The Use of Fine-Needle Aspiration (FNA) Cytology in Patients with Thyroid Nodules in Asia: A Brief Overview of Studies from the Working Group of Asian Thyroid FNA Cytology
Article information
Abstract
Ultrasound-guided fine-needle aspiration (FNA) cytology is the most widely used screening and diagnostic method for thyroid nodules. Although Western guidelines for managing thyroid nodules and the Bethesda System for Reporting Thyroid Cytopathology are widely available throughout Asia, the clinical practices in Asia vary from those of Western countries. Accordingly, the Working Group of Asian Thyroid FNA Cytology encouraged group members to publish their works jointly with the same topic. The articles in this special issue focused on the history of thyroid FNA, FNA performers and interpreters, training programs of cytopathologists and cytotechnicians, staining methods, the reporting system of thyroid FNA, quality assurance programs, ancillary testing, and literature review of their own country’s products. Herein, we provide a brief overview of thyroid FNA practices in China, India, Japan, Korea, the Philippines, Taiwan, and Thailand.
Fine-needle aspiration (FNA) cytology has been widely accepted as a safe, cost-effective, and accurate tool for the preoperative diagnosis of thyroid nodules. In the past, aspirations were performed only with the manual aid. Since FNA under ultrasound guidance proved to be more accurate for the detection of thyroid cancer, FNA should be performed under ultrasound guidance using a 23-, 25-, or 27-gauge needle for cytological evaluation [1,2]. The wide use of FNA cytology for thyroid nodules has significantly decreased the rate of unnecessary surgery for benign thyroid nodules over the last three decades [1,3].
Although North American and European guidelines for managing thyroid nodules and the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) are available throughout Asia, the clinical practices in Asia vary from those of Western countries in terms of disease incidence, diagnostic methods, availability of diagnostic tests, conservative management approach, national health insurance system, and governmental regulations on health care. Moreover, there is considerable variation among Asian countries due to the different rates of economic development and kinds of healthcare systems. Asian countries have increasingly reported their experiences of FNA of thyroid nodules using TBSRTC. Despite these efforts, Asian data on thyroid FNA have not been very well-organized so far. Accordingly, the Working Group of Asian Thyroid FNA Cytology established in 2016 has encouraged group members to publish their work jointly [4].
In this special issue, seven articles from China, India, Japan, Korea, the Philippines, Taiwan, and Thailand jointly focused on the same topic regarding the history of thyroid FNA, FNA performers and interpreters, the training programs of cytopathologists and cytotechnicians, staining methods, the reporting system of thyroid FNA, quality assurance programs, and ancillary testing, added by the comprehensive review of publications released from the individual countries [5-11]. Herein, we provide a brief overview of contemporary thyroid FNA practices based on the review articles from seven Asian countries.
HISTORICAL ASPECTS OF THYROID FINE-NEEDLE ASPIRATION
In the late 1920s, Hayes Martin and Edward Ellis performed aspiration biopsies using an 18-gauge needle for the cytological evaluation of thyroid lesions in the Memorial Hospital of New York [12]. In 1952, thyroid aspiration cytology using a fine needle (diameter of 0.4–0.8 mm) was introduced by Nils Söderström in Sweden [13]. Thyroid FNA was used in routine practice as an accurate test for distinguishing between benign and malignant thyroid nodules in Sweden since the 1950s. In the United States, FNA was not successfully used for the diagnosis of thyroid nodules before 1970s because of the clinician’s preference for surgical biopsies, a lack of familiarity with the FNA procedure, and concerns about tumor seeding along the needle tract [14,15]. After that time, thyroid FNA was reintroduced in the United States and became widely available in the 1980s [14].
In Asia, thyroid FNA was introduced in China and Japan in the 1950s [9,10]. In Korea, India, and Taiwan, thyroid FNA was introduced in the 1970s [5-7,11]. Table 1 summarizes the brief history of thyroid FNA in seven Asian countries [5-11].
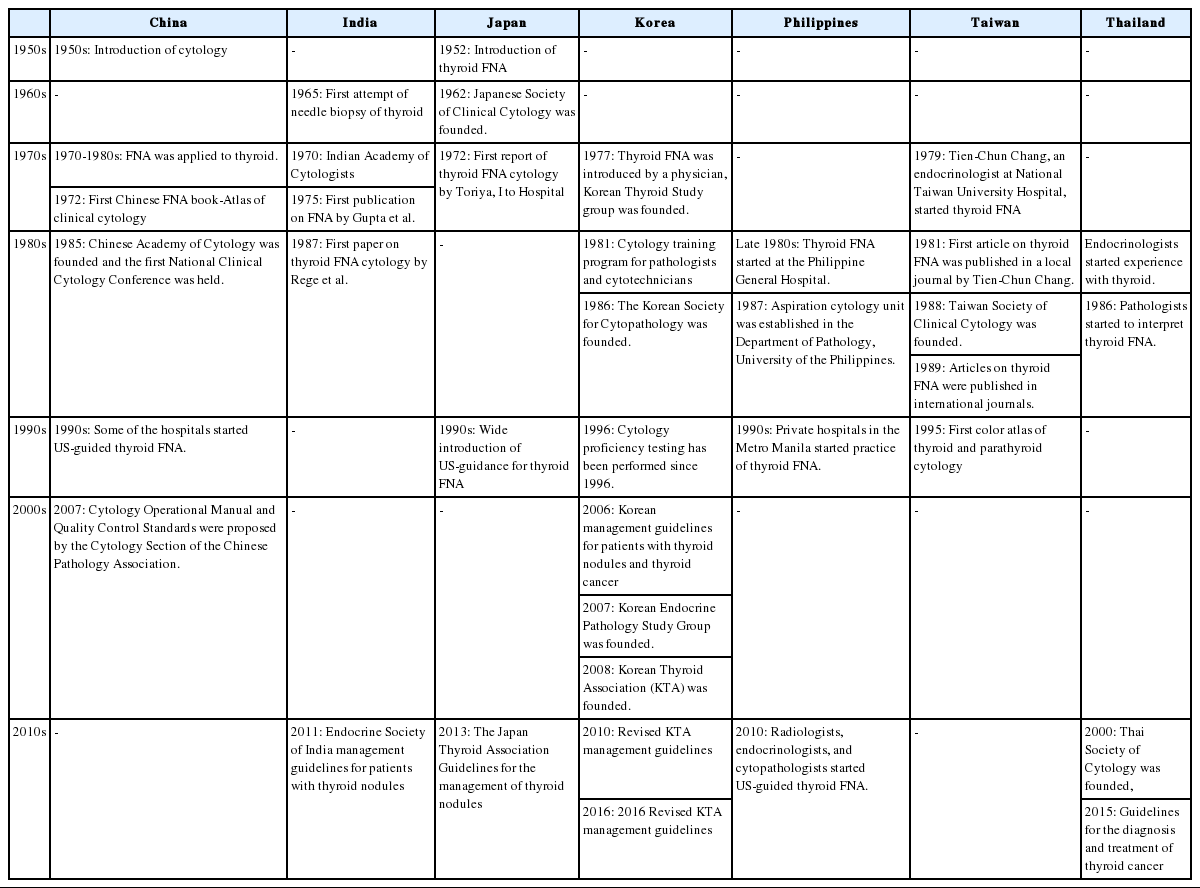
A brief overview of the history of thyroid FNA cytology in Asian countries
PERFORMERS AND INTERPRETERS OF THYROID FINE-NEEDLE ASPIRATION CYTOLOGY
Since thyroid FNA was initially introduced by clinicians in most countries, interpretation of FNA cytology were mostly done by clinicians in the past, including endocrinologists, surgeons, and radiologists. In recent years, thyroid FNA has been performed under ultrasound guidance by clinicians in Japan, Korea, the Philippines, Taiwan, and Thailand. Chinese clinicians prefer an intraoperative frozen section rather than FNA for the diagnosis of thyroid nodules [9]. Thyroid FNA is more frequently performed through palpation rather than ultrasound in India, Thailand, and the Philippines because of limited or delayed access to sonography [5,8,11]. Table 2 summarizes the current practices of thyroid FNA performers and interpreters in seven Asian countries [5-11].
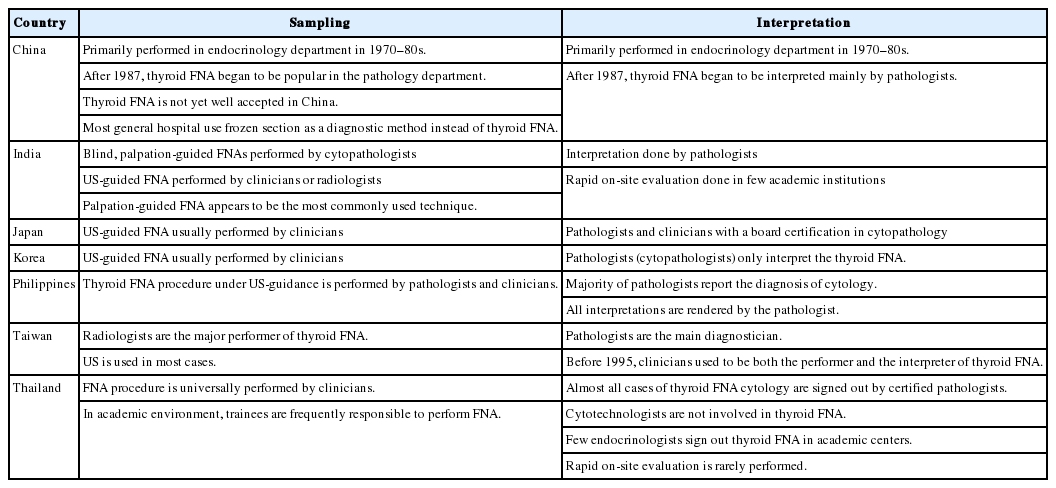
Thyroid FNA performer and interpreter
STAINING METHODS OF THYROID FINE-NEEDLE ASPIRATION CYTOLOGY SAMPLES
The most widely used staining method for thyroid FNA specimens was Papanicolaou stain. Hematoxylin and eosin stain was favored by most Chinese pathologists [9]. In India and Thailand, thyroid FNA samples were stained with a combination of two classical stains: alcohol-fixed smears were stained with Papanicolaou stain and air-dried smears were stained with modified Giemsa stain (e.g., May-Grünwald-Giemsa stain or Diff-Quik stain) [5,8]. Table 3 summarizes the staining methods for thyroid FNA cytology specimens [5-11].
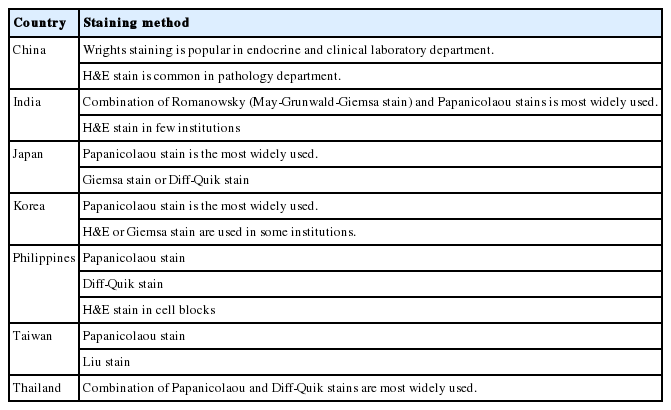
Staining methods for thyroid fine-needle aspiration cytology specimens
REPORTING SYSTEM OF THYROID FINE-NEEDLE ASPIRATION CYTOLOGY
The reporting system of thyroid FNA cytology has improved significantly over the past 10 years with the introduction of TBSRTC [1,3]. TBSRTC consists of six diagnostic categories in order to facilitate communication among cytopathologists and their clinical colleagues and to provide the risk of malignancy for each diagnostic category [3]. After the introduction of TBSRTC, the system has been most widely accepted in China, India, Korea, the Philippines, and Thailand [5,6,8,9]. Other reporting systems for thyroid FNA cytology used in Asia were the General Rules for the Description of Thyroid Cancer by the Japanese Society of Thyroid Surgery, the Japanese System for Thyroid FNA Cytology by the Japan Thyroid Association, and the 6-tier System of Taiwan [7,10]. Table 4 summarized the reporting system of thyroid FNA cytology before and after the introduction of TBSRTC [5-11].
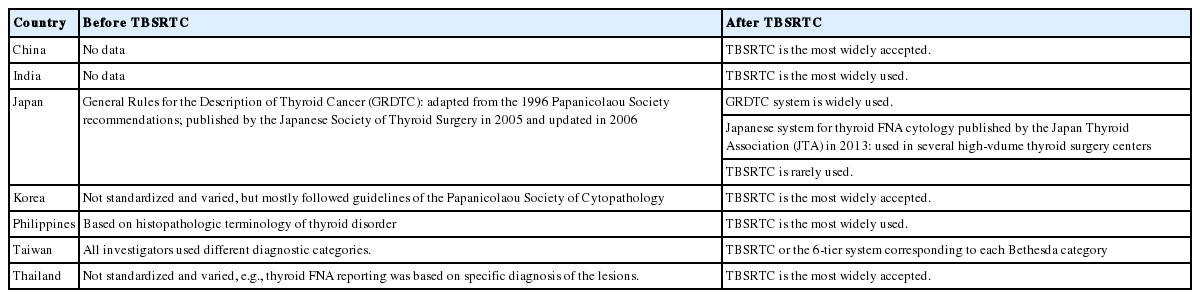
Reporting system of thyroid FNA cytology
NON-DIAGNOSTIC THYROID FINE-NEEDLE ASPIRATION
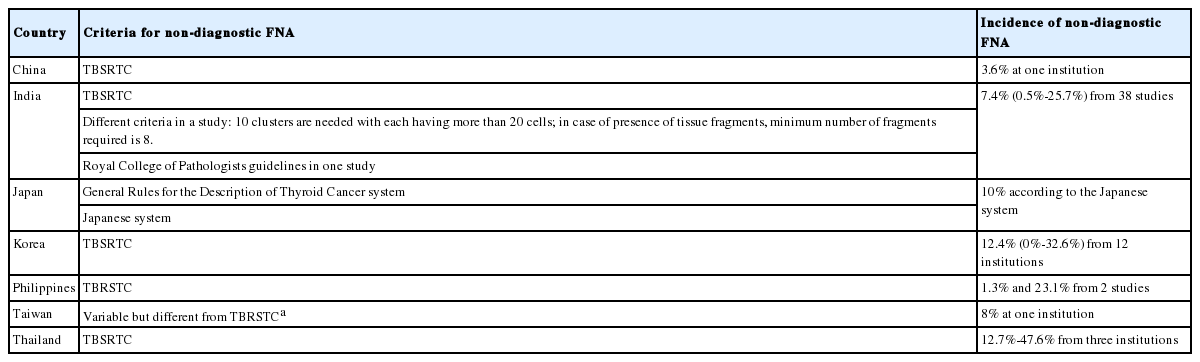
Although ultrasound-guided thyroid FNA has high sensitivity and specificity in distinguishing benign from malignant thyroid nodules, in 1%–40% of cases, thyroid FNA is insufficient for diagnosis and is categorized as non-diagnostic according to TBSRTC [16]. The non-diagnostic FNA cytology by TBSRTC includes virtually acellular specimens (requiring the presence of at least six groups of well-visualized follicular cells with each group containing at least 10 well-preserved epithelial cells), cystic fluid only, and other specimens (obscuring blood, crushed artifacts, poor clotting artifacts, air drying artifacts, overly thick smears, etc.) [3]. In the Japanese system, thyroid FNA with “cystic fluid only” is classified as benign rather than non-diagnostic [10,17]. In Taiwan, a paucicellular specimen with fewer than six groups of ten benign follicular cells is considered benign if it contains more than 50 follicular cells in total or consists of degenerative hemorrhagic cyst fluid and scant benign follicular cells [7].
Table 5 summarizes the criteria and rate of non-diagnostic thyroid FNA [5-11]. A high rate of non-diagnostic aspirates was reported from several teaching hospitals in the Philippines and Thailand, which was linked to the training activity of unskilled residents and limited access to ultrasound guidance [8,11].
Non-diagnostic thyroid FNA
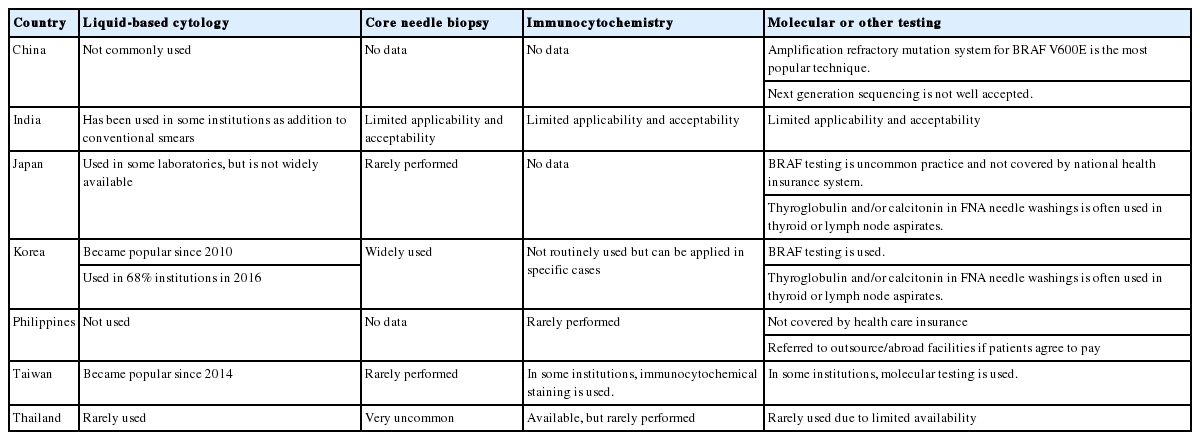
LIQUID-BASED CYTOLOGY AND ANCILLARY TESTS
In Korea, the use of liquid-based cytology in thyroid FNA was adopted in 2008 and became widely used since 2010 [6,18]. In Taiwan, liquid-based cytology in thyroid FNA was first introduced in 2014 and then became commonly used [7]. However, liquid-based cytology has not been made widely available for thyroid FNA in other countries [5,8-11].
Core needle biopsy as an alternative to thyroid FNA has been used mainly in Korea whereas in other countries, this biopsy is performed only in a few institutions [5-10].
Immunocytochemistry generally has limited applications for the diagnosis of thyroid FNA in Asian countries. Although molecular testing has been useful for the diagnosis of indeterminate thyroid FNA, it is often not practical for most clinical laboratories and is generally not covered by health insurance in Asia [5-11].
Table 6 summarizes the ancillary tests in thyroid FNA cytology [5-11].
Ancillary tests in thyroid FNA cytology
TRAINING PROGRAM
Asian pathologists receive a certification in pathology and cytopathology after completing residency training and passing board examinations, and usually practice both surgical pathology and cytopathology. Training programs for cytotechnicians have been well organized in Japan, Korea, and Taiwan. Certified cytotechnicians screen thyroid FNA cytology, but are not eligible to declare a final diagnosis without supervision by a pathologist. Table 7 summarizes the training programs for cytopathologists and cytotechnicians [5-11].
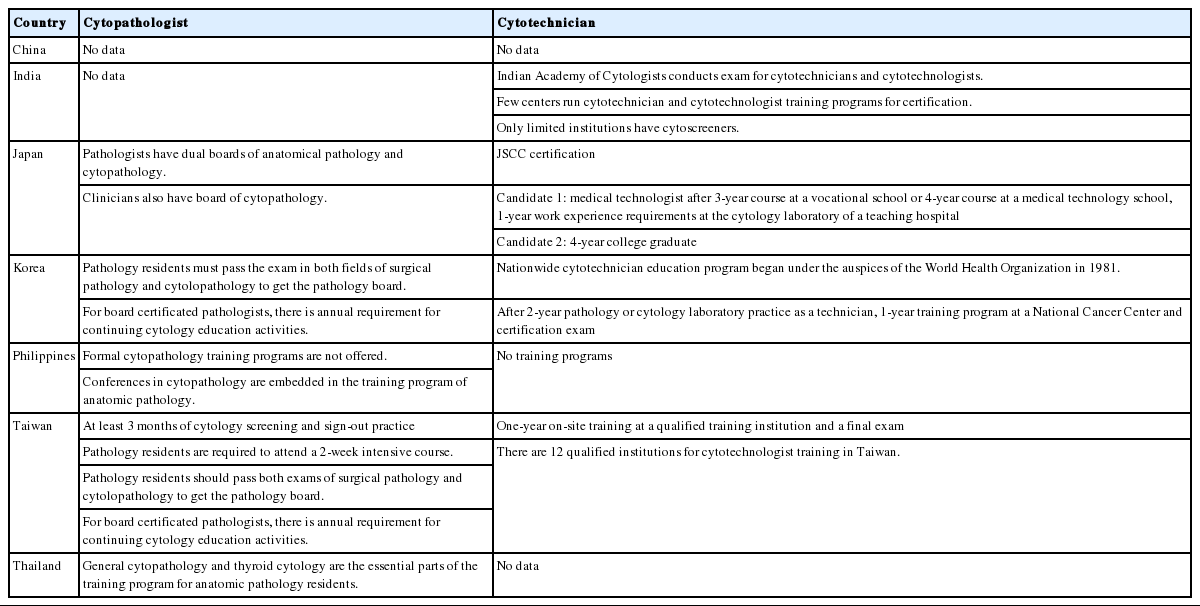
Training programs for cytopathologists and cytotechnicians
QUALITY CONTROL AND QUALITY ASSURANCE PRACTICES
Quality control in cytology includes all activities to improve the performance of the test from the time of specimen collection until the cytology report is completed. Quality assurance defined by the College of American Pathologists includes quality review activities and systematic monitoring of quality control results to provide confidence that all quality control systems are functioning properly and quality requirements are fulfilled [19]. Quality control materials in thyroid FNA should include the distribution of each diagnostic category, histologic outcomes of FNA diagnostic categories, rate of surgical follow-up, and risk of malignancy calculated using the total number of each diagnostic category with and without surgical follow-up.
Quality improvement programs in Asian countries are organized by local societies of cytology and/or pathology. Table 8 summarizes the quality assurance and quality control programs in thyroid FNA cytology [5-11].
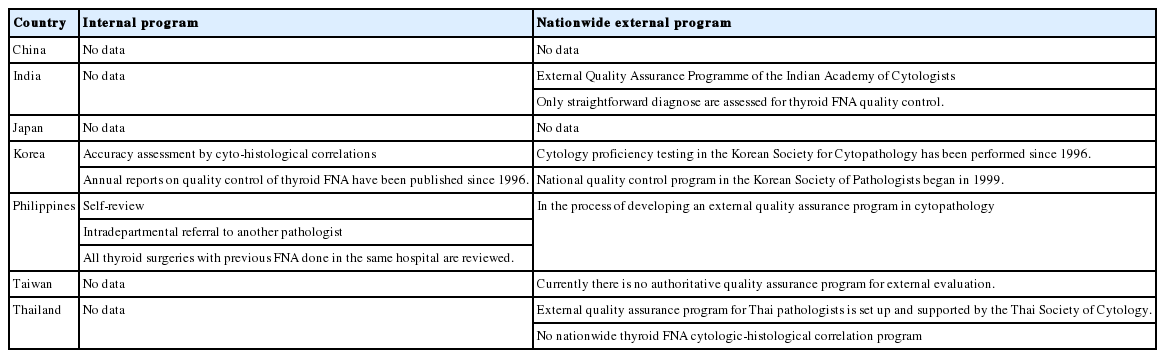
Quality assurance and quality control programs in thyroid FNA cytology
CONCLUSION
The purpose of the recently established Working Group of Asian Thyroid FNA Cytology is to promote communication and share practices among pathologists, cytopathologists, and clinicians dealing with thyroid FNA in Asia. In this special issue, we presented for the first time a single volume collection of contemporary reviews on Asian practices of thyroid FNA. Despite most countries adopting Western systems and guidelines and incorporated them into their national systems early, there remains local variation which should be considered when doing comparisons between Asian and Western countries, and among Asian countries. We hope that these reports from Asia will encourage further studies on thyroid FNA cytology to improve the diagnosis of thyroid nodules and subsequently provide optimal care for patients with thyroid nodules in Asia.
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
We would like to acknowledge all the members of the Working Group of Asian Thyroid FNA Cytology. This work was supported by a grant (HI16C2013) from the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea.