An Unusual Case of Pulmonary Mucous Gland Adenoma with Fibromyxoid Stroma and Cartilage Islands in 68-Year-Old Woman
Article information
Pulmonary mucous gland adenoma (MGA) is an uncommon, benign tumor that histologically resembles the mucus-secreting component of the tracheobronchial gland. The majority of such tumors arise within the main, lobar or segmental bronchi, but peripheral lesions have been reported.1 The exact incidence rate cannot be determined, but its rarity can be presumed considering that the ten cases reported by England and Hochholzer2 is the largest available data set. Four cases of MGA were reported in Korea,1,3 and our case is the second presenting in the peripheral lung.1 MGA comprises many mucin-filled cystic spaces lined by bland columnar or flattened mucus-secreting cells. Though MGA usually has bands of spindle-rich stroma and may be hyalinized, multiple cartilage islands are an extraordinary finding. To the best of our knowledge, there has been no case of MGA combined with hamartoma-like stroma. Herein, we report a case of bronchial MGA with fibromyxoid stroma and cartilage islands in a 68-year-old woman.
CASE REPORT
68-year-old woman, who had no specific medical history or history of smoking, was transferred to our hospital due to an incidentally identified mass at the peripheral territory of the right upper lobe of the lung (Fig. 1A). The mass measured about 3 cm in diameter with no definite change of size over 18 months. In spite of bronchoscopic biopsy, no definite diagnosis could be made. One year later, positron emission tomography revealed a mild hypermetabolic state of the mass with no other remarkable findings, and wedge resection of the lung was performed for histological confirmation.
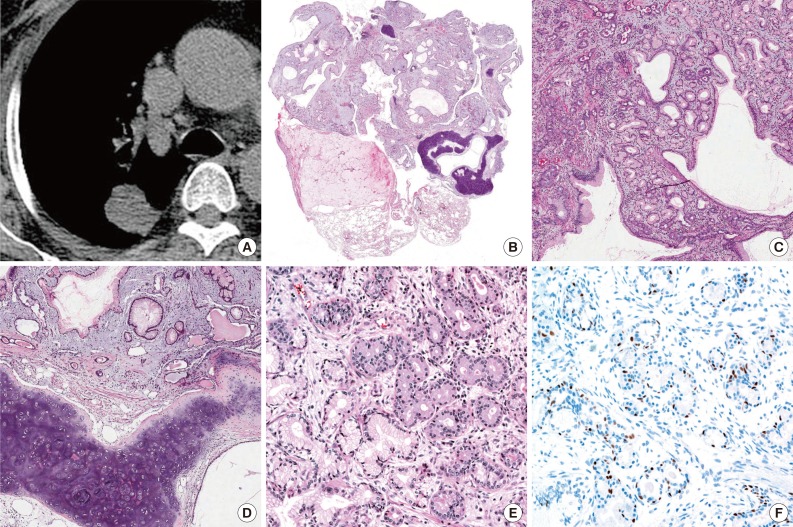
Mucous gland adenoma with fibromyxoid stroma and cartilage islands of lung. (A) Computed tomography shows a 3-cm-sized, well circumscribed mass at the posterior segment of the right upper lobe of lung. (B) The tumor is well circumscribed and shows multiple varying cysts surrounded by myxoid stroma and several separated islands of cartilage. (C) Irregularly-shaped mucous glands are noted on the myxoid background. (D) Some of the glands are cystically dilated and filled with proteinaceous material and separated islands of cartilage. (E) Mucoserous glands are lined by columnar or flat cuboidal epithelial cells with clear or eosinophilic cytoplasm and basally located small nuclei with no atypia. (F) Myoepithelial cells of glands show positivity for p63; however, stromal cells are negative.
Macroscopically, the mass was a 3×1.9-cm-sized, solid ovoid mass that had a grayish and weakly glistening cut surface and disclosed several small cystic spaces and fragments of cartilage. There was no identifiable connection to the bronchus on any of multiple sections. Microscopically, the tumor was well circumscribed and composed of multiple cystic glands and myxoid stroma containing lobules of cartilage (Fig. 1B). Mucous and serous glands were haphazardly scattered on the myxoid background, and some of them were cystically dilated; however, no invasive foci were found (Fig. 1C). Irregularly-shaped cartilaginous islands were noted on the myxoid stroma, and some of the dilated glands were filled with proteinaceous or secretory material (Fig. 1D). The lining epithelial cells of the glands had basally located hyperchromatic nuclei and abundant clear or eosinophilic cytoplasm (Fig. 1E). No mitotic figure was observed. Immunohistochemical staining for p63 (1:200, 4A4, Dako, Glostrup, Denmark) (Fig. 1F) and calponin (1:200, CALP, Bio-Genex, San Ramon, CA, USA) showed positivity in the myoepithelial cells in glands but negativity in the stromal cells. The patient is alive and well five months after the operation.
DISCUSSION
Pulmonary MGA with lack of bronchial relation is extremely unusual.4 Moreover, MGA of the peripheral lung with cartilage islands has not been reported.
The histologic findings of a benign mucous glandular proliferation mixed with cartilage/mesenchymal component suggest several possible scenarios. First, it is reasonable that MGA with myxoid stroma develops chondroid metaplasia, as occurs in other organs. The stroma of MGAs varies, and hyalinized sclerosis can be seen.2 However, no report describing myxoid stroma and cartilage islands in MGA could be found in the English literature.
We also considered coincidental combination of MGA and pulmonary hamartoma. There was a case report of a collision tumor of pulmonary hamartoma and a carcinoid.5 However, this was likely an extremely extraordinary situation, considering the rarity of mucus gland adenoma.
There have been two reported cases of salivary gland-type tumors developed in hamartoma; myoepithelioma and malignant mixed tumor.6 The myoepithelial cells composing these tumors can arise from stromal cells of hamartoma. Additionally, there was no glandular component like our case of MGA.
Pleomorphic adenoma of the lung also can be considered, showing varying admixtures of epithelial elements and a stromal/mesenchymal component showing abundant myxoid or focally chondroid matrix. In a literature review of 24 cases of salivary gland-type mixed tumor of the lung, Matsumoto et al.7 suggested that peripherally developed tumors might be derived from primitive stem cells with the ability to differentiate toward ductal structures, myoepithelium, and chondroid and myxoid matrix components. However, our case is morphologically different from pleomorphic adenoma, and immunohistochemical staining of myoepithelial cells showed positivity for normal myoepithelial cells within glands and negative for the stromal cells, while pleomorphic adenoma shows positivity for the stromal cells.
Although none of the above possibilities sufficiently explains the histologic finding of our case, it is a very interesting case. Herein, we report a rare case of MGA with fibromyxoid stroma and cartilage islands.
Notes
No potential conflict of interest relevant to this article was reported.