E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(4); 2014 > Article
-
Brief Case Report
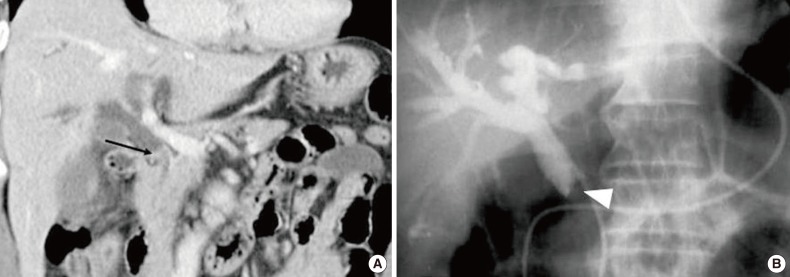
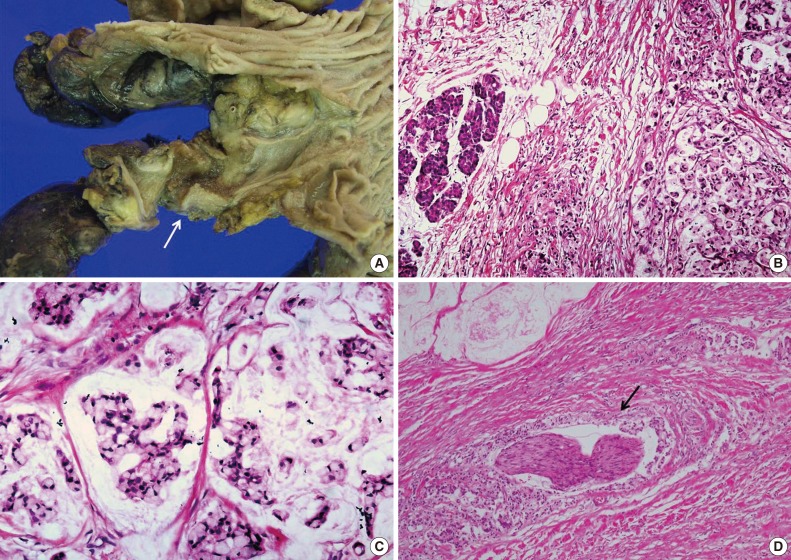
Signet-Ring Cell Carcinoma of the Distal Common Bile Duct: Report of a Case - Hyung Jun Kwon, Ghil-Suk Yoon1, Yong Chul Kwon2, Sang Geol Kim, Ji Yun Jeong1
-
Korean Journal of Pathology 2014;48(4):315-318.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.4.315
Published online: August 26, 2014
Department of Surgery, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, Daegu, Korea.
1Department of Pathology, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, Daegu, Korea.
2Department of Pathology, Catholic University of Daegu School of Medicine, Daegu, Korea.
-
Corresponding Author: Sang Geol Kim, M.D. Department of Surgery, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, 807 Hoguk-ro, Buk-gu, Daegu 702-210, Korea. Tel: +82-53-200-2703, Fax: +82-53-200-2027, 'ksg@knu.ac.kr'
Corresponding Author: Ji Yun Jeong, M.D. Department of Pathology, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, 807 Hogukno, Buk-gu, Daegu 702-210, Korea. Tel: +82-53-420-3391, Fax: +82-53-200-2027, 'jjiyun@gmail.com'
• Received: September 30, 2013 • Revised: February 23, 2014 • Accepted: February 27, 2014
© 2014 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
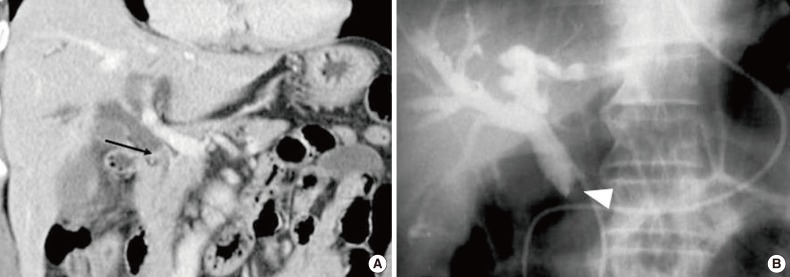
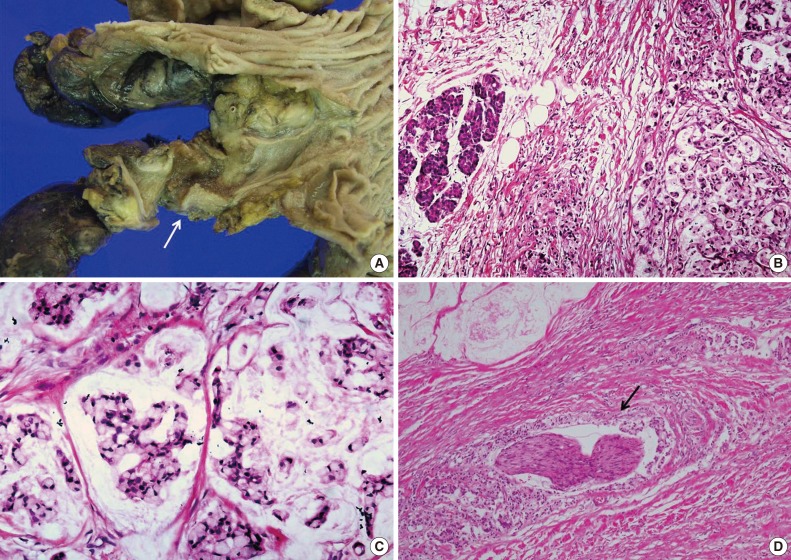
Figure & Data
References
Citations
Citations to this article as recorded by 
- Rare histotypes of epithelial biliary tract tumors: A literature review
Elena Sapuppo, Oronzo Brunetti, Dalila Tessitore, Giovanni Brandi, Nicola Di Giovanni, Guido Fadda, Claudio Luchini, Maurizio Martini, Davide Quaresmini, Antonio Russo, Mariacarmela Santarpia, Aldo Scarpa, Mario Scartozzi, Giovanni Tuccari, Tindara Franch
Critical Reviews in Oncology/Hematology.2023; 181: 103892. CrossRef - Primary signet-ring cell carcinoma of the extrahepatic bile duct: A case report
Chao-Bang Xie, Yang Wu, Feng Li, Kai-Fei Zhao, Rong-Shu Shi, Qiong Huang, Jin Ao, Di Ke
World Journal of Gastrointestinal Oncology.2022; 14(7): 1356. CrossRef - Duodenal Stenosis Due to Carcinoma of the Lower Bile Duct: A Case Report
Takumi Maki, Atsushi Irisawa, Kenji Notohara, Goro Shibukawa, Ai Sato, Akane Yamabe, Yoshitsugu Yoshida, Shogo Yamamoto, Nobutoshi Soeta, Takuro Saito
Clinical Medicine Insights: Case Reports.2020; 13: 117954762091945. CrossRef - Rapidly Progressing Primary Extrahepatic Bile Duct Signet-Ring Cell Carcinoma in a Caucasian Woman
Jessemae L. Welsh, Omar Jaber, Marina Ivanovic, Frederick C. Johlin, Rami G. El Abiad, Gerald H. Clamon, Mark C. Smith, Carlos H. F. Chan
Journal of Gastrointestinal Cancer.2018; 49(1): 63. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-