Causes of necrotic features in fine-needle aspirates from cervical lymph nodes
Article information

Abstract
Background
Lymph node fine-needle aspiration (LN FNA) cytology indicates necrosis in various diseases. Dominant necrotic features make the diagnosis of underlying conditions very difficult.
Methods
We retrospectively reviewed 460 patients who underwent cervical LN aspiration cytology that revealed necrotic findings at Keimyung University Dongsan Hospital in Daegu, Korea, from 2003–2017. Each specimen was evaluated and analyzed in association with the clinical findings, biopsy findings, and/or other ancillary tests, including acid-fast bacilli staining and molecular testing for Mycobacterium tuberculosis.
Results
When necrotic features were noted upon cervical LN FNA cytology, the most common pathologic LN FNA category was necrosis alone (31.5%). The second most common category was granulomatous inflammation (31.3%), followed by Kikuchi disease (20.0%) and malignant neoplasm (8.7%). In cases where the cervical LN FNA revealed necrosis alone, the most common final diagnosis was tuberculosis. In young patients, Kikuchi disease should be considered as one cervical LN FNA category, while metastatic carcinoma should be suspected in older patients.
Conclusions
Even when necrosis alone is observed in LN FNA cytology, it is important to determine the cause through further evaluation.
Fine-needle aspiration (FNA) is an excellent, minimally invasive diagnostic technique for evaluating a mass or lesion. In particular, FNA is commonly used for evaluating enlarged lymph nodes (LNs). In many cases, the aspirate can provide conclusive evidence for a diagnosis; sometimes, the cytology reveals only necrosis.
Necrosis of LNs is found in various diseases. Malignant neoplasms (including lymphomas and metastatic carcinomas) must first be excluded. In addition, numerous benign conditions, such as tuberculosis (TB) and Kikuchi disease, also cause LN necrosis. When necrosis is identified in an LN FNA cytology sample, pathologists should consider various entities and attempt to find clues that lead to a final diagnosis. However, LN FNA cytology sometimes reveals necrosis alone, and few studies have investigated this situation.
The aim of this study was to evaluate the causes of necrosis in FNA of enlarged LNs.
MATERIALS AND METHODS
We searched the electronic medical record system of the Keimyung University Dongsan Hospital from 2003–2017 to find patients who underwent FNA on cervical LNs. We selected cases with a description of necrotic features on the pathology report. In addition, we also collected the clinical parameters of these cases, including patient age, sex, biopsy findings, other ancillary tests for Mycobacterium tuberculosis (MTB; including acid-fast bacilli staining), and molecular studies carried out using conventional polymerase chain reaction (PCR) or real-time PCR. We classified these cases into five categories: granulomatous inflammation, Kikuchi disease, suppurative inflammation, malignant neoplasm, and necrosis only. When granuloma was included in the microscopic description (e.g., granulomatous inflammation with caseous necrosis, granulomatous inflammation with a necrotic background, or necrosis with a vague granuloma), it was classified as granulomatous inflammation. When the LN FNA result contained content that indicated histiocytic necrotizing inflammation, we placed the patient into the Kikuchi disease category. Cases reported as suspicious for Kikuchi disease with various microscopic descriptions (e.g., necrotizing lymphadenitis, polymorphous lymphoid cells, and macrophages on a necrotic background) were classified as Kikuchi disease. Malignant neoplasms (e.g., metastatic carcinoma, metastatic sarcoma, metastatic melanoma, and malignant lymphoma) with a necrotic background were determined to be malignancies. Cases with suppurative inflammation on a necrotic background, acute inflammatory cells on a necrotic background, aspirated pus, or neutrophilic infiltration with necrotic material were classified as suppurative inflammation.
RESULTS
Clinical characteristics of the patients
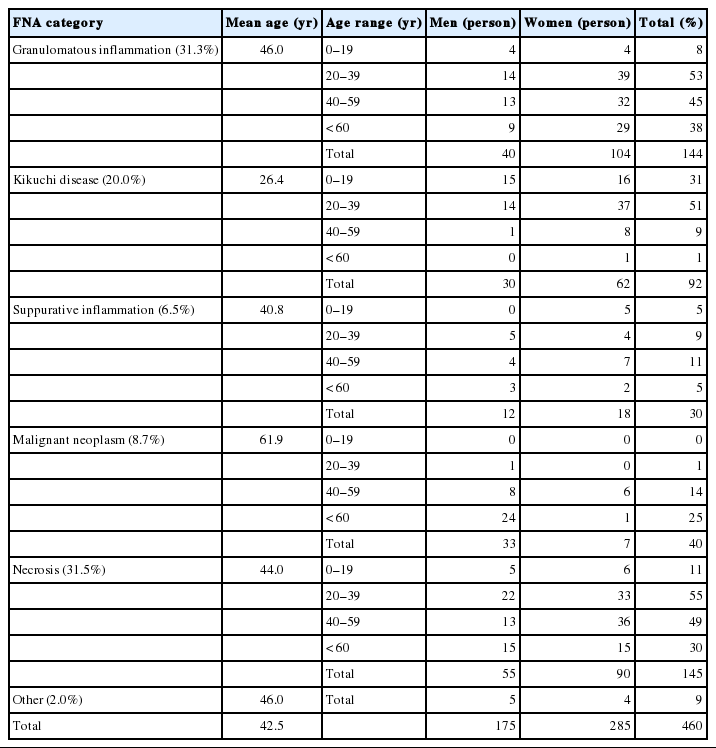
We retrieved the electronic medical reports of 460 patients who underwent LN aspiration cytology at our hospital that revealed necrotic features. The mean age of the patients was 42.5 years (range, 2 to 86 years; median, 40 years). The male-to-female ratio (M:F ratio) was 0.62. Except for cases of pure necrosis, the most common FNA category was granulomatous inflammation (31.3%), followed by Kikuchi lymphadenitis (20.0%), malignancy (8.7%), and suppurative lymphadenitis (6.5%) (Table 1).
The age and sex distribution of cervical LN FNA categories according to the FNA diagnosis
Granulomatous inflammation
Of the 460 patients, 144 were classified with granulomatous inflammation from among the LN FNA categories. The M:F ratio was 0.38. This type of inflammation was mainly distributed in people from 20–39 years of age (36.8%). Of the 144 patients with granulomatous inflammation, 117 underwent ancillary tests for MTB; 82 (70.0%) of these were diagnosed with TB. In addition, MTB testing was performed in 364 of the 460 total cases who underwent cervical LN FNA. Among these patients, 148 cases were MTB-positive, which represented 32% of all cervical LN FNA cases (Table 2).
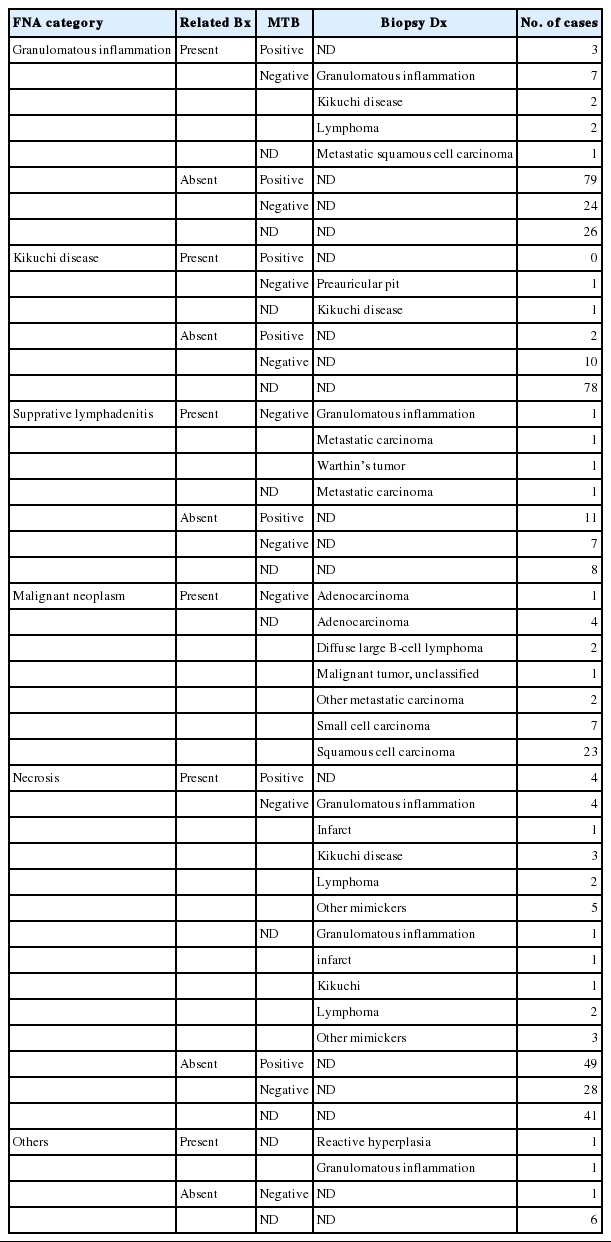
The results of ancillary tests for Mycobacterium tuberculosis in the granulomatous inflammation, Kikuchi disease, suppurative lymphadenitis, malignant neoplasm, and necrosis categories of cervical LN FNA findings
Kikuchi disease
Ninety-two patients who underwent LN FNA were determined to have Kikuchi disease. Of these 92 people, 89.1% were young (< 40 years). The M:F ratio was approximately 1:2. Thirteen of these patients classified as having Kikuchi disease by LN FNA underwent ancillary tests for MTB. Among them, 11 patients were negative, but the remaining two patients had positive results. Therefore, the final diagnosis of 11 patients was TB.
Suppurative lymphadenitis
Of the 460 total patients, 30 (6.7%) were classified with suppurative lymphadenitis. Twenty-five patients (83.3%) were <60 years of age. The M:F ratio was 0.67. Among these 30 patients, 21 underwent ancillary tests for MTB. Eleven patients received a final diagnosis of TB. Four of the 10 patients who were negative for MTB underwent LN biopsy and were finally diagnosed with granulomatous inflammation, Warthin tumor, and metastatic carcinoma (Table 2).
Malignant neoplasm
In 40 patients, malignant neoplasms were classified into distinct LN FNA categories. The average patient age was 61.9 years. The M:F ratio was 4:7. All 40 patients underwent LN biopsies in the same region. Metastatic carcinoma accounted for 92.5% of cases. Among these cases, the incidence of squamous cell carcinoma was 62.2%. Two cases of malignant lymphoma were diffuse large B-cell lymphomas. In young patients, many cases were diagnosed as TB, while some older patients had metastatic carcinoma.
Necrosis alone
Of the 460 cases, 145 were classified as having necrosis alone; 94 cases underwent ancillary testing for MTB, and 53 patients (56.4%) were diagnosed with TB. In addition, 27 patients received an LN biopsy. These remaining cases were finally diagnosed with granuloma, Kikuchi disease, necrosis, lymphomas, and other disorders (Table 2). Seven other mimickers included reactive hyperplasia (n = 2), metastatic papillary carcinoma (n = 1), Warthin tumor (n = 1), salivary duct cyst (n = 1), schwannoma (n = 1), and spindle cell tumor (n = 1) (Fig. 1).
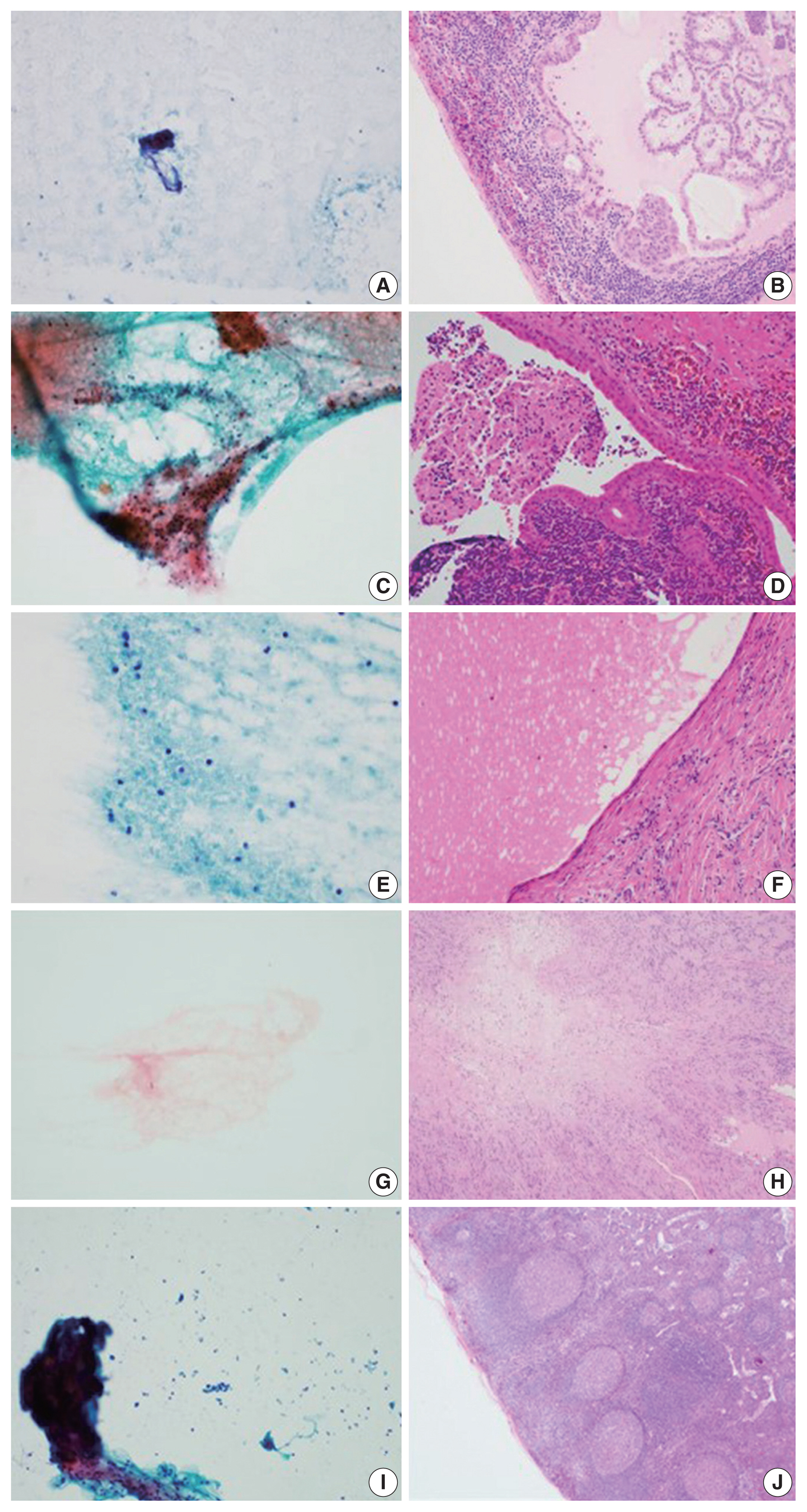
Smear and biopsy findings of the neck lesion diagnosed as necrosis on aspiration but changed diagnosis by biopsy (A, B). (A) Fine needle aspiration (FNA) shows colloid material. (B) Lymph node (LN) excision specimen was diagnosed as metastatic papillary carcinoma. (C, D) Case 2. (C) FNA shows pinkish amorphous material. (D) LN excision specimen was diagnosed as Warthin tumor. (E, F) Case 3. (E) FNA shows cystic fluid material. (F) LN excision specimen was diagnosed as salivary duct cyst. (G, H) Case 4. (G) FNA shows myxoid stroma. (H) LN excision specimen was diagnosed as schwannoma. (I, J) Case 5. (I) FNA shows red blood cells and fibrin material. (J) LN excision specimen was diagnosed as reactive hyperplasia.
DISCUSSION
FNA is frequently performed as a minimally invasive procedure in patients with mass lesions of superficial organs. It is also a very useful test for clinicians to use when deciding on a treatment. However, the FNA cytology slides may offer no diagnostic clues. In some cases, the cellularity is too low and reveals only necrotic material. In these situations, the pathologist faces difficulties in arriving at a diagnosis. Necrosis is common in benign inflammatory lesions as well as in metastatic malignancies. Extensive necrosis is known to accompany not only metastatic malignancy, but also acute inflammation or granulomatous inflammation. In addition, focal necrosis is seen in LNs associated with systemic lupus erythematosus, infectious mononucleosis, and brucellosis [1].
We reviewed the literature on LN FNAs that reveal necrotic features. The most common reports were on TB [2–11], followed by studies on lymphoma [12–19] and metastatic lesions [20–23] (Table 3). However, most of these studies were case reports. There have been very few systematic reports of cases where necrosis is observed or certain diseases must be considered to be more important based on the patient age.
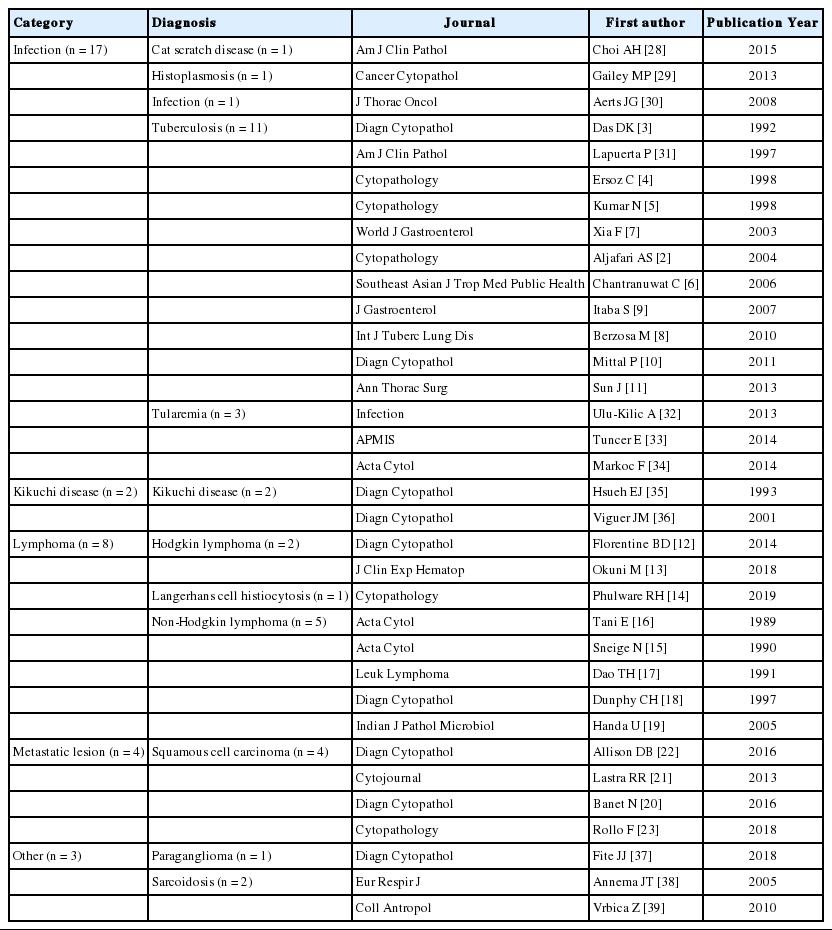
Previously published reports with the keywords “FNA,” “necrosis,” and “lymph node”
In this study, we analyzed 460 patients who underwent cervical LN FNA cytology that revealed necrotic features. The most common causative disease was TB. Of the 460 patients, 247 underwent ancillary testing for MTB, and 148 (59.9%) were finally diagnosed with TB. Typically, the most characteristic cytologic findings of TB are nodular collections of epithelioid histiocytes with Langhans giant cells and caseous necrosis. However, either end of the cytologic spectrum may be seen, especially necrosis without granulomas [24]. Kumar et al. [5] reported that the presence of acute lymphadenitis does not completely exclude TB. They clinically suspected TB in 263 cases with a cytologic picture that demonstrated acute suppurative inflammation. LN FNA should be repeated in all FNA cases that show acute suppurative inflammation without granulomas. It has been reported that a repeat LN FNA helps to detect more than 55% of additional TB cases [25]. In this study, among the patients classified with suppurative lymphadenitis according to FNA cytology, 36.7% were finally diagnosed with TB following ancillary tests. Therefore, it is important to rule out TB when necrotic features are noted on LN FNA cytology.
Necrotic features may also be characteristic of the Kikuchi disease category in cervical LN FNA. The FNA findings in Kikuchi disease typically reveal a polymorphous lymphoid population, crescentic histiocytes, extensive apoptotic bodies, and necrosis. The combination of crescentic histiocytes and karyorrhectic debris suggests the diagnosis of Kikuchi disease. However, some cases show only karyorrhexis and necrosis, which is not specific for Kikuchi disease. For example, infectious mononucleosis may rarely demonstrate extensive necrosis. Infectious mononucleosis is a self-limited viral disease that frequently involves the cervical LNs of young patients who present with fever and pharyngitis. In infectious mononucleosis, a polymorphous infiltrate with atypical large lymphoid cells is usually noted. The patient’s clinical history is helpful in arriving at a differential diagnosis in these cases [26].
Another important cause of necrotic features in cervical LN FNA cytology is malignant neoplasm. Among our 460 cases, 49 were finally confirmed as malignancies (including metastatic carcinoma) by tissue biopsy. The mean age of these patients was 62 years. Forty cases were metastatic carcinoma. Among these cases, the most common malignancy was squamous cell carcinoma (62.5%). This trend was consistent with the findings of previous reports. In squamous cell carcinoma, metastatic LNs of the head and neck are often the first signs of malignancy in the inconspicuous organs of this region [1]. Additionally, cystic changes are often observed in metastatic LNs in squamous cell carcinoma [27]. Necrotic material may also be identified in the cyst spaces; therefore, pathologists should be mindful during their microscopic examinations. In our study, most cases were diagnosed as malignant neoplasms by FNA alone; the remaining nine cases were diagnosed as suppurative lymphadenitis (n = 1), granuloma (n = 3), and necrosis (n = 5) of the LNs. Therefore, when necrotic features are seen in the cervical LN FNA cytology in older patients, pathologists should consider the possibility of malignancy and carefully correlate their findings with the clinical history of the patient to ensure the proper evaluation is recommended to clinicians, even though there may be a paucity of cells on the smeared slides.
In this study, we identified misdiagnosed cases of cervical LN necrosis on FNA. Following an excision biopsy, these cases were diagnosed as reactive hyperplasia, salivary duct cysts, Warthin tumors, schwannomas, and spindle cell tumors. As demonstrated by these cases, fibrinoid material that is present due to excessive hemorrhaging, amorphous material of tumor components, or hypocellular myxoid stroma could be confused with a necrotic background.
An accurate diagnosis on cervical LN FNA cytology is important to determine the most appropriate treatment and to prevent unnecessary surgery. This study was conducted in the Republic of Korea, and we found that the most common cause of necrosis in cervical LN FNA cytology was TB. When there are necrotizing features in the FNA of the cervical lymph nodes in young patients, Kikuchi disease should be considered first. Metastatic carcinoma should always be suspected in older patients, even if they do not have any previous history of malignancy. In addition, when necrotizing features are noted in the FNA of the cervical lymph nodes of patients in any age group, MTB testing should be performed in parallel to exclude TB, which has a high prevalence in the Republic of Korea.
Notes
Ethics Statement
This study was approved by the Institutional Review Board of the Keimyung University Dongsan Hospital with a waiver of informed consent (DSMC 2020-03-069-002) and performed in accordance with the principles of the Declaration of Helsinki.
Author Contributions
Conceptualization: HRJ. Data curation: YJS, HS. Formal analysis: YJS, HRJ. Methodology: YJS, HRJ. Supervision: HRJ. Visualization: YJS, HWL. Writing—original draft: YJS, HRJ. Writing—review & editing: YJS, HS, HWL, HRJ. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
No funding to declare.