 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Articles
- Clinicopathological profile of high-grade differentiated thyroid carcinoma in an Indonesian tertiary hospital
- Novita , Agnes Stephanie Harahap, Maria Francisca Ham, Alfianto Widiono, Chan Kwon Jung
- J Pathol Transl Med. 2026;60(3):338-348. Published online April 23, 2026
- DOI: https://doi.org/10.4132/jptm.2026.01.15
- 2,139 View
- 72 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background
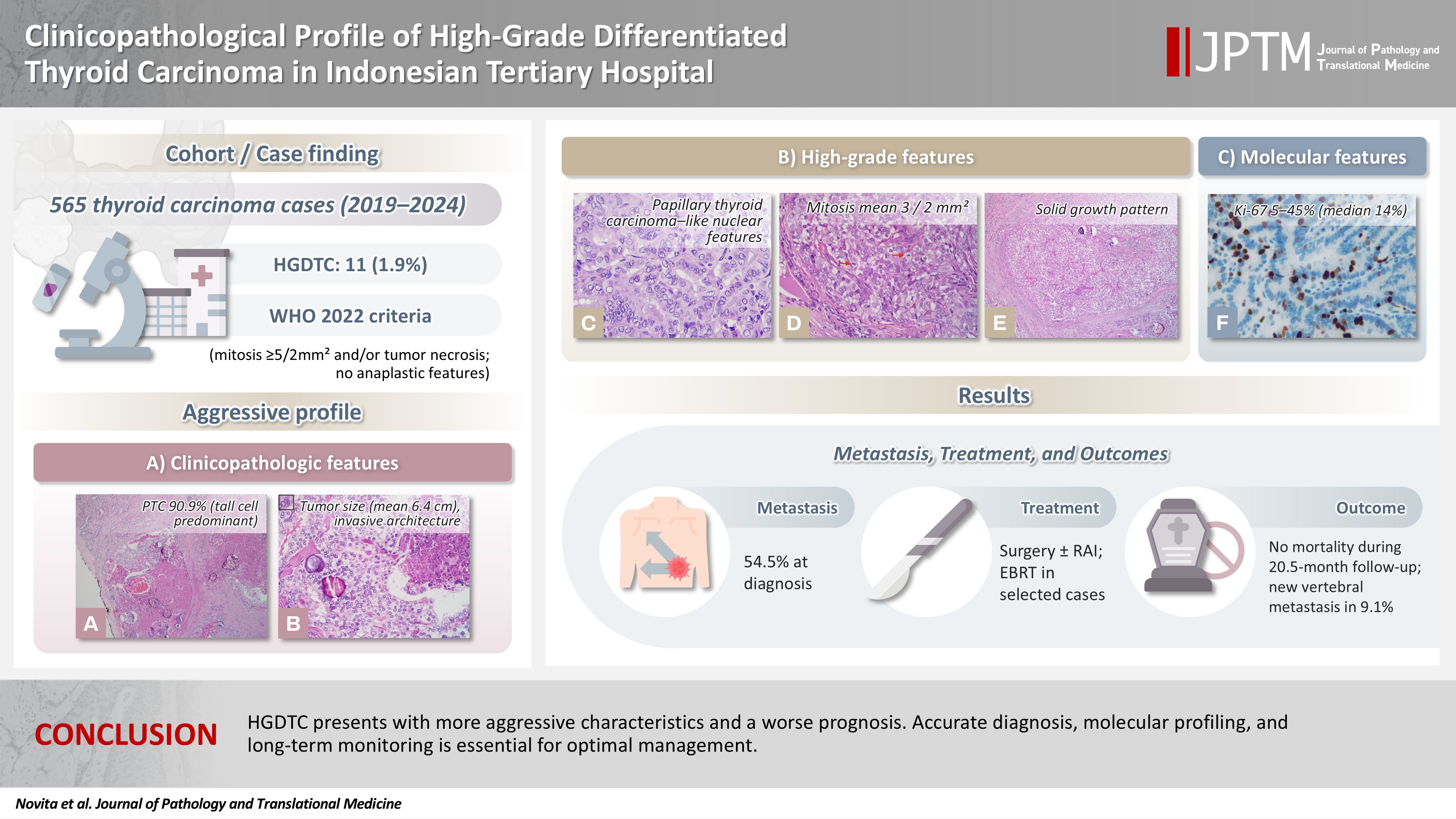
High-grade differentiated thyroid carcinoma (HGDTC) is a recently recognized entity in the 2022 World Health Organization classification, representing a more aggressive subtype of differentiated thyroid carcinoma. Previously, high-grade features such as increased mitotic activity and tumor necrosis were often overlooked, despite being important independent prognostic factors. Although rare, HGDTC carries significant diagnostic, prognostic, and therapeutic implications. Data remain limited in Indonesia. Methods: This retrospective descriptive study reviewed 565 thyroid carcinoma cases diagnosed at Cipto Mangunkusumo Hospital from 2019 to 2024. Eleven cases (1.9%) met HGDTC criteria. Clinicopathological characteristics, histologic subtypes, Ki-67 proliferation index, molecular alterations, treatment modalities, and clinical outcomes were analyzed. Results: Patients had a mean age of 54.6 years, with a female-to-male ratio of 2.7:1. Papillary thyroid carcinoma was the main type (90.9%), with the tall cell subtype predominating. Mean tumor size was 6.4 cm. Lymphatic invasion, vascular invasion, and extrathyroidal extension were present in 54.5%, 18.2%, and 45.5% of cases, respectively. All tumors showed necrosis. Mean mitotic count was 3 per 2 mm². The Ki-67 index ranged from 5% to 45% (median, 14%). BRAFV600E and TERT promoter mutations were detected in 18.2% and 36.4% of cases, respectively, with co-mutations in 18.2%. Six cases (54.5%) had metastases at time of diagnosis. During a mean follow-up of 20.5 months, one patient (9.1%) developed new vertebral metastases and all patients (100%) remained alive. Conclusions: HGDTC presents with more aggressive characteristics and a worse prognosis. Accurate diagnosis, molecular profiling, and long-term monitoring are essential for optimal management.
- Lessons learned from the first 2 years of experience with thyroid core needle biopsy at an Indonesian national referral hospital
- Agnes Stephanie Harahap, Maria Francisca Ham, Retno Asti Werdhani, Erwin Danil Julian, Rafi Ilmansyah, Chloe Indira Arfelita Mangunkusumso, Tri Juli Edi Tarigan
- J Pathol Transl Med. 2025;59(3):149-160. Published online April 25, 2025
- DOI: https://doi.org/10.4132/jptm.2025.02.19

- 5,404 View
- 207 Download
- 1 Web of Science
- 2 Crossref
-
Abstract
PDF
- Background
Core needle biopsy (CNB) improves diagnostic accuracy by providing precise tissue sampling for histopathological evaluation, overcoming the limitation of inconclusive fine-needle aspiration results. This study evaluated the diagnostic performance of CNB in assessing thyroid nodules, with additional analysis of the benefits of BRAF V600E and RAS Q61R immunohistochemical (IHC) markers.
Methods
This retrospective study enrolled patients with thyroid nodules who underwent CNB at Dr. Cipto Mangunkusumo Hospital, Jakarta, from July 2022 to July 2024. CNB diagnoses were classified using the Korean Thyroid Association Criteria. Diagnostic efficacy was evaluated for neoplastic and malignant lesions, both independently and with BRAF V600E and RAS Q61R IHC. The correlation between nodule size and postoperative diagnosis was also analyzed.
Results
A total of 338 thyroid nodule samples was included, and 52.7% were classified as CNB category II. In the 104 samples with postoperative diagnoses, category IV was the most prevalent (39.4%). CNB demonstrated a sensitivity of 74% and a specificity of 100% for neoplastic lesions and 23.8% sensitivity and 100% specificity for malignant lesions. Combining CNB with BRAF V600E and RAS Q1R IHC increased the sensitivity to 77% for neoplastic lesions and 28.8% for malignant lesions. Larger nodules (>3 cm) were significantly associated with neoplastic (p = .005) and malignant lesions (p = .004).
Conclusions
CNB performs well in identifying neoplastic lesions, with or without BRAF V600E and RAS Q61R IHC, but its low sensitivity for malignant lesions warrants caution. While CNB categories V–VI indicate malignancy, the possibility of malignancy in categories I–IV should not be overlooked. -
Citations
Citations to this article as recorded by
- Clinicopathological profile of high-grade differentiated thyroid carcinoma in an Indonesian tertiary hospital
Novita, Agnes Stephanie Harahap, Maria Francisca Ham, Alfianto Widiono, Chan Kwon Jung
Journal of Pathology and Translational Medicine.2026; 60(3): 338. CrossRef - Integrating Digital Ki-67 Labeling Index and K-TIRADS for Malignancy Risk Stratification in Thyroid Core Needle Biopsies
Yujin Cha, Sue Youn Kim, Chankyung Kim, Ja Seong Bae, Dong-Jun Lim, So-Lyung Jung, Chan Kwon Jung
Cancers.2026; 18(14): 2260. CrossRef
- Clinicopathological profile of high-grade differentiated thyroid carcinoma in an Indonesian tertiary hospital
Correspondence
- Erratum: Diagnostic challenges in the assessment of thyroid neoplasms using nuclear features and vascular and capsular invasion: a multi-center interobserver agreement study
- Agnes Stephanie Harahap, Mutiah Mutmainnah, Maria Francisca Ham, Dina Khoirunnisa, Abdillah Hasbi Assadyk, Husni Cangara, Aswiyanti Asri, Diah Prabawati Retnani, Fairuz Quzwain, Hasrayati Agustina, Hermawan Istiadi, Indri Windarti, Krisna Murti, Muhammad Takbir, Ni Made Mahastuti, Nila Kurniasari, Nungki Anggorowati, Pamela Abineno, Yulita Pundewi Setyorini, Kennichi Kakudo
- J Pathol Transl Med. 2025;59(3):201-201. Published online March 31, 2025
- DOI: https://doi.org/10.4132/jptm.2024.07.25.r
- Corrects: J Pathol Transl Med 2024;58(6):299
- 3,036 View
- 66 Download
- 1 Crossref
Review
- Cytologic hallmarks and differential diagnosis of papillary thyroid carcinoma subtypes
- Agnes Stephanie Harahap, Chan Kwon Jung
- J Pathol Transl Med. 2024;58(6):265-282. Published online November 7, 2024
- DOI: https://doi.org/10.4132/jptm.2024.10.11
- 23,612 View
- 829 Download
- 17 Web of Science
- 15 Crossref
-
Abstract
PDF
- Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy, characterized by a range of subtypes that differ in their cytologic features, clinical behavior, and prognosis. Accurate cytologic evaluation of PTC using fine-needle aspiration is essential but can be challenging due to the morphologic diversity among subtypes. This review focuses on the distinct cytologic characteristics of various PTC subtypes, including the classic type, follicular variant, tall cell, columnar cell, hobnail, diffuse sclerosing, Warthin-like, solid/trabecular, and oncocytic PTCs. Each subtype demonstrates unique nuclear features, architectural patterns, and background elements essential for diagnosis and differentiation from other thyroid lesions. Recognizing these distinct cytologic patterns is essential for identifying aggressive subtypes like tall cell, hobnail, and columnar cell PTCs, which have a higher risk of recurrence, metastasis, and poorer clinical outcomes. Additionally, rare subtypes such as diffuse sclerosing and Warthin-like PTCs present unique cytologic profiles that must be carefully interpreted to avoid diagnostic errors. The review also highlights the cytologic indicators of lymph node metastasis and high-grade features, such as differentiated high-grade thyroid carcinoma. The integration of molecular testing can further refine subtype diagnosis by identifying specific genetic mutations. A thorough understanding of these subtype-specific cytologic features and molecular profiles is vital for accurate diagnosis, risk stratification, and personalized management of PTC patients. Future improvements in diagnostic techniques and standardization are needed to enhance cytologic evaluation and clinical decision-making in thyroid cancer.
-
Citations
Citations to this article as recorded by- Oncocytic Thyroid Tumours With Pathogenic FLCN Mutations Mimic Oncocytic Papillary Thyroid Carcinoma on Fine‐Needle Aspiration
Adeel M. Ashraf, Faisal Hassan, Adrian A. Dawkins, Julie C. Dueber, Derek B. Allison, Thèrése J. Bocklage
Cytopathology.2026; 37(1): 108. CrossRef - Using a new type of visible light-based emission fluorescence microscope to identify the benign and malignant nature of thyroid tissue during the surgical process: Analysis of diagnostic results
Yu Miao, Liu Xiaowei, Li Muyang, Gao Jian, Chen Lu
Photodiagnosis and Photodynamic Therapy.2026; 57: 105324. CrossRef - Clinical Behavior of Aggressive Variants of Papillary Thyroid Carcinoma: A Retrospective Case–Control Study
Jovan Ilic, Nikola Slijepcevic, Katarina Tausanovic, Bozidar Odalovic, Goran Zoric, Marija Milinkovic, Branislav Rovcanin, Milan Jovanovic, Matija Buzejic, Duska Vucen, Boban Stepanovic, Sara Ivanis, Milan Parezanovic, Milan Marinkovic, Vladan Zivaljevic
Cancers.2026; 18(2): 345. CrossRef - Advantages of thyroid core needle biopsy: an emerging selective first-line biopsy modality
Jae Ho Shin, Yeseul Kim, Min Kyoung Lee, Jung Hwan Baek, So Lyung Jung
Ultrasonography.2026; 45(3): 205. CrossRef - Clinicopathological profile of high-grade differentiated thyroid carcinoma in an Indonesian tertiary hospital
Novita, Agnes Stephanie Harahap, Maria Francisca Ham, Alfianto Widiono, Chan Kwon Jung
Journal of Pathology and Translational Medicine.2026; 60(3): 338. CrossRef - Interpretable SVM-Based Integrated Ultrasound Model for Preoperative Thyroid Nodule Subtype Classification: Improved Identification of Follicular Variant Papillary Thyroid Carcinoma
Ran Zheng, Zhen Wang, Yongxin Li, Yuanqing Zhang, Fang Nie
Diagnostics.2026; 16(13): 1950. CrossRef - Papillary thyroid carcinoma in thyroglossal duct cyst: a Peruvian case series
José Luis Paz-Ibarra, Marialejandra Delgado Rojas, Edward Paucar Holgado, Jenyfer María Fuentes-Mendoza, Luis Concepción-Urteaga, Juan Eduardo Quiroz-Aldave, Marcio José Concepción-Zavaleta, José Somocurcio Peralta
Endocrinology, Diabetes & Metabolism Case Reports.2026;[Epub] CrossRef - Single-cell reveals age-dependent epithelial reprogramming and EMT vulnerability in THCA
Qiankun Zhang, Wei Pan, Xiaohua Gong, Qi Zhou
Endocrine-Related Cancer.2026;[Epub] CrossRef - Nuclear pseudoinclusion is associated with BRAFV600E mutation: Analysis of nuclear features in papillary thyroid carcinoma
Agnes Stephanie Harahap, Dina Khoirunnisa, Salinah, Maria Francisca Ham
Annals of Diagnostic Pathology.2025; 75: 152434. CrossRef - 2025 Korean Thyroid Association Clinical Management Guideline on Active Surveillance for Low-Risk Papillary Thyroid Carcinoma
Eun Kyung Lee, Min Joo Kim, Seung Heon Kang, Bon Seok Koo, Kyungsik Kim, Mijin Kim, Bo Hyun Kim, Ji-hoon Kim, Shin Je Moon, Kyorim Back, Young Shin Song, Jong-hyuk Ahn, Hwa Young Ahn, Ho-Ryun Won, Won Sang Yoo, Min Kyoung Lee, Jeongmin Lee, Ji Ye Lee, Kyo
International Journal of Thyroidology.2025; 18(1): 30. CrossRef - Structure-based molecular screening and dynamic simulation of phytocompounds targeting VEGFR-2: a novel therapeutic approach for papillary thyroid carcinoma
Shuai Wang, Lingqian Zhang, Wenjun Zhang, Xiong Zeng, Jie Mei, Weidong Xiao, Lijie Yang
Frontiers in Pharmacology.2025;[Epub] CrossRef - 2025 Korean Thyroid Association Clinical Management Guideline on Active Surveillance for Low-Risk Papillary Thyroid Carcinoma
Eun Kyung Lee, Min Joo Kim, Seung Heon Kang, Bon Seok Koo, Kyungsik Kim, Mijin Kim, Bo Hyun Kim, Ji-hoon Kim, Shinje Moon, Kyorim Back, Young Shin Song, Jong-hyuk Ahn, Hwa Young Ahn, Ho-Ryun Won, Won Sang Yoo, Min Kyoung Lee, Jeongmin Lee, Ji Ye Lee, Kyon
Endocrinology and Metabolism.2025; 40(3): 307. CrossRef - A Case of Warthin-Like Variant of Papillary Thyroid Cancer
Amy Chow, Israa Laklouk
Cureus.2025;[Epub] CrossRef - Propensity score-matched analysis of the ‘2+2’ parathyroid strategy in total thyroidectomy with central neck dissection
Hao Gong, Simei Yao, Tianyuchen Jiang, Yi Yang, Yuhan Jiang, Zhujuan Wu, Anping Su
Frontiers in Endocrinology.2025;[Epub] CrossRef - Cytological Findings in Pediatric Thoracic Tumors: A Review of Diagnostic Insights and Pitfalls
Parikshaa Gupta, Pranab Dey
Acta Cytologica.2025; 70(3): 320. CrossRef
- Oncocytic Thyroid Tumours With Pathogenic FLCN Mutations Mimic Oncocytic Papillary Thyroid Carcinoma on Fine‐Needle Aspiration
Original Articles
- Diagnostic challenges in the assessment of thyroid neoplasms using nuclear features and vascular and capsular invasion: a multi-center interobserver agreement study
- Agnes Stephanie Harahap, Mutiah Mutmainnah, Maria Francisca Ham, Dina Khoirunnisa, Abdillah Hasbi Assadyk, Husni Cangara, Aswiyanti Asri, Diah Prabawati Retnani, Fairuz Quzwain, Hasrayati Agustina, Hermawan Istiadi, Indri Windarti, Krisna Murti, Muhammad Takbir, Ni Made Mahastuti, Nila Kurniasari, Nungki Anggorowati, Pamela Abineno, Yulita Pundewi Setyorini, Kennichi Kakudo
- J Pathol Transl Med. 2024;58(6):299-309. Published online September 12, 2024
- DOI: https://doi.org/10.4132/jptm.2024.07.25
- Correction in: J Pathol Transl Med 2025;59(3):201
- 7,129 View
- 432 Download
- 2 Web of Science
- 1 Crossref
-
Abstract
PDFSupplementary Material
- Background
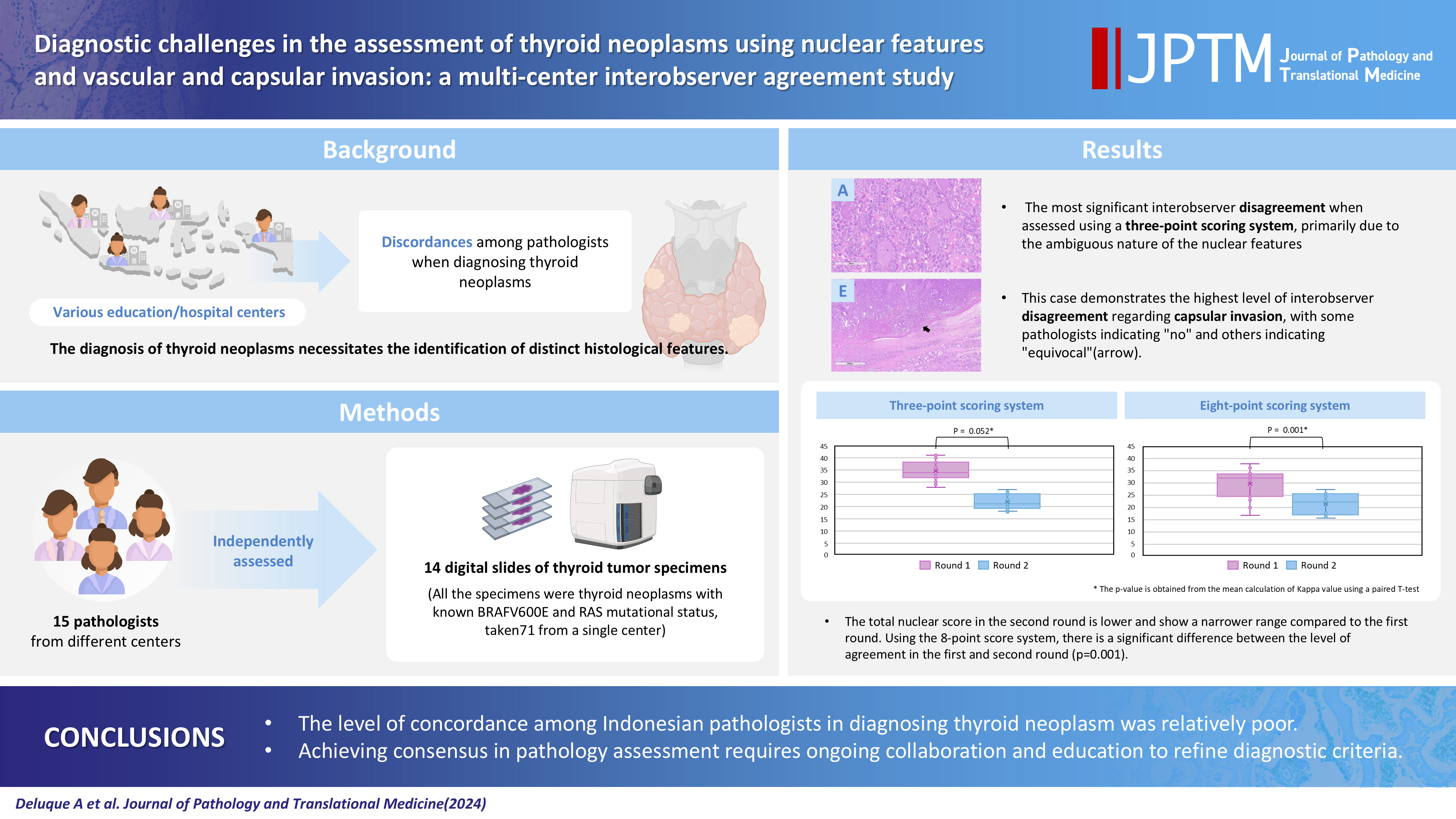
The diagnosis of thyroid neoplasms necessitates the identification of distinct histological features. Various education/hospital centers located in cities across Indonesia likely result in discordances among pathologists when diagnosing thyroid neoplasms.
Methods
This study examined the concordance among Indonesian pathologists in assessing nuclear features and capsular and vascular invasion of thyroid tumors. Fifteen pathologists from different centers independently assessed the same 14 digital slides of thyroid tumor specimens. All the specimens were thyroid neoplasms with known BRAFV600E and RAS mutational status, from a single center. We evaluated the pre- and post-training agreement using the Fleiss kappa. The significance of the training was evaluated using a paired T-test.
Results
Baseline agreement on nuclear features was slight to fair based on a 3-point scoring system (k = 0.14 to 0.28) and poor to fair based on an eight-point system (k = –0.02 to 0.24). Agreements on vascular (κ = 0.35) and capsular invasion (κ = 0.27) were fair, whereas the estimated molecular type showed substantial agreement (κ = 0.74). Following the training, agreement using the eight-point system significantly improved (p = 0.001).
Conclusions
The level of concordance among Indonesian pathologists in diagnosing thyroid neoplasm was relatively poor. Consensus in pathology assessment requires ongoing collaboration and education to refine diagnostic criteria. -
Citations
Citations to this article as recorded by- Nuclear pseudoinclusion is associated with BRAFV600E mutation: Analysis of nuclear features in papillary thyroid carcinoma
Agnes Stephanie Harahap, Dina Khoirunnisa, Salinah, Maria Francisca Ham
Annals of Diagnostic Pathology.2025; 75: 152434. CrossRef
- Nuclear pseudoinclusion is associated with BRAFV600E mutation: Analysis of nuclear features in papillary thyroid carcinoma
- Educational exchange in thyroid core needle biopsy diagnosis: enhancing pathological interpretation through guideline integration and peer learning
- Agnes Stephanie Harahap, Chan Kwon Jung
- J Pathol Transl Med. 2024;58(5):205-213. Published online July 24, 2024
- DOI: https://doi.org/10.4132/jptm.2024.06.24
- 6,932 View
- 305 Download
- 1 Web of Science
- 2 Crossref
-
Abstract
PDF
- Background
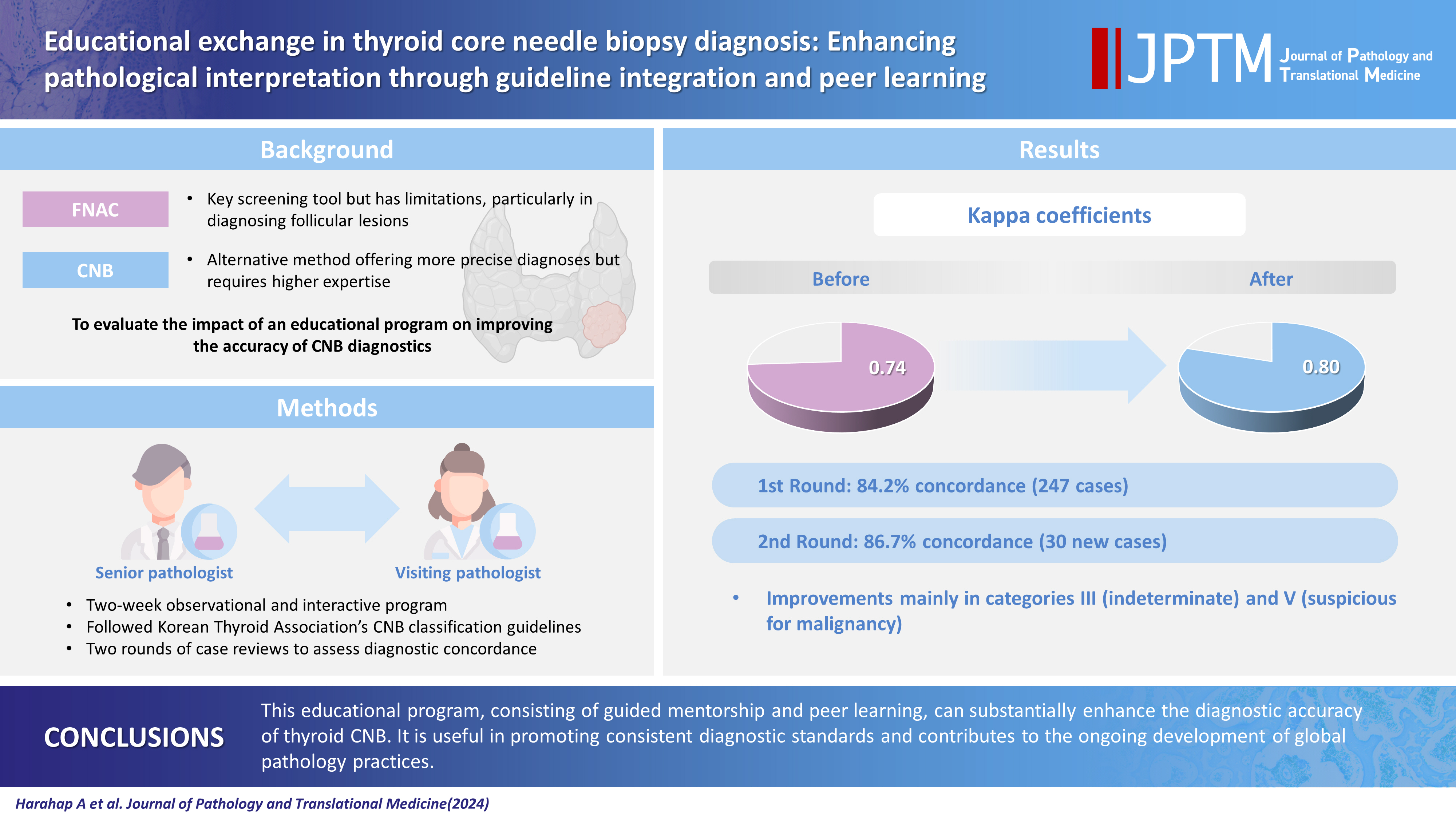
While fine needle aspiration cytology (FNAC) plays an essential role in the screening of thyroid nodules, core needle biopsy (CNB) acts as an alternative method to address FNAC limitations. However, diagnosing thyroid CNB samples can be challenging due to variations in background and levels of experience. Effective training is indispensable to mitigate this challenge. We aim to evaluate the impact of an educational program on improving the accuracy of CNB diagnostics.
Methods
The 2-week observational program included a host mentor pathologist with extensive experience and a visiting pathologist. The CNB classification by The Practice Guidelines Committee of the Korean Thyroid Association was used for the report. Two rounds of reviewing the case were carried out, and the level of agreement between the reviewers was analyzed.
Results
The first-round assessment showed a concordance between two pathologists for 247 thyroid CNB specimens by 84.2%, with a kappa coefficient of 0.74 (indicating substantial agreement). This finding was attributed to the discordance in the use of categories III and V. After peer learning, the two pathologists evaluated 30 new cases, which showed an overall improvement in the level of agreement. The percentage of agreement between pathologists on thyroid CNB diagnosis was 86.7%, as measured by kappa coefficient of 0.80.
Conclusions
This educational program, consisting of guided mentorship and peer learning, can substantially enhance the diagnostic accuracy of thyroid CNB. It is useful in promoting consistent diagnostic standards and contributes to the ongoing development of global pathology practices. -
Citations
Citations to this article as recorded by- Integrating Digital Ki-67 Labeling Index and K-TIRADS for Malignancy Risk Stratification in Thyroid Core Needle Biopsies
Yujin Cha, Sue Youn Kim, Chankyung Kim, Ja Seong Bae, Dong-Jun Lim, So-Lyung Jung, Chan Kwon Jung
Cancers.2026; 18(14): 2260. CrossRef - Lessons learned from the first 2 years of experience with thyroid core needle biopsy at an Indonesian national referral hospital
Agnes Stephanie Harahap, Maria Francisca Ham, Retno Asti Werdhani, Erwin Danil Julian, Rafi Ilmansyah, Chloe Indira Arfelita Mangunkusumso, Tri Juli Edi Tarigan
Journal of Pathology and Translational Medicine.2025; 59(3): 149. CrossRef
- Integrating Digital Ki-67 Labeling Index and K-TIRADS for Malignancy Risk Stratification in Thyroid Core Needle Biopsies
 First
First Prev
Prev


