E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(4); 2013 > Article
-
Case Study
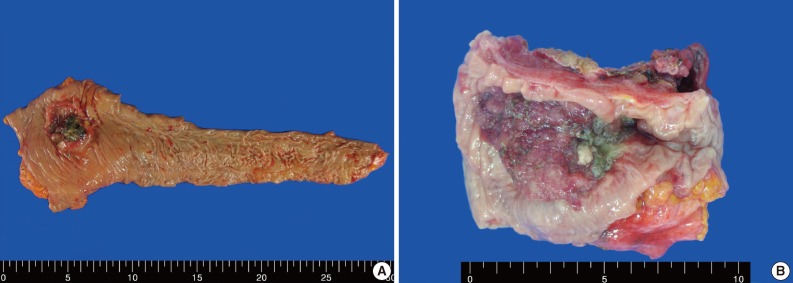
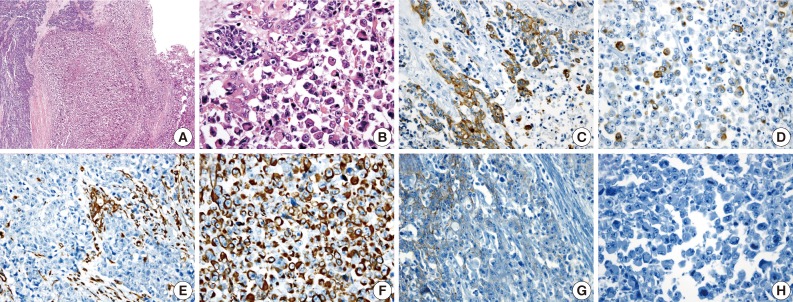
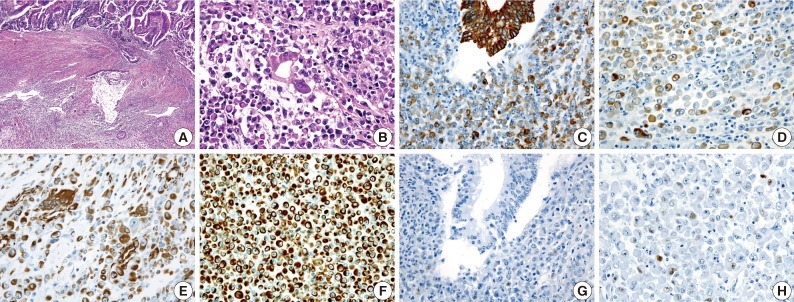
Rhabdoid Colorectal Carcinomas: Reports of Two Cases - Sang Hwa Lee, Hyesil Seol1, Wook Youn Kim1, So Dug Lim1, Wan Seop Kim1, Tae Sook Hwang1, Hye Seung Han1
-
Korean Journal of Pathology 2013;47(4):372-377.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.4.372
Published online: August 26, 2013
Department of Pathology, Research Center, Aerospace Medical Center, Republic of Korea Air Force, Cheongju, Korea.
1Department of Pathology, Konkuk University School of Medicine, Seoul, Korea.
- Corresponding Author: Hye Seung Han, M.D. Department of Pathology, Konkuk University School of Medicine, 120-1 Neungdong-ro, Gwangjin-gu, Seoul 143-729, Korea. Tel: +82-2-2030-5644, Fax: +82-2-2030-5629, 'aphsh@kuh.ac.kr'
• Received: August 20, 2012 • Revised: September 24, 2012 • Accepted: October 8, 2012
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
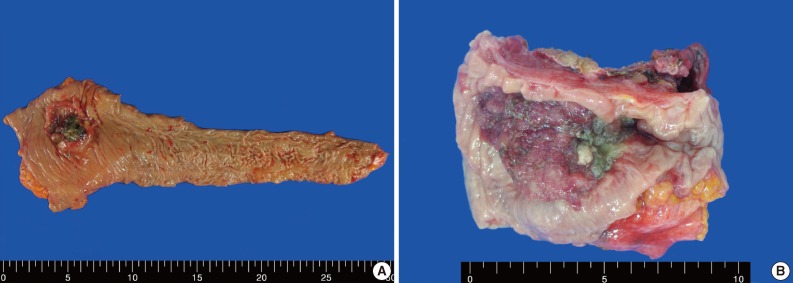
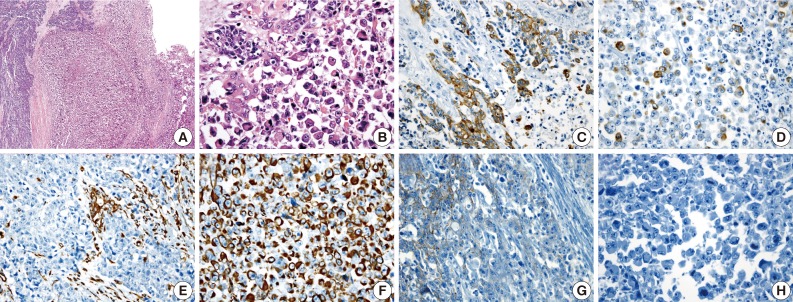
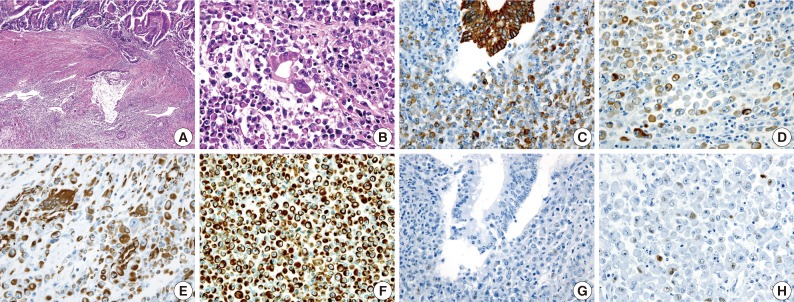
Figure & Data
References
Citations
Citations to this article as recorded by 
- SMARCB1/INI1-Deficient Poorly Differentiated Carcinoma of the Colon With Rhabdoid Features—A Rare Tumor With Serrated Phenotype: Case Report and Review of Literature
Shivali Maurya, Sujata Yadav, Subham Bhowmik, Jasmine Dhal, Lalita Mehra, Raju Sharma, Asuri Krishna, Atul Sharma, Adarsh Barwad, Prasenjit Das
International Journal of Surgical Pathology.2024; 32(1): 187. CrossRef - Emerging and under-recognised patterns of colorectal carcinoma morphologies: a comprehensive review
Yuho Ono, Osman Yilmaz
Journal of Clinical Pathology.2024; : jcp-2023-208816. CrossRef - A Rare Case of Undifferentiated Rhabdoid Carcinoma of the Colon
Syed Alishan Nasir, Ronak Patel, Lalaine Ruiz, Michael Bush
Cureus.2022;[Epub] CrossRef - INI1-negative colorectal undifferentiated carcinoma with rhabdoid features and postoperative rapidly growing liver metastases: a case report and review of the literature
Masatsugu Kojima, Toru Miyake, Tomoyuki Ueki, Hiroyuki Ohta, Ryoji Kushima, Masanori Shiohara, Hiroo Mizuta, Hiroya Iida, Tsuyoshi Yamaguchi, Sachiko Kaida, Katsushi Takebayashi, Hiromitsu Maehira, Yusuke Nishina, Tomoharu Shimizu, Eiji Mekata, Masaji Tan
Surgical Case Reports.2021;[Epub] CrossRef - Undifferentiated carcinoma of the transverse colon with rhabdoid features that developed during treatment of non-small cell lung carcinoma with pembrolizumab: a case report
Yuya Ashitomi, Mitsuhiro Yano, Michihisa Kono, Takefumi Suzuki, Ichiro Kawamura, Shinji Okazaki, Yukinori Kamio, Osamu Hachiya, Yuka Urano, Fuyuhiko Motoi
Surgical Case Reports.2020;[Epub] CrossRef - BRAF Mutation in Colorectal Rhabdoid and Poorly Differentiated Medullary Carcinomas
Bolzacchini, Digiacomo, Marrazzo, Sahnane, Maragliano, Gill, Albarello, Sessa, Furlan, Capella
Cancers.2019; 11(9): 1252. CrossRef - Pathologic complete response to bevacizumab-FOLFIRI in metastatic colonic undifferentiated carcinoma with rhabdoid features
Tien-Chan Hsieh, Hung-Wei Liu, Chao-Wen Hsu
Journal of Cancer Research and Practice.2019; 6(3): 140. CrossRef - Extraordinary disease-free survival in a rare malignant extrarenal rhabdoid tumor: a case report and review of the literature
Francesco D’Amico, Alessandra Bertacco, Maurizio Cesari, Claudia Mescoli, Giorgio Caturegli, Gabriel Gondolesi, Umberto Cillo
Journal of Medical Case Reports.2018;[Epub] CrossRef - Tumor rabdoide extrarrenal maligno de colon: presentación de 3 casos y revisión de la literatura
María José Sánchez-de las Matas Garre, José García Solano, Pablo Conesa Zamora, Fidel Fernández Fernández, Miguel Pérez-Guillermo
Revista Española de Patología.2016; 49(2): 119. CrossRef - Poorly differentiated cecal adenocarcinoma showing prominent rhabdoid feature combined with appendiceal mucinous cystadenoma: A case report and review of the literature
IN-JU CHO, SUNG-SOO KIM, YOUNG-DON MIN, MUN-WHAN NOH, RAN HONG
Oncology Letters.2015; 9(4): 1527. CrossRef - A Rare Case of Undifferentiated Carcinoma of the Colon with Rhabdoid Features: A Case Report and Review of the Literature
E. Moussaly, J. P. Atallah
Case Reports in Oncological Medicine.2015; 2015: 1. CrossRef - Case Report of Rhabdoid Colon Cancer and Review of Literature
Aparna Kalyan, Gurleen Pasricha, Dulabh Monga, Aatur Singhi, Nathan Bahary
Clinical Colorectal Cancer.2015; 14(1): e5. CrossRef - Malignant Rhabdoid Tumor of the Colon: A Case Report
Elena Romera Barba, Ainhoa Sánchez Pérez, Carlos Duque Pérez, José Antonio García Marcilla, José Luis Vázquez Rojas
Cirugía Española (English Edition).2014; 92(9): 638. CrossRef - Tumor rabdoide maligno de colon: a propósito de un caso☆
Elena Romera Barba, Ainhoa Sánchez Pérez, Carlos Duque Pérez, José Antonio García Marcilla, José Luis Vázquez Rojas
Cirugía Española.2014; 92(9): 638. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-