Congenital Peribronchial Myofibroblastic Tumor: A Case Study and Literature Review
Article information
Abstract
Congenital peribronchial myofibroblastic tumor (CPMT) is a benign pulmonary spindle cell neoplasm of intrauterine and perinatal period, which is thought to arise from primitive peribronchial mesenchyme. We present a case detected incidentally in a one-month-old infant. The solid and partially necrotic tumor involved the right middle and lower lobes of the lung with extension to the diaphragm. Histologically, the tumor was composed of fasciculated monotonous spindle cells, proliferating peribronchiolar cartilage and round cells with rich vasculature, and high mitotic activity was identified in the round cell area. Immunohistochemical and electron microscopic studies showed that the spindle cells were myofibroblastic in phenotype. Although the tumor showed several malignant pathological features, recurrence was not observed in the two-year follow-up period, consistent with the benign clinical behavior of CPMT.
Congenital peribronchial myofibroblastic tumor (CPMT; also known as congenital pulmonary myofibroblastic tumor) is a rare, benign spindle cell neoplasm of the lung found in newborns and fetuses. The disease entity was first proposed in 1993 by McGinnis et al.1 after having been reported under various categories, such as bronchopulmonary fibrosarcoma,2,3 bronchopulmonary leiomyosarcoma,4,5 congenital mesenchymal malformation,6-8 and harmartoma.9 There have been 16 reports of CPMT including those under different designations (Table 1).2,3,5-10 We present a case of CPMT in a Korean patient. This case has been tabulated in our previous report summarizing 22 pediatric lung tumors.11

Clinicopathologic features of CPMT
CASE REPORT
The patient was a female infant born at 38 weeks gestation by Caesarian section without prenatal complications. At one month of age, a right lung lesion was discovered on a chest X-ray taken for evaluation of prolonged diarrhea. Subsequent computed tomography scan at 47 days of age showed a large solid and cystic mass involving the right middle lobe and the right lower lobe of the lung (Fig. 1). With the radiologic impression of mesenchymal tumor or pleuropulmonary blastoma, the baby presented to our institution for further management. At admission, the baby at 80 days of age had no respiratory or gastrointestinal symptoms, and no abnormality was noted on laboratory tests. Four days later, a thoracotomy with right middle and lower bilobectomy was performed to remove the lung mass. The mass extended into the diaphragm, but it was dissectible without causing a defect in the diaphragm. The patient received no further treatment after the surgery and had been healthy without evidence of recurrence for two years until lost to follow-up.
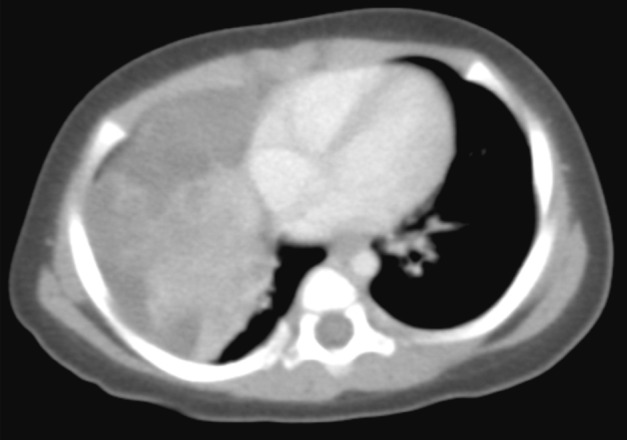
Computed tomography scan image shows a solid and cystic mass in the right hemithorax.
On gross examination, the lung showed a partially necrotic solid mass, which measured 5.5×5×4 cm out of the 11×6×5 cm-sized bilobectomy specimen. The cut surface of the solid portion was white to pink with a trabeculated area and cartilaginous foci (Fig. 2A). The border with the lung parenchyma was indistinct in some areas. Microscopically, the tumor was in irregular shape consisting of three components (Fig. 2B). Fascicles of monotonous spindle cells constituted the largest portion (Fig. 3A). The cords and nodules of spindle cells infiltrated the lung parenchyma at the tumor boundary. The second component was broad irregular plates of mature cartilage, which were associated with airways. The third component was sheets of round to polygonal cells enriched with vascular channels, comparable to a hemangiopericytoma-like pattern (Fig. 3B). These round cells were distributed near the foci of necrosis/hemorrhagic degeneration with gradual transformation from spindle cells. Higher cellularity with a moderate degree of nuclear pleomorphism was observed in the round cell area, in which the mitosis was counted to be as many as eight per ten high power fields (hpf). Additionally, rare foci of adipose tissue were observed at the periphery of the tumor (Fig. 2B). The bronchial resection margin and the visceral pleura were involved by the tumor. The background lung parenchyma was unremarkable.
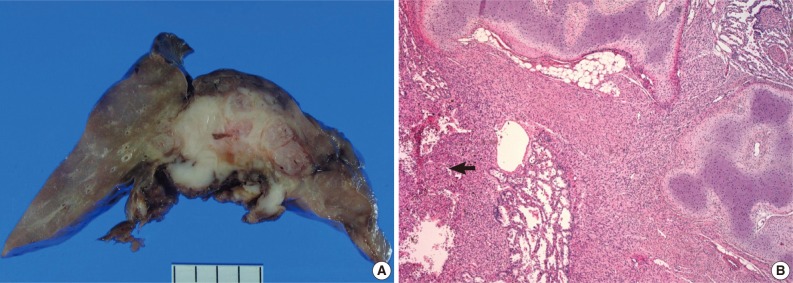
(A) Grossly, the cut surface shows a white to pink fibrous tumor with a fascicular pattern and cartilage component. (B) Low-power microscopic view showing the cartilage, spindle cell and round cell (arrow) components of the tumor. Adipose tissue is also included.
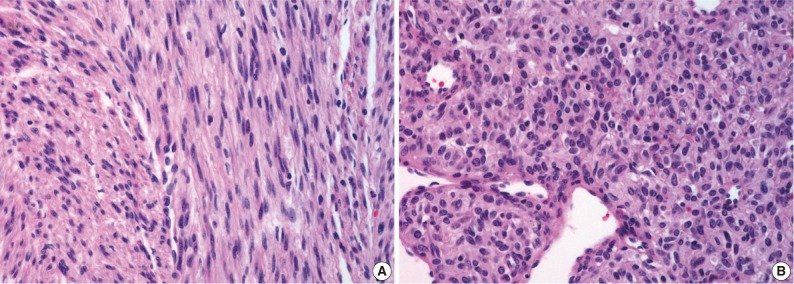
(A) Spindle cell area showing intersecting fascicles of monotonous cells. (B) Round cell area with hemangiopericytoma-like vascular pattern.
Immunohistochemical study showed that the spindle cell and the round cell were positive for vimentin, but only the spindle cell was strongly reactive for smooth muscle actin (Fig. 4). Ki-67 staining was positive in about 1% and 5% in the spindle cell and round cell areas, respectively. The chondrocytes in the cartilage component were positive for S-100. Desmin, cytokeratin, epithelial membrane antigen, and factor VIII were negative in the tumor. On electron microscopic examination of spindle cell areas (Fig. 5), uniform oval to polygonal cells with smooth cell borders and occasional primitive intercellular junctions were observed. The cytoplasm was abundant and contained rough endoplasmic reticulum of variable density, mitochondria, free ribosomes and a few foci of dense bodies with cytoplasmic filaments. Pinocytotic vesicles or basal lamina were also observed. These findings indicate primitive mesenchymal cells with partial myofibroblastic differentiation, which is compatible with the expression of vimentin and smooth muscle actin.
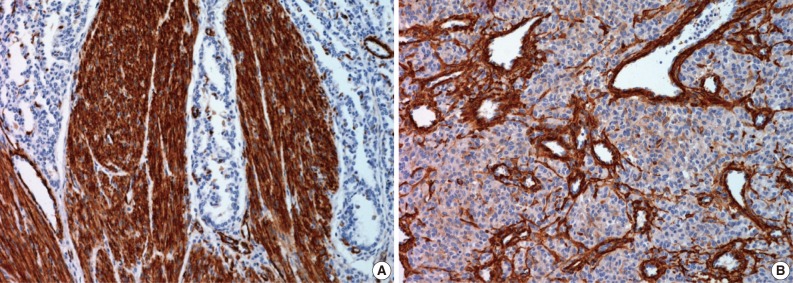
(A) Strong smooth muscle actin positivity in the spindle cells contrasting with the background lung parenchyma. (B) Round cells show faint to zero reactivity to smooth muscle actin.
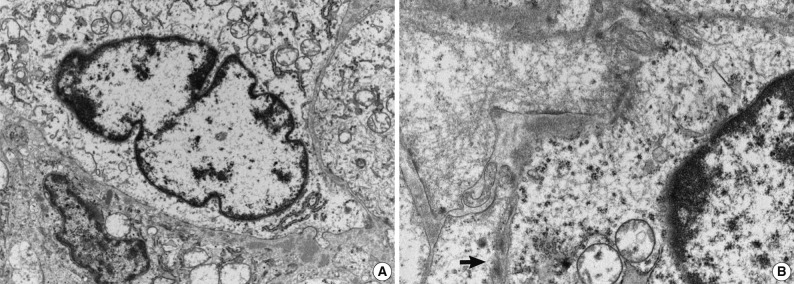
Electron micrographs of (A) the spindle cell area (×10,000) and (B) cells showing cytoplasmic microfilaments with a dense body (arrow) (×20,000).
DISCUSSION
The microscopic pattern of CPMT spans from that of uniform spindle cells4,12,13 to that harboring peribronchial cartilage proliferation6,9,14-16 and/or having a hemangiopericytoma-like area.2,10,17 The phenotype of the tumor cells has been related to that of myofibroblasts or fibroblasts, with variable reactivity to smooth muscle actin or muscle specific actin1,2,10,12-17 and the variable presence of cytoplasmic filaments in electron microscopy. 1,2,4,7,15,17 McGinnis et al.1 have proposed that the tumor arises from primitive peribronchial mesenchyme that may differentiate to form smooth muscle and cartilage. A recent account of CPMT provided supporting evidence for this notion by demonstrating the differentiating tendency in the histology of the same tumor obtained by fetal surgery and postnatal surgery.16 Over the four-month interval of observation, the authors noted decreased cellularity of the spindle cell component and increased proportion and maturation of the cartilage component of the tumor.16 The current case is unique in presenting a tumor in an infant, while all previous reports described tumors from the perinatal period (Table 1). The prominence of the cartilage component in the current case is also supportive of the proposed differentiating potential of the tumor.
Since CPMT has been known to manifest certain features of malignant neoplasm, such as frequent mitosis (greater than 10/10 hpf2,5,7), necrosis,2,12,13,17 and infiltrative growth, some CPMT cases have been reported as malignant entities, such as bronchopulmonary fibrosarcoma2,3 and bronchopulmonary leiomyosarcoma.4,5 However, this neoplasm is benign, as it has not recurred or metastasized in patients surviving through the tumor-removal operation, even with positive surgical resection margins (current case and Huppmann et al.16). The tumor has been mostly associated with hydrops fetalis and neonatal respiratory distress, which has led to in utero and perinatal morbidity and mortality. The current case is among the rare instances3,10 in which the patient was asymptomatic at detection. Cytogenetic analysis of CPMT was conducted in a few reports,1,16,17 and complex chromosomal rearrangements were shown in one.17
The differential diagnosis of CPMT has been extensively discussed in previous reports.1,10,14 Two entities deserve recapitulation for the current case. The solid, type III pleuropulmonary blastoma may show sheets of spindle cells, chondroid foci and necrosis. Unlike CPMT, pleomorphic and anaplastic cells are characteristic, and the clinical course is that of malignancy.18 Bronchopulmonary fibrosarcoma is a low-grade malignancy, which presents as an endobronchial or intraparenchymal mass consisting of bundled spindle cells. Among 30 pediatric cases reported in the literature,2,19,20 four of five neonatal cases have been reclassified as CPMT.1,13 The recent, fifth neonatal case20 may also be considered a CPMT as it was composed of monotonous spindle cells with a high mitotic rate (20/10 hpf) and had not recurred during the 16-month follow-up. It has been suggested that CPMT and pediatric bronchopulmonary fibrosarcoma may be in a spectrum of the same neoplasm.1,14
As CPMT shows good prognosis once adequately resected, it is important not to misdiagnose it as a malignant neoplasm, thereby subjecting the patient to unneeded chemotherapy or radiation therapy. The current case is notable in that it may be one of the most malignant-appearing CPMT cases reported, as it was characterized by a high mitotic rate, necrosis and invasion of the diaphragm.
Acknowledgments
We thank Dr. Yeon-Lim Suh for help with electron microscopic examination.
Notes
No potential conflict of interest relevant to this article was reported.