 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(4); 2013 > Article
-
Brief Case Report
Pleomorphic Adenoma of the Trachea: A Case Report - Ki-Sung Park, Woo Jung Sung1
-
Korean Journal of Pathology 2013;47(4):399-401.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.4.399
Published online: August 26, 2013
Department of Thoracic and Cardiovascular Surgery, Catholic University of Daegu, School of Medicine, Daegu, Korea.
1Department of Pathology, Catholic University of Daegu, School of Medicine, Daegu, Korea.
- Corresponding Author: Woo Jung Sung. Department of Pathology, Catholic University of Daegu, School of Medicine, 33 Duryugongwon-ro 17-gil, Nam-gu, Deagu 705-718, Korea. Tel: +82-53-650-4159, Fax: +82-53-650-3050, 'wjsung@cu.ac.kr'
• Received: September 10, 2012 • Revised: December 12, 2012 • Accepted: December 13, 2012
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
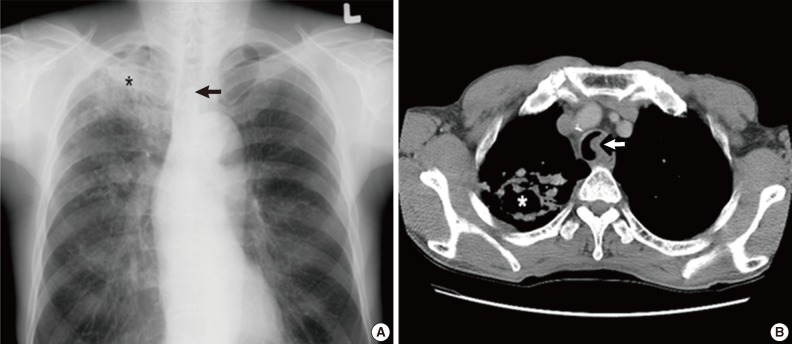
- A 59-year-old male was referred to our hospital due to a three-month history of dyspnea on exertion. He was a current smoker with a 45-year history of smoking 2 packs of cigarettes per day. He had no past medical history except for pulmonary tuberculosis two years prior. On physical examination, the sound of his right lung was decreased with crackles but he did not have lymphadenopathy or weight loss. Laboratory findings were unremarkable except that the pulmonary function test revealed a moderately obstructive lung defect. Chest X-ray showed reactivation of pulmonary tuberculosis in the upper lung field and a round mass shadow in the mid-tracheal area (Fig. 1A). A computed tomography (CT) scan showed a 2.2 cm-sized homogenous mass originating from the left lateral inner wall of the trachea, and active pulmonary tuberculosis with cavitation in the right upper lobe and in the superior segment of the right lower lobe (Fig. 1B). Flexible bronchoscopy revealed a broad-based, polypoid mass obstructing 75% of the lumen in the left lateral wall. The mass was 5 cm above the carina, without endobronchial lesion (Fig. 2A). We decided to surgically remove the lesion after initial management for pulmonary tuberculosis since airway obstrucion could occur during the bronchoscopic procedure owing to rich vascularity on the tumor surface.
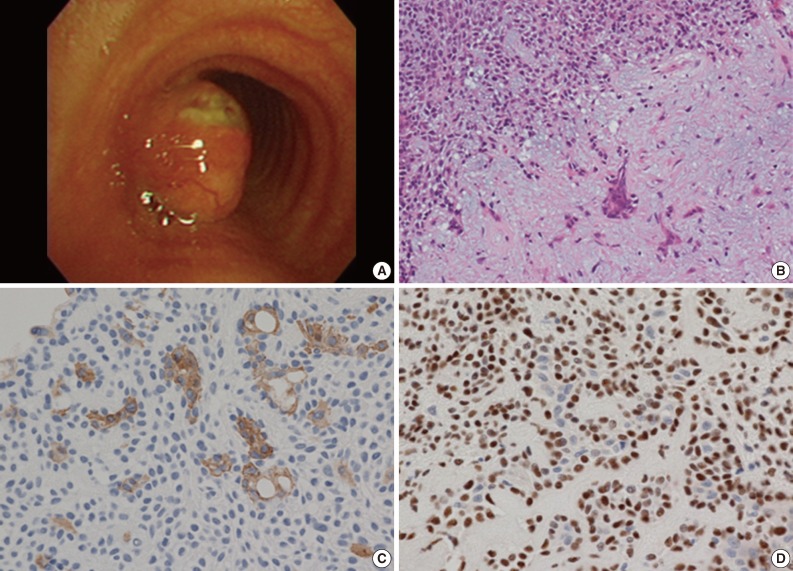
- The patient underwent right thoracotomy with segmental resection and end-to-end anastomosis. Four tracheal rings were excised along with the tumor. The excised tumor appeared as a single well-demarcated solid, polypoid mass, measuring 2×2 cm in size. The mass was completely covered by intact mucosa without any visible sign of hemorrhage or necrosis. On microscopic examination, the mass was composed of epithelial and myoepithelial cells in the chondromyxoid stroma (Fig. 2B). There was no definitive cellular pleomorphism and mitotic figures. The surgical margins of the resected trachea were free of tumor. Immunohistochemically, the epithelial cells were positive for cytokeratin, cytokeratin 19 and epithelial membrane antigen (EMA). The myoepithelial cells were immunoreactive for cytokeratin, S100 protein, and p63 (Fig. 2C, D). Overall, these findings were suggestive of a pleomorphic adenoma involving the mid trachea. The postoperative course was uneventful, and the patient has been asymptomatic and in good health for 5 years after the surgery.
CASE REPORT
- Pleomorphic adenoma is the most common tumor of the major salivary gland, rarely occurring in the lung and typically arising from the tracheal and bronchial seromucous glands.2,3 The exact definitive incidence has not been reported. The age range of patients diagnosed with pleomorphic adenoma is usually between 35 and 74 years, with no gender or age predominance,1,2 although a case has been reponted in an 8-year-old male.4 Almost half of these tumors were localized in the upper one-third of the trachea and 12% were localized in the lower one-third.5 The tumor in the present case arose from the left lateral inner wall of the lumen which was 5 cm above the carina in the mid-tracheal area. The most common symptoms are cough, sputum, dyspnea, wheeze, and stridor.1,4 Normally, because of the slow tumor growth, these respiratory signs and symptoms are misdiagnosed as asthma,5 and thus proper diagnosis may be delayed. The tumor may not be discovered on plain chest posterior-anterior view and therefore, chest CT and bronchoscopy are important in diagnosing the patient at presentation.
- The histological characteristics are similar to salivary gland tumors. Microscopic findings show trabecular or islands of epithelial and myoepithelial cells in a myxoid or chondroid matrix.1 Immumohistochemical staining is helpful to diagnose pleomorphic adenoma, in which the findings are positive for the myoepithelial cell components for cytokeratin, p63 and S100 protein.5 In addition, ductal epithelial cell components are positive for cytokeratin, EMA, secretory component carcinoembryonic antigen, lysozyme, and gross cystic disease fluid protein-15. The most frequently expressed cytokeratin 19 is positive in the luminal cells of the tubular structures.6
- The most difficult differential diagnosis of pleomorphic adenoma is adenoid cystic carcinoma. Tumor cell nests of adenoid cystic carcinoma are sharply separated from the stroma.7 Adenoid cystic carcinoma is an aggressive malignant tumor, therefore invasive focus, especially perineural invasion, is usually identified.
- Assessing the prognosis such as biological behavior and clinical course is difficult. Histological findings associated with aggressive behavior, such as recurrence and metastasis, include infiltrative and poorly circumscribed tumor margin and high mitotic counts.1,8
- There have been two reports of malignant and aggressive tumors.9,10 Thus, tumors should be considered to have malignant potential and a careful follow-up is mandatory after complete resection, as in our patient's case who is healthy 5 years postoperatively. Because the tumor rarely occurs, standard management has not been established. In general, endoscopic resection or surgical segmental resection is selected as a treatment on the basis of tumor status and physician's preference.2,5 Endoscopic removal may be used when rapid respiratory symptom improvement or hemorrhage control is required. Segmental resection is the only curative treatment for complete excision of both types of benign and malignant tumors, and decreases the possibility of lesion recurrence.
- In conclusion, pleomorphic adenoma of the trachea should be included in the differential diagnosis of tracheal tumors, although the occurrence is very rare. Surgical excision is the optimal therapy for a low possibility of recurrence of pleomorphic adenoma. Future studies with additional cases are needed in order to define the clinical course, biologic behavior and prognosis of pleomorphic adenoma of the trachea.
DISCUSSION
- 1. Moran CA, Suster S, Askin FB, Koss MN. Benign and malignant salivary gland-type mixed tumors of the lung: clinicopathologic and immunohistochemical study of eight cases. Cancer 1994; 73: 2481–2490. PMID: 7513602. ArticlePubMed
- 2. Goto T, Maeshima A, Akanabe K, et al. Bronchial pleomorphic adenoma coexisting with lung cancer. Ann Thorac Cardiovasc Surg 2011; 17: 174–177. PMID: 21597416. ArticlePubMed
- 3. Paik SS, Jin YH, Park CK, Shin DH, Chung WS, Lee JD. Pleomorphic adenoma of the trachea. J Korean Med Sci 1997; 12: 564–566. PMID: 9443098. ArticlePubMedPMC
- 4. Baghai-Wadji M, Sianati M, Nikpour H, Koochekpour S. Pleomorphic adenoma of the trachea in an 8-year-old boy: a case report. J Pediatr Surg 2006; 41: e23–e26. PMID: 16863832. Article
- 5. Aribas OK, Kanat F, Avunduk MC. Pleomorphic adenoma of the trachea mimicking bronchial asthma: report of a case. Surg Today 2007; 37: 493–495. PMID: 17522768. ArticlePubMed
- 6. Ogawa Y, Toyosawa S, Ishida T, Ijuhin N. Keratin 14 immunoreactive cells in pleomorphic adenomas and adenoid cystic carcinomas of salivary glands. Virchows Arch 2000; 437: 58–68. PMID: 10963381. ArticlePubMed
- 7. Sano T, Hirose T, Hizawa K, et al. A case of pleomorphic adenoma of the trachea. Jpn J Clin Oncol 1984; 14: 93–98. PMID: 6323791. PubMed
- 8. Payne WS, Schier J, Woolner LB. Mixed tumors of the bronchus (salivary gland type). J Thorac Cardiovasc Surg 1965; 49: 663–668. PMID: 14274349. ArticlePubMed
- 9. Hemmi A, Hiraoka H, Mori Y, et al. Malignant pleomorphic adenoma (malignant mixed tumor) of the trachea: report of a case. Acta Pathol Jpn 1988; 38: 1215–1226. PMID: 2853932. ArticlePubMed
- 10. Demirağ F, Topcu S, Kurul C, Memiş L, Altinok T. Malignant pleomorphic adenoma (malignant mixed tumor) of the trachea: a case report and review of the literature. Eur Arch Otorhinolaryngol 2003; 260: 96–99. PMID: 12582787. ArticlePubMedPDF
References
Fig. 1(A) Chest X-ray reveals a round mass shadow in the mid tracheal level (arrow) and tuberculosis (asterisk). (B) Computed tomographic scan of the chest shows a 2 cm-sized homogenous mass in the left lateral inner wall of the trachea (arrow) and tuberculosis with cavitation (asterisk).
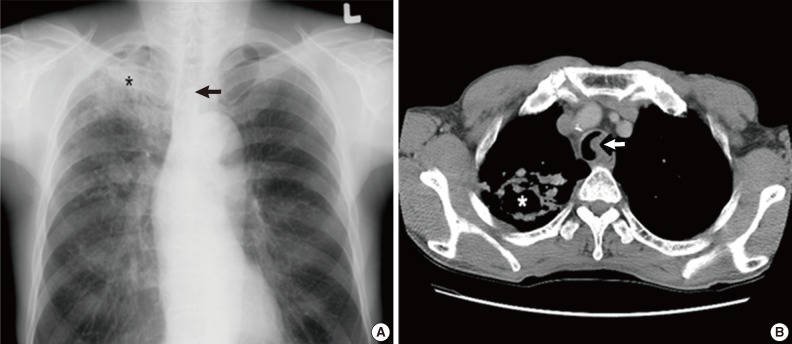
Fig. 2(A) Bronchoscopic finding of a broad and polypoid mass with branching blood vessels on the tumor surface with ulcer formation. (B) The tumor shows admixed epithelial component (left upper) and chodromixoidstroma (right lower) on microscopic examination. (C) The epithelial cell components are positive for cytokeratin 19. (D) The myoepithelial cell components show immunoreactivity for p63.
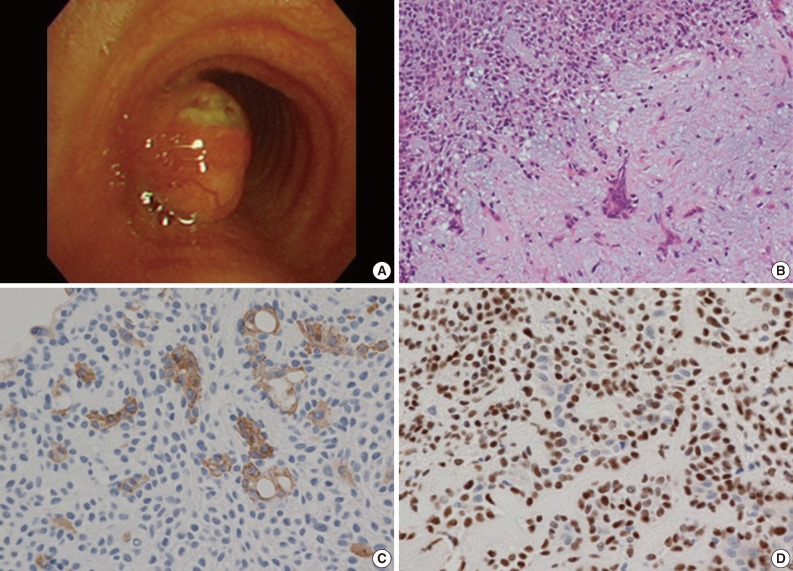
Figure & Data
References
Citations
Citations to this article as recorded by 
- Pleomorphic adenoma of the trachea: A case report
Mayu Inomata, Shoei Kuroki, Nobuyuki Oguri, Yuichiro Sato, Fumiya Kawano, Ryo Maeda
International Journal of Surgery Case Reports.2023; 109: 108499. CrossRef - Corrélation clinique, endoscopique, histologique et radiologique des tumeurs et pseudo-tumeurs de la trachée
Y. El Hassani, L. Belliraj, A. Miry, M. Haloua, N. Hammas, Y. Ouadnouni, M.Y. Alaoui Lamrani, M. Boubbou, H. El Fatemi, M. Serraj, M. Smahi, B. Amara, M. Maaroufi, B. Alami
Journal d'imagerie diagnostique et interventionnelle.2021; 4(5): 317. CrossRef - Pleomorphic Adenoma of the Trachea
Abel P. David, Stephen R. Bakos, James J. Daniero
Ear, Nose & Throat Journal.2020; 99(4): 235. CrossRef - A case report of bronchial pleomorphic adenoma in a child in China
Haiqin Zhong, Silei Yan, Kung Jiang, Yijing Hu, Xiaoyan Dong
BMC Pulmonary Medicine.2020;[Epub] CrossRef - Pleomorphic adenoma of the trachea: A case report and review of the literature
Qian-Nuan Liao, Ze-Kui Fang, Shu-Bing Chen, Hui-Zhen Fan, Li-Chang Chen, Xi-Ping Wu, Xi He, Hua-Peng Yu
World Journal of Clinical Cases.2020; 8(23): 6021. CrossRef - Pleomorphic adenoma of the trachea: A case report and review of the literature
Qian-Nuan Liao, Ze-Kui Fang, Shu-Bing Chen, Hui-Zhen Fan, Li-Chang Chen, Xi-Ping Wu, Xi He, Hua-Peng Yu
World Journal of Clinical Cases.2020; 8(23): 6026. CrossRef - Obstructive tracheal neoplasm
Badreeddine Alami, Saïd Boujraf, Mohamed Smahi, Mounia Serraj, Moulay Youssef Alaoui Lamrani, Meryem Boubbou, Mustapha Maaroufi
Formosan Journal of Surgery.2019; 52(3): 92. CrossRef - Tracheal pleomorphic adenoma with coexisting pulmonary tuberculoma
Jehun Kim, Chul-Ho Oak, Tae-Won Jang, Mann-Hong Jung
Yeungnam University Journal of Medicine.2018; 35(1): 114. CrossRef - Right main bronchial pleomorphic adenoma
Zhixing Zhu, Xihua Lian, Dongyong Yang
Medicine.2018; 97(42): e12648. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
- Related articles

