Current Issues and Clinical Evidence in Tumor-Infiltrating Lymphocytes in Breast Cancer
Article information
Abstract
With the advance in personalized therapeutic strategies in patients with breast cancer, there is an increasing need for biomarker-guided therapy. Although the immunogenicity of breast cancer has not been strongly considered in research or practice, tumor-infiltrating lymphocytes (TILs) are emerging as biomarkers mediating tumor response to treatments. Earlier studies have provided evidence that the level of TILs has prognostic value and the potential for predictive value, particularly in triple-negative and human epidermal growth factor receptor 2–positive breast cancer. Moreover, the level of TILs has been associated with treatment outcome in patients undergoing neoadjuvant chemotherapy. To date, no standardized methodology for measuring TILs has been established. In this article, we review current issues and clinical evidence for the use of TILs in breast cancer.
Molecular medicine has shown that all cancers are caused by mutations accumulated in various genes. Cancerous tissues harboring genetic mutations frequently create a new class of tumor-specific antigens [1,2]. The presentation of neoantigen by tumor cells induces an immune response and triggers antitumor immunity. These neoantigens are displayed on the surfaces of tumor cells and are increased in relation to mutational load because mutations increase the efficiency with which a peptide is presented by MHC molecules [1]. Recent findings based on whole-exome sequencing have revealed that different tumors have different mutational loads, suggesting that neoantigen repertoire varies according to tumor type [3]. That study showed that breast cancer has an average of one somatic mutation per megabase (Mb) of coding DNA and is expected to have moderate immunogenicity among human cancers.
Though the immunogenicity of breast cancer has not been traditionally considered in clinical practice or cancer research, the presence of tumor-infiltrating lymphocytes (TILs) in the tumor or peritumoral site has emerged as a biomarker of antitumor immune response in breast cancer. Despite the heterogeneity of TILs and the absence of a standardized methodology of evaluating TILs, recent studies have suggested that the presence of TILs is correlated with good outcome in patients with breast cancer [4-7]. With advances in understanding of the role of the immune system during carcinogenesis and tumor progression, TILs have been recognized as important biomarkers reflecting antitumor immune response in several malignancies, such as epithelial ovarian carcinoma [8,9] and endometrial cancer [10-14], as well as breast cancer.
Recent achievements in immune therapy such as adoptive T-cell therapy or dendritic cell therapy, which reactivate the antitumor immune response and immune check-points inhibiting monoclonal antibodies, have been applied in practice and have ameliorated outcomes in patients with advanced malignancies [15]. Understanding the biology and clinical utilization of TILs might offer novel therapeutic options in management of breast cancer.
In this article, we review three issues of TILs in patients with breast cancer: (1) biology of TILs, (2) methodology defining TILs, and (3) clinical evidence of TILs as biomarkers with clinical utility.
THE BIOLOGY OF TUMOR-INFILTRATING LYMPHOCYTES IN BREAST CANCER
The components of TILs
Infiltrating immune cells are frequently observed in tumors, but the proportion of immune cells comprising the host immune system is diverse and depends on the type and organ sites of malignancies [16]. Previous evidence from animal and clinical studies has shown that leukocyte subsets predominantly contribute to either tumor-suppressive or tumor-stimulating activities. In murine models, myeloid lineage leukocytes, such as dendritic cells, myeloid-derived suppressor cells, and tumor-as-sociated macrophages, have been identified and are thought to principally act to modulate the immune microenvironment toward either an antitumor milieu or a tumor-promoting milieu. T cells that migrate to tumor and/or peritumor sites are activated or inactivated and, in turn, regulate macrophage differentiation via polarization toward pro-tumorigenic M2 or antitumor M1 functional phenotypes, suggesting the importance of cell-to-cell cross-talk in the immune milieu [17].
Most TILs are T lymphocytes [18-20]. Tumor-infiltrating B lymphocytes are less common and are poorly defined [21]. The composition of TILs has been well studied in two recent publications [19]. These studies showed similar results that T lymphocytes constituted 75% of TILs, B lymphocytes made up fewer than 20%, monocytes constituted fewer than 10%, and natural killer and natural killer T cells made up fewer than 5% of all leukocytes.
To understand the role of T-lymphocyte–dominant TILs in antitumor response through adaptive immunity, it is necessary to understand the biologic characteristics and sub-classification of T cells. T cells, which are distinguished from other lymphocytes such as B cells and natural killer cells, have a T-cell receptor on the cell surface. There are several subgroups of T lymphocytes, each with a unique function. CD8+ T cells are known as cytotoxic T cells and destroy tumor cells by binding to antigen presented by MHC class I molecules, which are expressed on the membranes of all nucleated cells. These cytotoxic CD8+ T cells are regulated and can be inactivated by regulatory T cells (Treg), interleukin (IL) 10, and other cytokines, which prevent autoimmune diseases.
T helper cells (Th cells), which are also known as CD4+ T cells, mediate the immune response of other white blood cells. They assist in maturation of B cells into plasma cells and memory B cells and activate CD8+ T cells and macrophages. Th cells are activated when they come into contact with peptide antigens expressed by MHC class II molecules, which exist on the surfaces of antigen-presenting cells (APCs). This type of immune reaction is classified as type II immunity, which is distinguished from type I immunity, which is mainly conveyed by CD8+ T cells [22]. When Th cells are activated, they undergo rapid division and release cytokines mediating the active immunologic reaction. According to signaling from APCs, Th cells differentiate into various types such as Th1, Th2, Th3, Th17, Th9, or tumor-infiltrated follicular helper (Tfh) and release different cytokines to promote various active immune reactions. Among Th cells, Treg cells develop either in the thymus or in peripheral lymphoid organs. Treg cells developed in a peripheral lymphoid organ regulate adaptive immune responses [23]. The expression of forkhead box P3 protein (FOXP3) is used to identify Treg cells.
Several studies have highlighted the importance of T cells and TILs in breast cancer. Regarding the prognostic effect of cytotoxic CD8+ T cells, it is evident that the presence of these cells is significantly associated with prolonged survival outcome [5,24] and good response to chemotherapy [25]. The presence of CD8+ T cells is also associated with different subtypes of breast cancer. In a study with more than 1,200 breast cancer cases, high level of CD8+ T cells was found in the less aggressive subtypes, such as luminal cancer. In contrast, low level of CD8+ T cells was observed in HER2-positive or basal-like breast cancer [26].
In contrast to the studies with CD8+ T cells, the prognostic effect of CD4+ T cells in breast cancer is variously reported and remains inconclusive. Th1 cells, which are the primary sources of interferon-γ, were reported to correlate with favorable prognostic outcome [19], whereas Th2 cells were reported to counteract Th1 cells and attenuate the antitumor response based on analyses with immune-gene signatures [27]. A recent study defined the existence of Tfh cells and showed that an increase in CXCL13-producing Tfh cells in tertiary lymphoid structures adjacent to breast tumors is positively associated with treatment outcome and might modulate an effective and durable antitumor immune response [19]. Th17 cells also contribute to the tumor microenvironment. Particularly, the balance between Th17 cells and IL-17 family, which have pro-inflammatory functions, has an important role in regulating tumor angiogenesis. The effect of Th17 cells near tumors seems to be variable depending on the cytokine milieu [28]. The antitumor or pro-tumor effect of Th17 cells might be different depending on the type of tumor [28].
Studies with CD4+ Treg cells expressing FOXP3 remain controversial because the presence of Treg cells has been associated with both immunosuppressive and immunostimulatory activity [18,29,30]. The effects of Treg cells on prognosis differed according to immunohistochemistry (IHC) marker and type of CD4+ T cells. Interestingly, the ratio of CD8+ to FOXP3+ is correlated with molecular subtype [26] and is characterized to define medullary cancer [31]. Furthermore, a recent study showed that this ratio can be used to identify patients with good response to neoadjuvant chemotherapy in triple-negative breast cancer (TNBC) [32].
Currently, little is known regarding the role of tumor-infiltrating B cells (CD20+) as components of TILs [33,34]. Some authors have reported that increased expression of immunoglobulin κC by B cells is associated with favorable prognosis of breast cancer according to the database of gene-expression profiling [35].
Factors affecting recruitment of TILs
There are several factors responsible for lymphocyte recruitment in tumors. High endothelial venules (HEV) interact with blood vessels and contribute to lymphocyte infiltration in breast cancer [36]. The high density of HEV is related to lymphotoxin-β produced by mature dendritic cells [37] and is associated with improved survival outcome in patients with breast cancer. It has been noted that HEV density is increased in ductal carcinoma in situ compared to invasive ductal carcinoma.
Indoleamine-2,3-dioxygenase (IDO), which catalyzes the conversion of tryptophan to kynurenine, is one of the enzymes affecting lymphocytic infiltration of tumors. Tryptophan depletion inhibits both tumor cells and lymphocytes, and kynurenine has cytotoxic activity against tumors [38]. Therefore, the catalytic activity of IDO might inhibit or stimulate both tumor growth and antitumor immune functions [39].
Factors affecting TIL count and recruitment of TILs have been studied. High TIL count has been observed in patients with TNBC [25]. The presence of TILs has been shown to inversely correlate with expression of human leukocyte antigen-G, which might be involved in tumor escape [40]. The TIL count has also been reported to be associated with expression of stem cell makers or epithelial-mesenchymal transition markers in cancer cells [25].
Stromal TILs and intratumoral TILs
Depending on lymphocyte-infiltrated site, TILs are classified as infiltrated lymphocytes in the tumor stroma (stromal TILs) or in the tumor cell islets (intratumoral TILs). Stromal TILs are defined as lymphocytes dispersed in the stroma and are distinguished from intratumoral TILs, which are located within carcinoma nests and are in direct contact with tumor cells [41]. To date, most clinical trials have suggested that stromal TILs are likely to be more stable and reproducible markers than intratumoral TILs because of their increased frequency.
Efforts in methodological agreement in evaluation of TILs in breast cancer
There are many hurdles to utilizing TILs as prognostic or predictive markers because of their heterogeneity and the absence of standardized methods of evaluation. Moreover, the methodology based on IHC assessment of TILs demonstrates enormous variation in analytical practice and limits the value of TIL measurement to experimental research or specific studies. Consequently, TIL determination is not yet feasible in routine clinical practice and urgently demands a consensus in the development of a standardized measurement system.
The initial method for measuring TILs was proposed by Denkert et al. in 2010 [42], which evaluated TILs in specimens from core biopsies. Since then, the majority of researchers investigating TILs have used that method, which has now been supported by robust findings. With this background, an International TIL Working Group was recently organized, and participants with experience in evaluation of TILs in specimens from phase III clinical trials were surveyed regarding topics in the methodology of TILs evaluation. Consequently, they reported current recommendations to reconcile the method of evaluating TILs (Table 1) [43].
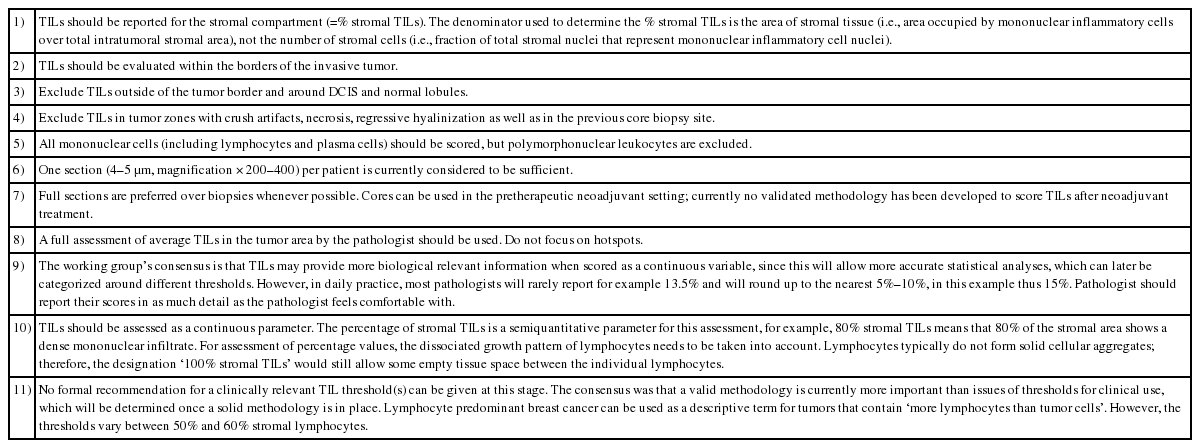
International TIL Working Group recommendations for assessing TILs in breast cancer
Clinical evidence of TILs in adjuvant or neoadjuvant studies
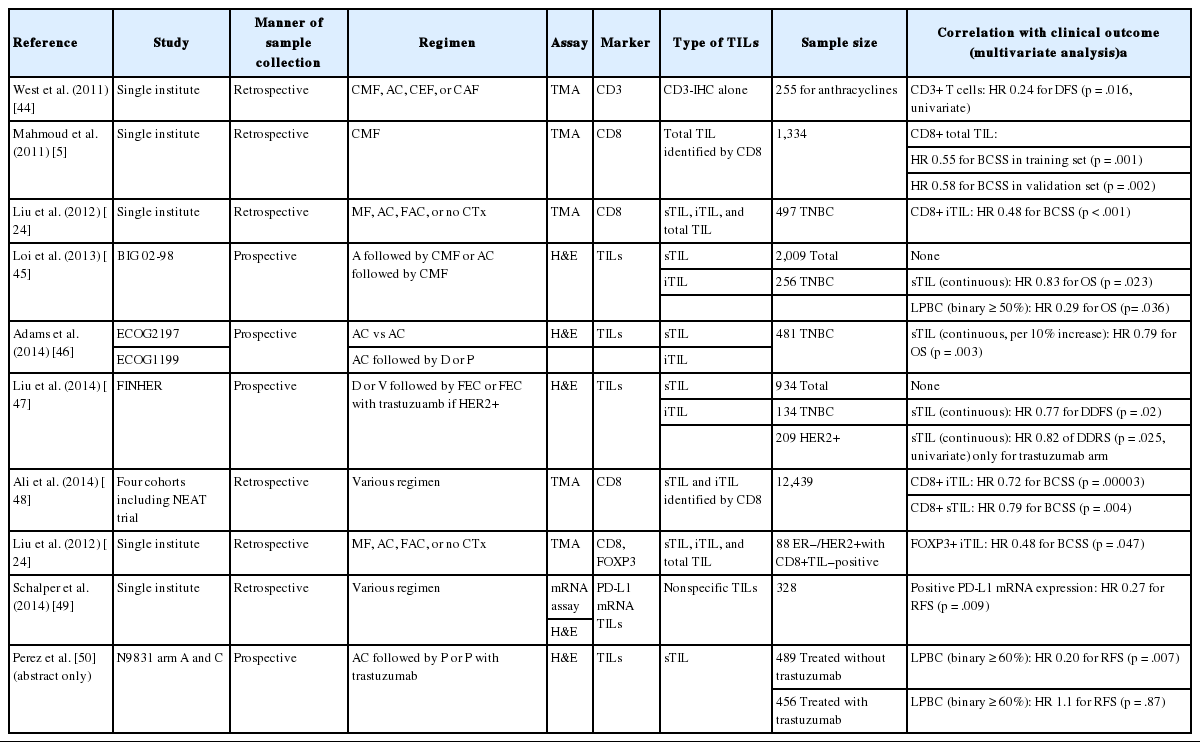
Major adjuvant or neoadjuvant studies testing TILs are presented in Tables 2 and 3 [5,24,25,35,41,42,44-57]. Most of these studies evaluated both stromal and intratumoral TILs. As described above, the measurement of stromal TILs is more reproducible among studies and has superior clinical value. Some studies have evaluated TILs using IHC, whereas others have identified the immune components of TILs based on databases of gene-expression profiling.
Adjuvant studies evaluating TILs and prognosis

The association between TILs and pathologic response in neoadjuvant studies
In 2010, the clinical significance of TILs as biomarkers associated with pathologic response was identified by Denkert et al. [42] using samples from large clinical trials. This pivotal study was the first to evaluate TILs using the protocol of the International TIL Working Group. From that time, many researchers have focused on the association between presence of TILs and clinical outcome in various cohorts.
Among these translational studies with TILs in the adjuvant setting, the most important finding is the prognostic value of stromal TILs in TNBC. The positive correlation between increase of stromal TILs and survival outcome in TNBC was initially reported using data from the BIG 2-98 trial [45]. This correlation was validated in independent cohorts of two clinical trials [46]. Interestingly, the level of TILs was not prognostic in patients with estrogen receptor (ER)–positive cancer receiving adjuvant chemotherapy. Consequently, these findings suggest that stromal TILs can be utilized as prognostic markers in a subset of breast cancer such as TNBC but not in ER-positive breast cancer. Despite the reproducibility of TILs as prognostic markers for patients with TNBC, TILs should not be used as predictive markers for chemotherapy response because of the absence of data from patients with TNBC not treated with chemotherapy.
The pronounced prognostic effect of TILs particularly in TNBC can be explained by the neoantigens described in the introduction because TNBC has higher mutational load than do non-TNBC tumors [58]. The higher mutational load of TNBC tumors enhances immunogenicity and might result in increased TIL recruiting.
Some studies have attempted to verify the prognostic significance of TILs in patients with HER2-positive breast cancer treated with adjuvant trastuzumab. Recent data from the FINHER study suggested that increased TILs are associated with better response to adjuvant trastuzumab. In the study, patients with TIL-predominant tumors showed a superior survival outcome compared to patients with non-TIL–predominant tumors after adjuvant trastuzumab [4]. Recently published data from the N9831 study, which tested the benefit of trastuzumab in HER2-positive breast cancer, also showed that patients with immunogenic tumors defined by mRNA expression of immune genes had improved survival in response to trastuzumab treatments [59]. However, there are major caveats to the results of the FINHER trial. The number of patients was small (n=209), and the prognostic value of TILs was not confirmed in multivariate analysis. Moreover, based on the same samples from the N9831 study, Perez et al. [50] demonstrated conflicting results. In exploratory analyses of TIL evaluation, stromal TILs were associated with improved relapse-free survival in patients treated with chemotherapy alone but were not shown to be associated with recurrence-free survival in patients treated with chemotherapy plus trastuzumab.
Therefore, based on the current findings, the effect of TILs in mediating the response to adjuvant trastuzumab is not conclusive. Despite the controversy regarding the role of TILs in response to HER2-targeted therapy, previous studies have suggested that TILs mediate the antitumor response of trastuzumab and have the potential to be predictive markers of trastuzumab response [4].
In addition to stromal TILs identified by hematoxylin and eosin exam, several studies have shown the prognostic value of CD8+ intratumoral TILs in adjuvant settings. Furthermore, genomic data might accelerate the discovery of immune markers or immune signatures associated with TILs or treatment outcome.
TILs have been evaluated in the samples of core biopsies from more than 3,000 patients receiving neoadjuvant chemotherapy. These studies used clinical information from prospective trials, as well as from single institutional cohorts. In an early study of a cohort of limited size, the numbers of intratumoral TILs detected by CD3 expression were significantly higher in patients with pathological complete response (pCR) [41]. Patients who achieved pCR also had significantly higher dendritic cell (CD83+) counts in specimens of core biopsies. The potential of TILs as biomarkers predicting pCR was independently confirmed using much larger cohorts of patients enrolled in the GeparDuo and GeparTrio trials. These studies showed that the percentage of intratumoral TILs is an independent predictor of pCR [42]. The studies investigating the role of TILs in patients undergoing neoadjuvant chemotherapy are summarized in Table 3. In summary, data of both histologically assessed TILs and molecular genetic signatures indicate that increased immune markers are related to higher pCR rates independent of other clinico-pathological factors or type of chemotherapy. A recent meta-analysis of TILs in neoadjuvant studies also supported the hypothesis that higher TIL level is associated with higher pCR rate [60].
CONCLUSION
Accumulating preclinical and clinical evidence supports the use of TILs as predictive and prognostic markers in breast cancer. However, it is essential to establish a standard definition of TILs and to develop a consensus for morphological evaluation of TILs before they can be applied in routine clinical practice. The heterogeneity of types and functions of lymphocytes and activating mechanisms demands molecular and functional characterization of TILs in order to improve their value. The incorporation of other biomarkers in breast cancer, such as the remaining hurdle with interobserver variability in determination of Ki-67, suggests that a biomarker cannot be widely applied in daily practice until a standardized approach has been validated in multiple studies including prospective trials. Further scientific research with TILs will offer unique insights and information on the role of the immune systems in malignancy and in treatment response.
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.