinct clinicopathologic features and remains localized for prolonged periods. We report a case of low grade B cell lymphoma of bronchus-associated lymphoid tissue (BALT). A 60-year-old female had a long-standing cough, sputum and intermittent fever for 10 years. In 1984, the chest radiography showed increased hazy density in both upper lungs. Although she had been treated by antituberculous medication under clinical diagnosis, there was no improvement. In 1995, open lung biopsy was carried out. Histologically, it showed massive nodular or diffuse infiltration of centrocyte-like cells in bronchus and parenchyme with pleural invasion. On immunohistochemical stain, they were positive for LN-2 and L26 and negative for UCHL-1, LN-1 and LN-3. In polymerase chain reaction (PCR), Ig heavy chain gene rearrangement was detected. The patient was well for 6 months after the biopsy.
Original Articles
- The Value of Immunohistochemistry on Paraffin Embedded Tissue Sections in the Differentiation of Subgroups of Low Grade B-Cell Lymphomas.
- Tae Sook Hwang, Seung Sook Lee, Ji Eun Kim, Hye Seung Han, Chul Woo Kim
- Korean J Pathol. 1998;32(12):1066-1073.
- 2,114 View
- 10 Download
-
Abstract
- There had been a continuous evolution of lymphoma classification and recently a Revised European-American Lymphoma Classification was proposed by the International Lymphoma Study Group. This new classification often requires information on immunophenotypic and molecular biologic markers in addition to the usual histologic findings. Recent advances in the production of commercially available monoclonal antibodies reactive on formalin-fixed paraffin-embedded tissues provide us a great help to classify the non-Hodgkin's lymphoma. We have analyzed 31 low grade B-cell lymphomas by the schemes proposed by the International Lymphoma Study Group using antibodies to CD3, CD5, CD20, CD23, CD43, cyclin D1, and bcl-2 protein, and have analyzed the immunophenotypic features. Among 31 low grade B-cell lymphomas, 8 small lymphocytic lymphomas, 5 mantle cell lymphomas, 7 follicle center lymphomas (2 grade I, 3 grade II, and 2 grade III), and 11 marginal zone B-cell lymphomas (all of which were extranodal) were identified. Among 8 small lymphocytic lymphomas, 5 cases were positive for CD5; 6 cases were positive for CD23; 7 cases were positive for CD43; all 8 cases were negative for cyclin D1; and 7 cases were positive for bcl-2. Among 5 mantle cell lymphomas, 4 cases were positive for CD5 and CD43; all five cases were negative for CD23; 4 cases were positive for cyclin D1 and bcl-2. All 7 follicle center lymphomas were negative for CD5, CD43 and cyclin D1 and 2 cases were positive for CD23; and 6 cases were positive for bcl-2. All marginal zone B-cell lymphomas were negative for CD5, CD23 and cyclin D1; 3 cases were positive for CD43 and 9 cases were positive for bcl-2. Diagnostic utility for CD5 antigen detection on paraffin embedded tissue has a limitation due to weak antigen expression in tumor cells of B-cell lymphomas; however, still be useful in differentiating small lymphocytic lymphoma and mantle cell lymphoma from other B-cell lymphomas when applied in conjunction with CD43. CD23, CD43, and cyclin D1 appear to be of great help in differentiating subgroups of low grade B-cell lymphomas. Bcl-2, as known, is found to be useful to rule out reactive follicular hyperplasia.
- Histologic and Immunopathologic Study of Central Nervous System Lymphoma.
- Yee Jeong Kim, Tae Seung Kim, Woo Ick Yang, Kyu Rae Kim
- Korean J Pathol. 1992;26(5):476-483.
- 2,199 View
- 14 Download
-
Abstract
PDF
- Twelve cases of primary malignant lymphoma of the central nervous system experienced between 1980 and 1990 were investigated by histological and immunohistochemical findings correlated with clinical observation. Of the 12 patients, 6 were male and 6 were female. Their ages ranged from 31 to 58 years(mean, 45.8 years). All Tumors were supratentorial except 1 case which was found in the spinal cord. The fronto-parietal lobe was the most common site, which accounted for 66.7%. Histologically, all the tumors showed unfavorable histology. Diffuse large cell type was the most frequent(66.7%). Immunohistochemical studies using monoclonal antibodies revealed predominance of B-cell phenotype. Although most cases were treated with a combination of surgery and irradiation, the outcome was poor in all.
 First
First Prev
Prev


