Solitary Myofibroma of the Adult Mandible: A Case Report and Review of Literature
Article information
Myofibroma is a rare benign neoplasm of myofibroblastic cells that can occur in either a solitary or multicentric form. Both forms were described as infantile myofibromatosis because of its multiplicity, typical age distribution (first decade of life), and frequent involvement of deep structures, including the central nervous system and visceral organs such as lung, heart, gastrointestinal tract, liver, kidney, and pancreas.1 In contrast to the multicentric form, solitary myofibroma usually presents as a cutaneous or subcutaneous mass of the head and neck region.2 Intraosseous lesions are much less common, although three studies in 1995 and one in 2000 reported the mandible as a frequent oral site (16 of 36 [or 44%],3 15 of 35 [or 42.6%],4 and 30 of 79 [or 38.0%]).5 Solitary myofibroma of the adult mandible, however, is extremely rare, and only four cases exist within the literature.6 The case of a 31-year-old woman with a symptomless solitary myofibroma arising in the mandible is discussed here. To the best of our knowledge, this is the first report of a solitary myofibroma arising in the adult mandible in Korea.
CASE REPORT
A 31-year-old woman was referred to the Department of Oral and Maxillofacial Surgery, Chungbuk National University Hospital, with a radiolucent lesion in the right mandible that had been noticed by a general dentist during routine check-up. She had not felt any discomfort and had been completely unaware of the lesion. An examination did not detect any recognizable abnormalities, such as mucosal bulging, local tenderness, tooth mobility, or palpable lymph nodes. An orthopantomogram and a facial bone computed tomography revealed a 2.5-cm-sized cystic lesion in the right mandibular alveolar process that formed the root of the first molar (Fig. 1A).
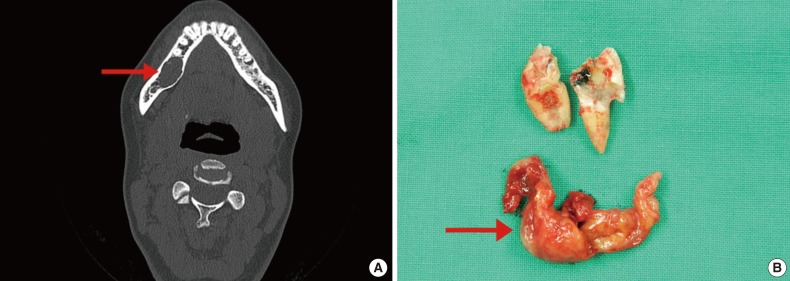
Radiologic evaluations. (A) Facial bone computed tomography reveals a cyst-like lesion in the right mandibular alveolar process of the first molar. (B) During surgery, the first molar is extracted and a solid, firm mass is found under the molar (arrow).
During surgery, a 2.5-cm-sized solid mass arising in the right first molar root was found in the mandibular process. After removing the right first molar tooth, the mass was enucleated along with a 1 to 2 mm margin of normal-appearing bone. The mass was well-circumscribed, did not adhere to the surrounding tissue, and had a rubbery consistency (Fig. 1B).
Microscopic examination revealed a well-defined round mass that consisted of mainly spindle cells and a relatively small portion of round-shaped cells with an ambiguous biphasic pattern intermingled with cleft-like angulated vascular spaces (Fig. 2A). The myoid spindle cells were arranged in interlacing fascicles and had blunt-ended or tapered nuclei with a relatively dense eosinophilic cytoplasm (Fig. 2B). When Masson's trichrome stain was done, the tumor revealed considerable collagenous stroma intermixed with the myofibroblastic cells (Fig. 2C). Immunohistochemistry revealed that the spindle cells were positive for smooth muscle actin (SMA; 1:150, Leica, Newcastle upon Tyne, UK), which had a strong, diffuse, and unequivocal distribution (Fig. 3A). As the tumor had a hemangiopericytoma-like vascular pattern, staining for CD34 (1:200, Thermo Fisher Scientific, Waltham, MA, USA) was also performed. Although the tumor was negative for this antigen, prominent slit-like blood vessels were revealed (Fig. 3B). In addition, the tumor cells did not exhibit immunoreactivity to S100 (1:800, DAKO, Glostrup, Denmark), CD117 (1:500, DAKO), human melanoma black 45 (1:100, Leica), estrogen receptor (1:50, Leica), or progesterone receptor (1:200, Leica). The Ki-67 (1:50, DAKO) proliferation index was approximately 1% throughout the tumor, which indicates a very low proliferative nature. To differentiate the myofibroma from smooth muscle tumor, desmin (1:100, Leica), h-caldesmon (1:100, DAKO), and vimentin (1:200, DAKO) stains were done; the tumor showed strong positivity for vimentin only (Fig. 3C). Based on the above findings, the diagnosis of an intraosseous myofibroma was made.
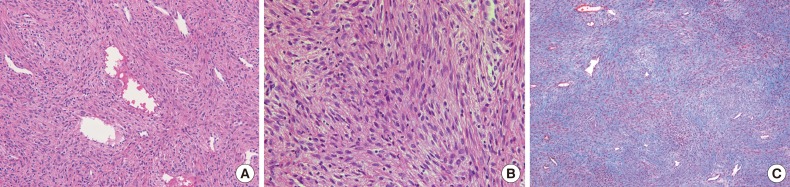
Microscopic and special staining features. (A) The tumor is highly cellular and exhibits an interlacing fascicle pattern with slit-like blood vessels. Neither atypical mitosis nor necrosis are detected. (B) A high-power view reveals spindle cells with elongated nuclei and blunted-ends closely resembling smooth muscle tumors. (C) Masson's trichrome stain shows plenty of collagenous stroma (blue stain) intermingled with myofibroblastic cells (red stain).
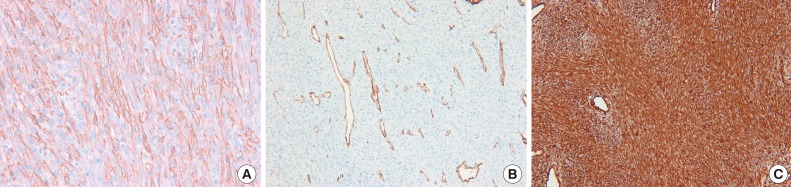
Immunohistochemical stains. (A) Smooth muscle actin is expressed diffusely and strongly in spindle cells. (B) CD34 demonstrates hemangiopericytoma-like vascular pattern. (C) Vimentin is diffusely and strongly positive in all around the tumor cells.
DISCUSSION
Myofibroma and myofibromatosis are rare benign mesenchymal neoplasms composed of contractile myofibroblastic cells arranged around thin-walled blood vessels with a predilection for the head, neck, and perioral structures.1 In the WHO Classification of tumours of soft tissue and bone revised in 2013, myofibroma was classified as a perivascular tumor, as well as angioleiomyoma.1
Radiologic feature of myofibroma involving the mandible is a radiolucent lesion, of which 70% are unilocular and 30% are multilocular with a well-defined border. Microscopically, myofibroma is a nodular, well-circumscribed neoplasm, characterized by biphasic growth of 1) immature-appearing, plump, spindled tumor cells showing oval nuclei and scant cytoplasm with numerous thin-walled, branching hemangiopericytoma-like vessels; and 2) more mature spindled tumor cells that possess eosinophilic cytoplasm and elongated, blunt-ended or tapered nuclei, arranged in bundles or whorls. Tumor cells are often set in a collagenous stroma with characteristic myxohyaline changes. Mitoses are variable in number; especially in immature-appearing tumors, numerous mitoses as well as areas of necrosis may be present.4 Myofibroma should be differentiated from leiomyoma, neurofibroma, nodular fasciitis, hemangiopericytoma, and fibrosarcoma due to their macroscopic and microscopic similarites.2,6,10
Because myofibromas are composed of cigar-shaped spindle cells that both resemble smooth muscle tumor and stain positive for SMA, myofibromas may easily be misdiagnosed as smooth muscle tumor.6 Moreover, due to its rarity, myofibromas may be missed by general surgical pathologists in the differential diagnosis of tumors arising in the mandible.
As both leiomyoma and myofibroma show immunoreactivity for SMA, immunohistochemical evaluation should be used to support the diagnosis of myofibroma. The myoid spindle cells of myofibroma are more likely to be immunoreactive for SMA and vimentin than the spindle cells of leiomyoma; the spindle cells in myofibroma are negative for desmin and caldesmon, whereas the spindle cells in leiomyoma are positive for the two markers. In addition, myofibroma and smooth muscle tumors demonstrate different characteristic patterns in Masson's trichrome stain; myofibroma is composed of much more collagenous stroma intermixed with the spindle cells than smooth muscle tumor is.10
Myofibroma of the mandible is a tumor typically occurring in children (mean, 7.2 years; median, 6 years), usually in the first decade of life, with definite male predominance (male:female ratio, 2.3:1). However, solitary myofibroma of the adult mandible is extremely rare with only four cases having been reported.6 The age of presentation ranged from 20 to 43 years (mean, 32 years; median, 32 years) with striking female predominance (male:female ratio, 1:4), as was seen in our case (Table 1).
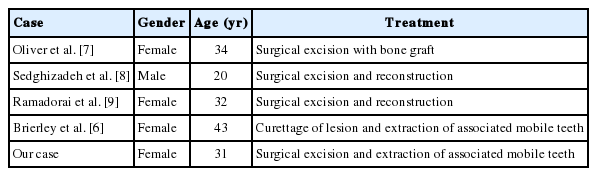
Clinicopathologic features of five cases of solitary myofibroma of the adult mandible
The recurrence rates for myofibromas are quite low, ranging from 0% to 12.5%. Recurrences can be attributed to tumors with difficult surgical access or incomplete removal. Smaller lesions can regress spontaneously, and observation might be warranted in those cases.
In summary, solitary myofibroma of the adult mandible is exceedingly rare, and surgical excision is the treatment of choice as recurrence is uncommon after complete resection. Owing to their similarities of individual cell morphology and general architecture, smooth muscle tumor can be one of the most difficult differential diagnoses. Therefore, use of appropriate immunohistochemical markers for smooth muscle differentiation, such as desmin and h-caldesmon, is recommended. Awareness of myofibroma arising in the mandible also may lower the possibility of misdiagnosis.
Notes
No potential conflict of interest relevant to this article was reported.