Increased Toll-like receptor 9 expression associated with cellular proliferation and poor prognosis in pleural mesothelioma
Article information

Abstract
Background
Pleural mesothelioma is an aggressive malignancy with a poor prognosis. The epithelioid subtype is the most common and can be challenging to distinguish from metastatic lung adenocarcinoma (MLAC). The role of Toll-like receptor 9 (TLR9) in the progression of pleural mesothelioma remains unclear.
Methods
A total of 30 pleural biopsy specimens were collected, comprising 10 cases of pleural epithelioid mesothelioma and 20 cases of MLAC. The mRNA expression levels of TLR9 and proliferating cell nuclear antigen (PCNA) were quantified. In addition, sixty archived formalin-fixed, paraffin-embedded tissue blocks (40 epithelioid mesothelioma and 20 MLAC) were analyzed via immunohistochemistry using an anti-TLR9 antibody in relation to various clinicopathological parameters.
Results
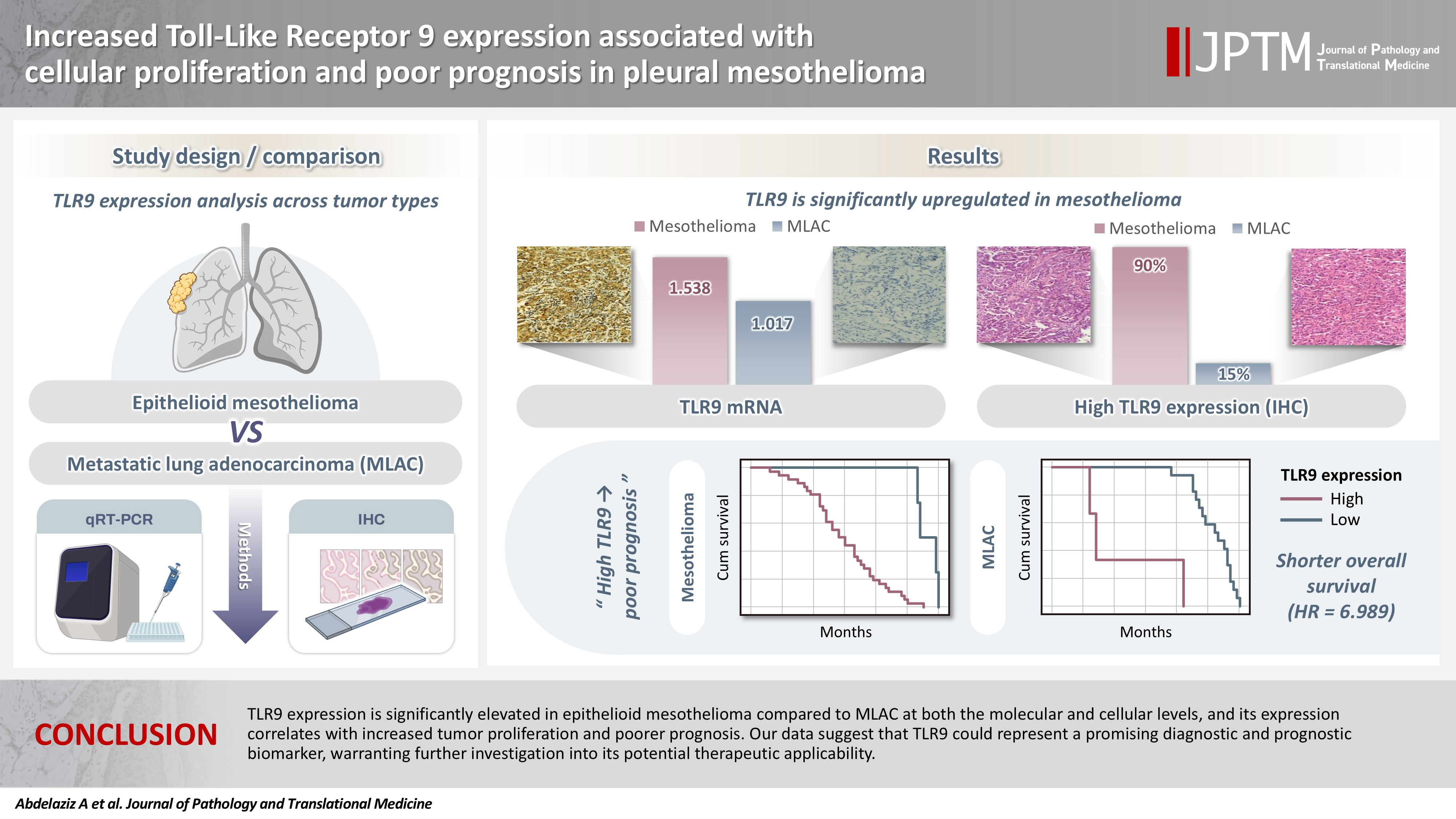
TLR9 expression was significantly higher in epithelioid mesothelioma cases than in MLAC cases (p < .001), with mean values of 1.54 ± 0.09 and 1.02 ± 0.08, respectively. A significant positive correlation was observed between TLR9 and PCNA expression levels specifically in the epithelioid mesothelioma cohort (p < .001, r = 0.8). Furthermore, immunohistochemical analysis confirmed that high TLR9 immunoexpression was significantly more prevalent in epithelioid mesothelioma (36/40 cases; 90%) than in MLAC (3/20 cases; 15%) (p < .001). Notably, elevated TLR9 expression was associated with a significantly shorter overall survival (p = .001).
Conclusions
In conclusion, TLR9 expression is significantly elevated in epithelioid mesothelioma compared to MLAC at both the molecular and cellular levels, and its expression correlates with increased tumor proliferation and poorer prognosis. Our data suggest that TLR9 could represent a promising diagnostic and prognostic biomarker, warranting further investigation into its potential therapeutic applicability.
INTRODUCTION
Pleural mesothelioma is a rare and aggressive malignancy with a poor prognosis, typically characterized by an average overall survival (OS) of 9 to 18 months [1]. The epithelioid subtype is the most prevalent and is often challenging to distinguish from metastatic lung adenocarcinoma (MLAC). The diagnostic confirmation of epithelioid mesothelioma typically relies on immunohistochemical profiling using a combination of two positive mesothelial markers (e.g., calretinin, Wilms' tumor-1, or cytokeratin 5/6) and two negative markers (e.g., carcinoembryonic antigen, Ber-EP4, or MOC-31) to exclude carcinoma [2]. The considerable histological diversity of mesotheliomas, coupled with the pleura being a common site for metastatic disease, renders diagnosis based on morphology alone particularly challenging. Current treatment modalities are primarily limited to surgery, chemotherapy, and radiotherapy. Consequently, there is an urgent, unmet need to develop novel, effective, and tailored therapeutic strategies for pleural epithelioid mesothelioma. Although Toll-like receptor 9 (TLR9) has ushered in a new era for mesothelioma management as a form of immunotherapy, its precise role remains incompletely understood [3]. TLR9 agonists show significant potential in combination therapies, where they synergize with other agents to augment anti-tumor immune responses [4]. Despite this promise, clinical trials of these agonists have yet to meet expectations [5]. Therefore, elucidating the expression pattern of TLR9 in mesothelioma and deciphering its role in tumorigenesis—particularly in proliferation—is essential. In this study, we compare TLR9 expression in pleural epithelioid mesothelioma and MLAC and correlate this expression with patients' clinicopathological parameters.
MATERIALS AND METHODS
Sample collection
Fresh samples
Pleuroscopy was performed under local anesthesia with intravenous conscious sedation using a Karl Storz rigid thoracoscope (Tuttlingen, Germany). The entry site, typically at the 5th or 6th intercostal space, was optimized under ultrasound guidance. Approximately six biopsies were collected from visible pleural lesions. From each patient, two sample sets were obtained: one was snap-frozen at −80°C for molecular analysis, and the other was fixed in neutral buffered formalin 10% for histopathological examination.
Paraffin blocks
Sixty archival formalin-fixed paraffin-embedded (FFPE) tissue blocks were randomly selected from previously diagnosed cases at the pathology laboratories of Minia University Hospitals and Minia Oncology Centre. All specimens were obtained via thoracoscopic biopsy. The cohort consisted of 40 cases of epithelioid mesothelioma and 20 cases of MLAC.
Histopathological confirmation and immunohistochemical validation
Histopathological examination of hematoxylin and eosin–stained sections was performed to confirm the initial diagnosis and to assess key tumor characteristics, including tumor grade, the presence of tumor-infiltrating lymphocytes (TILs), and necrosis. Immunohistochemical analysis confirmed the differential expression of the studied markers, supporting the mRNA expression results.
Pathological assessment
The pathological T stage was determined for all cases according to the 8th edition of the tumor-node-metastasis (TNM) classification system [6]. Tumor grading was assessed following the 2015 World Health Organization classification of tumors of the lung and pleura [7]. The presence or absence of tumor necrosis and significant TILs was systematically recorded.
Clinicopathological data collection
Relevant clinicopathological data were extracted through a comprehensive review of medical records. Systematically collected demographic data included patient age at diagnosis and sex. Age groups were subsequently categorized based on the median age of the enrolled cases. The clinicopathological data of the patients are summarized in Table 1.
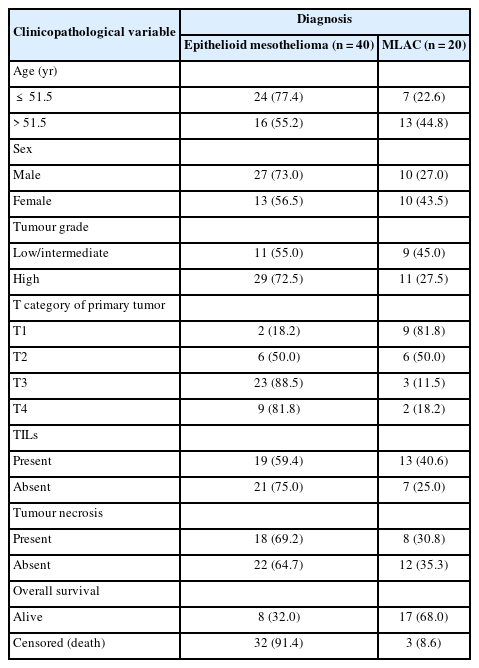
The clinicopathological data of epithelioid mesothelioma and MLAC patients (n=60)
Quantitative real-time polymerase chain reaction
The relative expression levels of TLR9 and proliferating cell nuclear antigen (PCNA) mRNA were quantified using quantitative reverse transcription polymerase chain reaction (qRT-PCR). Total RNA was extracted from pleural tissue samples using Ribozol solution (AMSBIO, Cambridge, UK). RNA concentration and purity were assessed spectrophotometrically (NanoDrop 2000, Thermo Fisher Scientific, Waltham, MA, USA); samples with a 260/280 ratio greater than 2.0 and a 260/230 ratio greater than 1.8 were considered intact and used for subsequent analysis. cDNA was synthesized from the extracted RNA, and real-time polymerase chain reaction (PCR) was subsequently performed using a commercial SYBR Green PCR kit (Qiagen, Hilden, Germany). The SYBR Green PCR kit included the provided Universal PCR Master Mix. The thermal protocol was run on DTlite Real-Time PCR System (DNA Technology, Moscow, Russia), and performed as follows: 45°C for 10 minutes, 95°C for 2 minutes, followed by 40 cycles at 95°C for 5 seconds, 60°C for 10 seconds, and 72°C for 5 seconds. Fluorescence was measured during the 72°C step for each cycle. The relative quantitation of both TLR9 and PCNA expression to glyceraldehyde 3-phosphate dehydrogenase (reference gene) were calculated using cycle threshold (Ct) method. Ct was calculated by DT master software: ΔCt = Ct (target gene) – Ct (reference gene). The ΔΔCt values were calculated through the following equation = Mean ΔCt(epithelioid mesothelioma) − Mean ΔCt (MLAC).
The TLR9 real-time PCR forward primer was TTCCCTGTAGCTGCTGTCC, reverse primer was ACAGCCAGTTGCAGTTCACC.
The PCNA real-time PCR forward primer was CCATCCTCAAGAAGGTGTTGG, reverse primer was GTGTCCCATATCCGCAATTTAT.
Immunohistochemistry
Four-micrometer tissue sections were cut from the FFPE blocks and mounted on positively charged slides. Immunohistochemistry (IHC) was performed on an automated immunostainer (Ventana BenchMark GX, Ventana Medical Systems, Inc., Tucson, AZ, USA) according to the manufacturer's protocol. Antigen retrieval was conducted using a Tris-based buffer (pH 7.6). Sections were incubated with a mouse anti-human monoclonal anti-TLR9 antibody [clone 26C593.2] (dilution 1:100, catalog number ab134368, Abcam, Cambridge, UK). Appropriate positive and negative controls were included in each run to ensure staining specificity and accuracy.
Evaluation of immunohistochemical staining
Immunohistochemical evaluation was performed independently by two pathologists (D.M.T. and M.F.G.). Staining was assessed based on the intensity and localization according to the method described by Gao et al. [8]. A semi-quantitative scoring system was employed, evaluating both the proportion and the staining intensity of immunoreactive cells. The proportion of stained tumor cells was scored as follows: 0 (negative), 1 (<10% stained tumor cells), 2 (10%–50% stained tumor cells), and 3 (>50% stained tumor cells). The staining intensity was scored on a scale of 0 (no staining), 1 (weak cytoplasmic staining, light yellow), 2 (moderate cytoplasmic staining, yellowish brown), and 3 (strong cytoplasmic staining, brown). A final staining index was calculated for each case using the formula: Staining index = (Intensity score) + (Proportion score).
Based on this index, cases were categorized as follows: A staining index of ≥4 indicated high TLR9 expression, whereas a staining index of <4 indicated low TLR9 expression [8].
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences ver. 20.0 (IBM Corp., Armonk, NY, USA). The association between TLR9 expression and clinicopathological parameters was evaluated using the chi-square test or Fisher’s exact test, as appropriate. Survival curves were generated using the Kaplan-Meier method, and differences were compared with the log-rank test. The prognostic impact of TLR9 expression was further assessed using univariate and multivariate Cox regression. Results are presented as hazard ratio (HR) with corresponding 95% confidence interval (CI). A p-value < .05 was deemed statistically significant.
RESULTS
Expression values of TLR9 mRNA in pleural epithelioid mesothelioma versus MLAC
qRT-PCR analysis revealed a significantly higher mRNA expression level of TLR9 in epithelioid mesothelioma cases (1.54 ± 0.09) compared to MLAC cases (1.02 ± 0.08) (p < .001) (Supplementary Fig. S1). PCNA mRNA levels were elevated in both groups. The ΔΔCt values were 0.63 for TLR9 and 0.08 for PCNA. Notably, a strong and significant positive correlation between TLR9 and PCNA expression was identified specifically within the epithelioid mesothelioma cohort (p < .001, r = 0.8) (Supplementary Fig. S2).
Immunohistochemical expression of TLR9 in pleural epithelioid mesothelioma and MLAC
Immunohistochemical analysis revealed high TLR9 expression, localized to the cytoplasm of malignant cells, in 36 of 40 (90%) epithelioid mesothelioma cases compared to only three of 20 (15%) MLAC cases (Fig. 1). In epithelioid mesothelioma, high TLR9 expression showed a significant association with advanced T category of the primary tumor (p = .045) (Fig. 2). Conversely, a significant inverse relationship was observed between TLR9 expression and T category of the primary tumor in MLAC (p = .014). No other significant associations were found between TLR9 expression and the remaining clinicopathological parameters. A detailed summary of these associations is provided in Table 2.
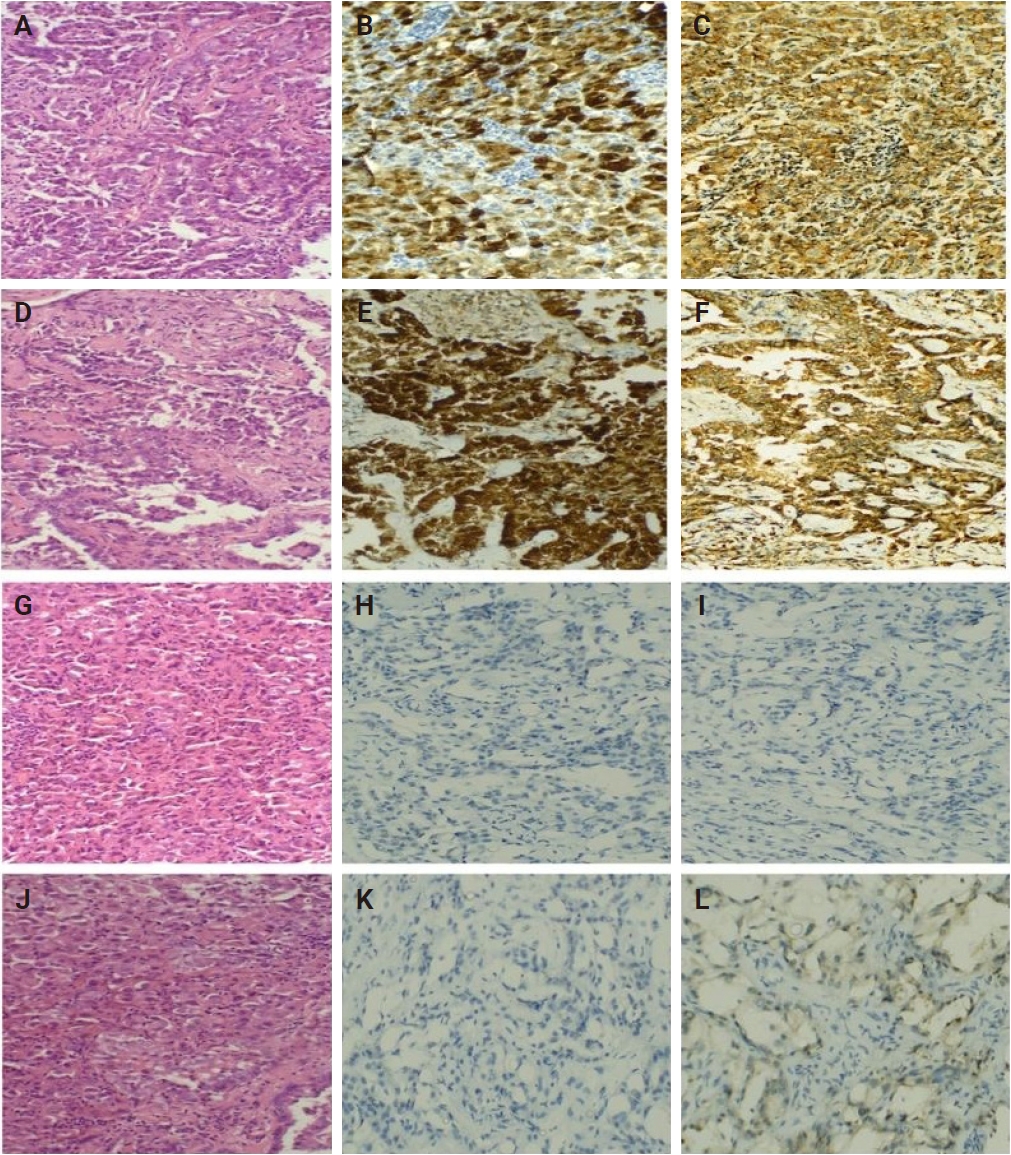
(A–F) Mesothelioma: H&E staining of epithelioid mesothelioma, positive calretinin expression and high Toll-like receptor 9 (TLR9) expression, respectively. (G–L) Metastatic adenocarcinoma: H&E staining of metastatic lung adenocarcinoma, negative calretinin expression and negative/low TLR9 expression, respectively. (A, D, G, J) H&E. (B, E, H, K) Calretinin. (C, F, I, L) TLR9.
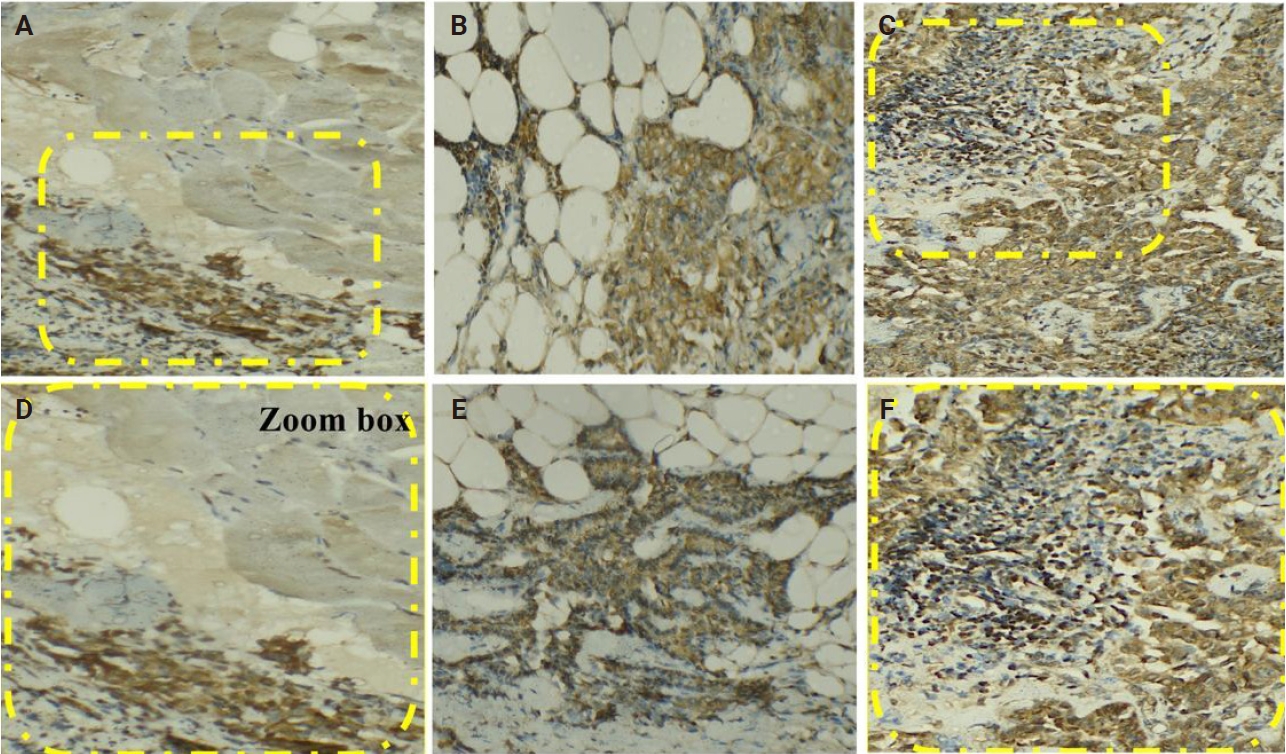
Expression of Toll-like receptor 9 (TLR9) in epithelioid mesothelioma cases with tumor invasion and inflammation. High TLR9 expression in mesothelioma with muscle invasion (A, D), fat invasion (B, E), and in mesothelioma and inflammatory cells (C, F). (A) Positive TLR9 expression in mesothelioma cells invading the surrounding muscle. (B) Positive TLR9 expression in mesothelioma cells invading the surrounding fat. (C) High TLR9 expression in inflammatory cells and mesothelioma cells. (D) Yellow zoom box showing the high expression of TLR9. (E) Another case showing positive TLR9 expression in mesothelioma cells invading the surrounding fat. (F) Yellow zoom box showing the high expression of TLR9 in inflammatory cells and mesothelioma cells.
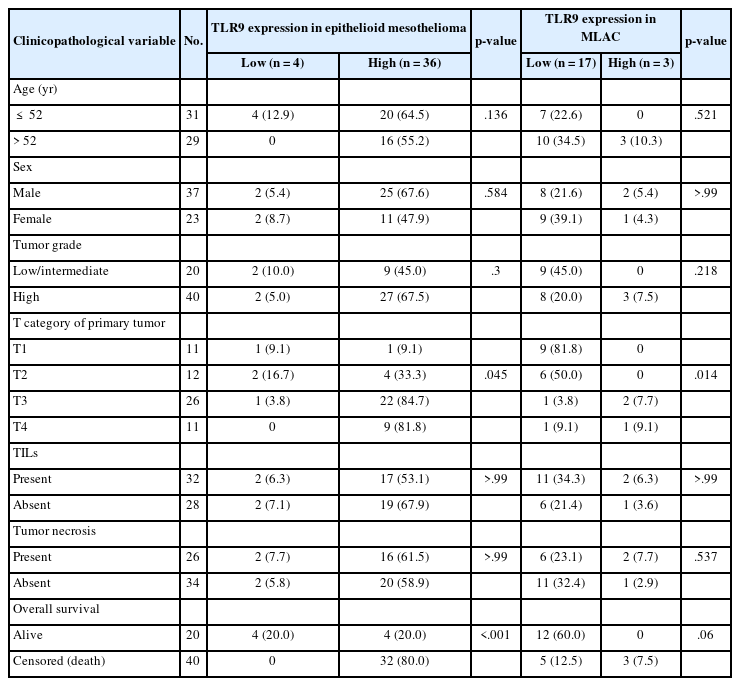
Immunohistochemical expression of TLR9 and its association with clinicopathological data
Survival analysis and prognostic significance
The OS follow-up period for all 60 cases of pleural malignancy ranged from 6 to 60 months. The mean OS was 37.48 ± 1.53 months, and the median survival time was 38 months. In epithelioid mesothelioma, high TLR9 expression was significantly associated with shortened OS (Fig. 3). Notably, 88.8% of mesothelioma patients with high TLR9 expression had died at the end of the follow-up period (log-rank test, p = .001). In contrast, no significant association was observed between TLR9 expression and OS in the MLAC cohort (Table 2).
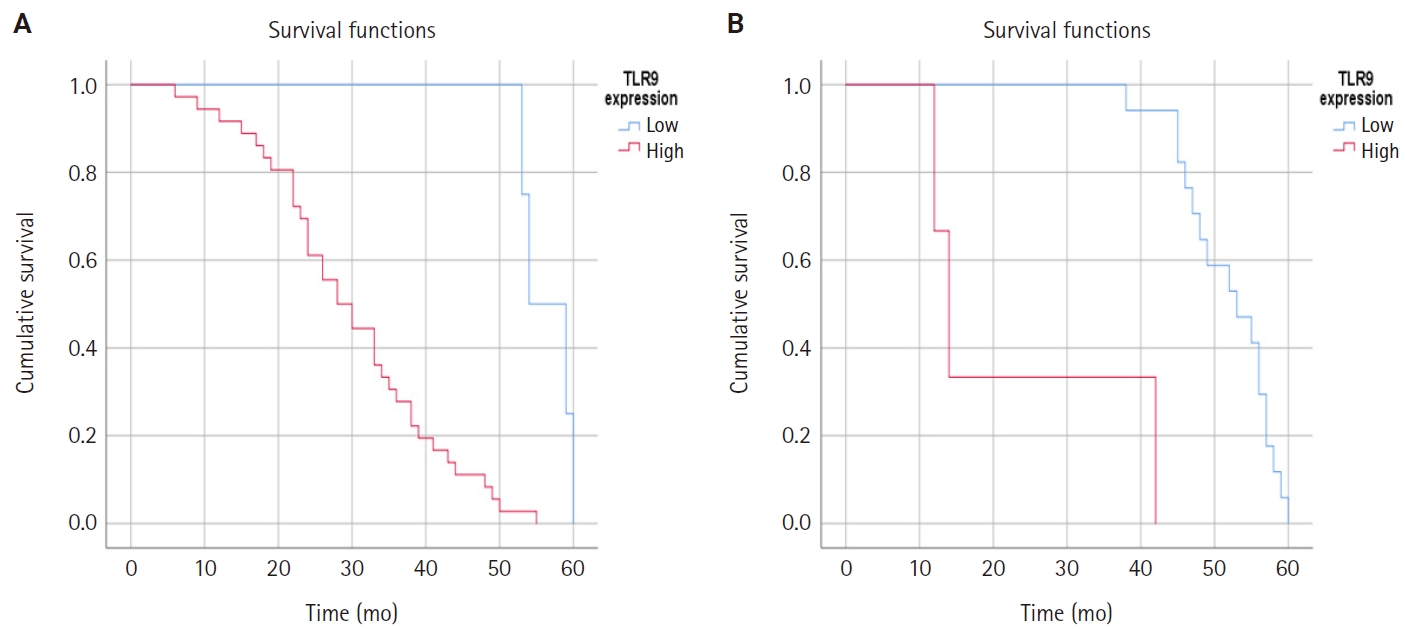
The relationship between Toll-like receptor 9 (TLR9) expression and overall survival in mesothelioma (A) and metastatic lung adenocarcinoma (MLAC) (B). Kaplan-Meier curves showing that high TLR9 expression is associated with shorter overall survival in patient with pleural epithelioid mesothelioma and not in MLAC.
Univariate and multivariable Cox regression analysis
Next, we considered clinicopathological variables (age, sex, tumor grade, tumor stage, inflammation, and tumor necrosis) in univariate Cox regression models for OS. Subsequently, a multivariable Cox regression model was constructed incorporating these variables along with TLR9 expression status. Although based on a relatively small cohort, the analysis suggested that high TLR9 expression may be independently associated with poorer prognosis in mesothelioma cases (HR, 6.989; 95% CI, 2.148 to 22.738). Given the sample size, these findings should be interpreted as exploratory and warrant further validation in larger cohorts (Table 3).
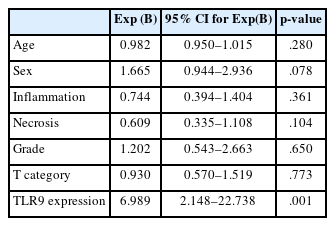
Multivariate survival analysis in pleural malignancy cases
DISCUSSION
Previous studies reported that TLR3, TLR7, and TLR9 could be targetable therapy in mesothelioma [9,10]. Furthermore, the well-known TLR9 agonist, cytosine-phosphoguanine oligodeoxynucleotides induced antitumor activity against peritoneal mesothelioma in an animal model [3], but still the role of TLR9 in pleural mesothelioma is undermined.
In this study, a significantly high TLR9 expression was detected in epithelioid mesothelioma by using PCR and IHC, suggesting a potential diagnostic value. Additionally, the positive correlation found between TLR9 and PCNA mRNA expression in epithelioid mesothelioma (p < .001, r = 0.8) suggesting a possible involvement of TLR9 in tumor proliferation. Aligned with our study, high TLR9 mRNA value was previously reported by various studies to be linked with tumor proliferation in several cancers [11,12].
To note, this study represents the first investigation of the immunohistochemical expression of TLR9 in pleural mesothelioma and suggests that TLR9 may play a role in mesothelioma tumorigenesis. Stimulation of TLR9 and high TLR9 expression were linked to tumor hallmarks in several cancers, including lung cancer [13,14], prostate cancer [15], hepatocellular carcinoma [16], and breast cancer [17]. Furthermore, previous studies underscored the role of TLR9 in tumorigenesis and cancer cell survival, through its effects on the activation of anti-apoptotic molecules such as Bcl2 and XIAP [18].
In contrast to our results, Droemann et al. [19] and Zhang et al. [14] found that TLR9 expression was significantly high in lung adenocarcinoma cases [18]. However, the mentioned expression in their studies was observed in primary lung tumors, and no data were provided regarding its expression in metastatic pleural deposits of lung adenocarcinoma, as is the case with our findings. The discrepancy in receptors expression between primary tumors and metastases was reported in previous studies. For instance, a study on breast cancer revealed that the estrogen receptor was highly expressed in primary tumors whereas weak expression was observed in metastases [20]. Another study showed that connexin 26 and 43 decreased in primary tumors compared to metastatic tumors [21]. This heterogeneity of receptors expression is a well-known phenomenon in cancer biology [19]. While primary tumors may benefit from high TLR9 expression, metastatic cells might downregulate TLR9 to evade immune detection in new sites, which could explain the reduction of TLR9 in MLAC that was detected in our study.
Interestingly, a significant positive association was detected between TLR9 expression and T category of tumor in mesothelioma, whereas an inverse relationship was observed in MLAC cases. This suggests that high TLR9 expression may be associated with tumor progression and spread in mesothelioma but its role in MLAC spread cannot be determined due to the lack of primary tumor expression values. Moreover, TLR9 receptor itself may elicit different functions depending on the tumor context. For instance, Gonzalez-Reyes et al. [15] observed that increased TLR9 expression correlated with greater aggressiveness in breast cancer, while in other studies elevated TLR9 was linked to advanced stages.
In contrast, Singh et al. [22] reported that high TLR9 expression following chemotherapy showed evidence of antitumor activity. These discrepancies in TLR9 expression suggest that TLR9 expression may be changed with different tumor status, treatment context, or experimental design. It is also worth noting that in our study, TLR9 expression in MLAC was evaluated only in metastatic deposits, and not in primary tumors, which may explain the lack of correlation with metastasis.
Survival analysis reported that high TLR9 expression in epithelioid mesothelioma was significantly associated with shorter OS (p = .001). TLR9 was suggested to be an independent prognostic factor by using multivariate Cox regression analysis (HR, 6.989; 95% CI, 2.148 to 22.738). This finding is comparable with other studies that revealed elevated TLR9 levels correlate with poor prognosis [23]. Conversely, no significant association between TLR9 expression and OS was observed in MLAC cases.
Interestingly, high TLR9 expression was detected in inflammatory cells in few cases of epithelioid mesothelioma (10%) and the tumor cells in these cases also revealed high TLR9 expression (Fig. 2). This suggests that TLR9 may have an additional action depending on its site, whether in tumor cells or in inflammatory cells [24].
Limitations of the study
First, the sample size, while sufficient for initial comparisons, is relatively small for robust survival and subgroup analyses. This limited statistical power likely explains why established prognostic factors like tumor stage did not reach significance in our multivariate model and precluded more sophisticated analyses to draw more definite conclusions. Therefore, our primary finding—that TLR9 expression is significantly higher in mesothelioma compared to MLAC—requires validation in a larger, independent cohort. Second, all cases were collected from a single institution; future multi-center studies would enhance the generalizability of the results. Third, we were unable to perform Western blot analysis on the exact same fresh-frozen samples used for qRT-PCR due to insufficient tissue material; however, our immunohistochemical findings on a larger, independent cohort provide strong complementary validation at the protein level. Finally, this study did not explore the mechanistic role of TLR9 in mesothelioma pathogenesis, which remains a crucial area for future investigation.
Conclusions
To conclude, this study underscores the role of TLR9 in epithelioid mesothelioma. TLR9 shows potential as a complementary diagnostic marker to differentiate epithelioid mesothelioma from MLAC and a potentially prognostic biomarker due to its association with poor prognostic parameters in epithelioid mesothelioma. Furthermore, this study suggests that targeting TLR9 could be a potential therapeutic strategy.
Supplementary Information
The Data Supplement is available with this article at https://doi.org/10.4132/jptm.2026.04.01.
Notes
Ethics Statement
The study performed was approved by the Research Ethics Committee of the Faculty of Medicine at Minia University (approval No. 334-6-2022). Informed consent was obtained from all individual participants included in the study.
Availability of Data and Material
All data generated or analyzed during the study are included in this published article (and its supplementary information files).
Code Availability
Not applicable.
Author Contributions
Conceptualization: AOA, FEZAM. Data curation: AOM, MFG. Formal analysis: MFG. Funding acquisition: AOA, DMT, RMK, HM, RFA, MFG, FEZAM. Investigations: RFA, HM, MFG. Methodology: DMT, HM, RFA. Project administration: all authors. Resources: AOA, DMT, MFG. Supervision: MFG, FEZAM. Validation: HM, RFA, FEZAM. Visualization: HM, RFA, FEZAM. Writing—original draft: DMT, RMK, HM, RFA, FEZAM. Writing —review & editing: DMT, RMK, HM, RFA, FEZAM. Approval of final manuscript: all authors.
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
Funding Statement
This study is partially supported by the Alexander Von Humboldt Foundation (Germany). The fund was provided as a return fellowship grant. The rest of the study fund is provided from the authors themselves.