E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 48(4); 2014 > Article
-
Brief Case Report
Signet-Ring Cell Carcinoma of the Distal Common Bile Duct: Report of a Case - Hyung Jun Kwon, Ghil-Suk Yoon1, Yong Chul Kwon2, Sang Geol Kim, Ji Yun Jeong1
-
Korean Journal of Pathology 2014;48(4):315-318.
DOI: https://doi.org/10.4132/KoreanJPathol.2014.48.4.315
Published online: August 26, 2014
Department of Surgery, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, Daegu, Korea.
1Department of Pathology, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, Daegu, Korea.
2Department of Pathology, Catholic University of Daegu School of Medicine, Daegu, Korea.
-
Corresponding Author: Sang Geol Kim, M.D. Department of Surgery, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, 807 Hoguk-ro, Buk-gu, Daegu 702-210, Korea. Tel: +82-53-200-2703, Fax: +82-53-200-2027, 'ksg@knu.ac.kr'
Corresponding Author: Ji Yun Jeong, M.D. Department of Pathology, Kyungpook National University Medical Center, Kyungpook National University School of Medicine, 807 Hogukno, Buk-gu, Daegu 702-210, Korea. Tel: +82-53-420-3391, Fax: +82-53-200-2027, 'jjiyun@gmail.com'
• Received: September 30, 2013 • Revised: February 23, 2014 • Accepted: February 27, 2014
© 2014 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
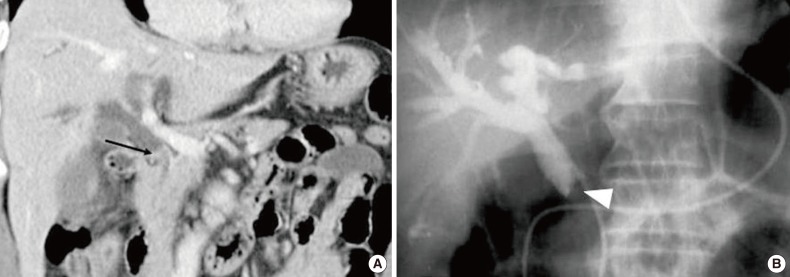
- A 63-year-old man presented with a 2-week history of epigastric pain and jaundice. His past medical history was unremarkable. Total bilirubin concentration was 9.3 mg/dL, alkaline phosphatase level was 290 IU/L (normal range, 115 to 359 IU/L), carcinoembryonic antigen was 1.1 ng/mL (normal range, 0 to 7 ng/mL), and cancer antigen 19-9 was 3.9 U/mL (normal range, 0 to 37 U/mL). Abdominal computed tomography (CT) showed wall thickening and luminal narrowing at the distal common bile duct (CBD) with proximal intrahepatic duct dilatation (Fig. 1A). Gastroduodenal fiberscopy revealed normal gastric and duodenal mucosa except a prominent ampulla, and biopsy of the ampulla showed inflammatory change. Endoscopic retrograde cholangiogram showed complete obstruction due to polypoid mass at the distal CBD and preoperative endoscopic bile drainage was performed (Fig. 1B). Upon clinical implication of carcinoma arising at the distal CBD, a pylorus-preserving pancreatoduodenectomy was performed.
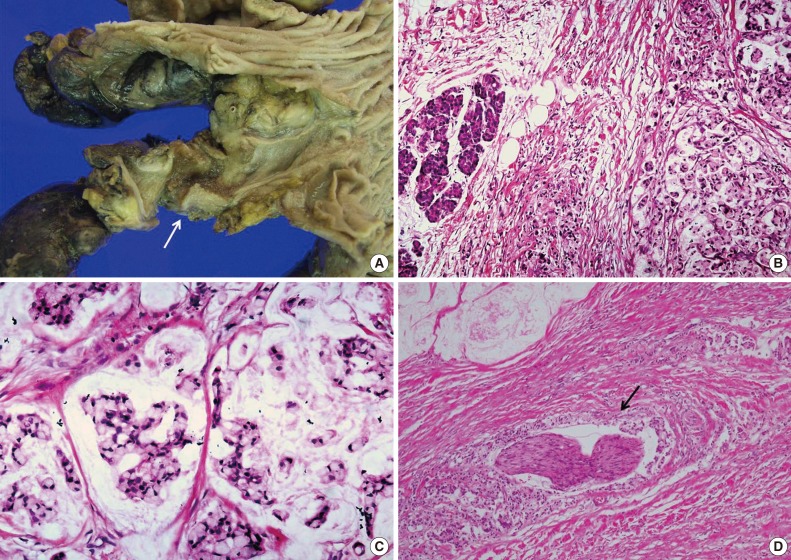
- The surgically-removed specimen showed that the ulcerofungating tumor at the distal CBD with the size of 1.5 cm in diameter (Fig. 2A). A microscopic examination of the tumor revealed diffusely infiltrative tumor cells invading into the capsule of the pancreas (Fig. 2B). The tumor cells contained abundant intracytoplasmic mucin, which pressed the nuclei toward the periphery of the tumor cells (Fig. 2C). Focal production of the mucin pool was identified, but it did not exceed 50% of the tumor. Some of the tumor cells consisted of poorly formed glandular structures, but even the tumor cells forming glands retained the same cytologic features with individually infiltrative signet-ring cells. At the interface between tumor and adjacent normal mucosa, no preneoplastic change was identified. Numerous lymphatic emboli and a few foci of perineural invasion were observed (Fig. 2D). Lymph node metastasis was not present in any of the nine submitted lymph nodes and all resection margins were free of carcinoma. TNM staging of the tumor was pT3N0M0, stage IIA according to the seventh edition of the American Joint Committee on Cancer (AJCC) cancer staging system.
- The patient's recovery was uneventful. The patient was regularly followed up. Five months after surgery, lymph node metastasis around the paraaortic area was found on abdominal CT, but the patient did not want to have chemotherapy. He died 15 months after surgery due to multiple distant metastases.
CASE REPORT
- Several cases of SRCC originating from the biliary epithelium including the ampulla of Vater, gallbladder and intrahepatic bile duct have been reported,8,9 but SRCC of the extrahepatic bile duct is extremely unusual. To the best of our knowledge, only three cases of SRCC of the extrahepatic bile duct including two Japanese and one Korean patient have been reported in the English literature.5,6,7 Clinicopathologic features of reported SRCC cases arising in the extrahepatic bile duct are summarized in Table 1. Interestingly, all four patients were Asians, but their age and follow-up data were variable.
- Because this type of variant is extremely rare in sites other than the stomach, SRCC of gastric origin should be excluded, once it is found in another site. In the present case, gastroduodenal fiberscopy revealed no mucosal lesion in the stomach, duodenum, or peri-ampullary region. Thus, it is unlikely that the tumor is a metastatic lesion.
- Although periampullary tumors require the same surgical approach, the prognosis of the tumor differs according to its origin. Tumors with a biliary epithelial origin are known to have a better prognosis than those with a duodenal or pancreatic ductal epithelial origin.10 Although the present case originated clearly from the bile duct, the patient developed lymph node metastasis around the paraaortic area at 5 months after surgery and died at 15 months after surgery. The poor prognosis may be related with presence of perineural invasion and lymphatic invasion. It is unclear whether the prognosis of SRCC of the extrahepatic bile duct is worse than that of ordinary type carcinoma at the same stage, because only rare cases of this variant have been reported. The impact of signet-ring cell type histology on the prognosis of extrahepatic bile duct carcinoma may be determined through additional reports of this unusual variant.
DISCUSSION
- 1. Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 4th ed. Lyon: IARC Press, 2010.
- 2. Kunisaki C, Shimada H, Nomura M, Matsuda G, Otsuka Y, Akiyama H. Therapeutic strategy for signet ring cell carcinoma of the stomach. Br J Surg 2004; 91: 1319–1324. PMID: 15376179. ArticlePubMed
- 3. Otsuji E, Yamaguchi T, Sawai K, Takahashi T. Characterization of signet ring cell carcinoma of the stomach. J Surg Oncol 1998; 67: 216–220. PMID: 9579367. ArticlePubMed
- 4. Malka D, Boige V, Dromain C, Debaere T, Pocard M, Ducreux M. Biliary tract neoplasms: update 2003. Curr Opin Oncol 2004; 16: 364–371. PMID: 15187892. ArticlePubMed
- 5. Hiraki M, Yakushiji H, Hashiguchil K, et al. Signet ring cell carcinoma of the lower bile duct with rapid growth: report of a case. Hepatogastroenterology 2007; 54: 1922–1924. PMID: 18251129. PubMed
- 6. Ogata S, Kimura A, Hatsuse K, et al. Poorly differentiated adenocarcinoma with signet-ring cell carcinoma of the extrahepatic bile duct in a 42-year-old Japanese female: a case report. Acta Med Okayama 2010; 64: 63–65. PMID: 20200586. PubMed
- 7. Lee EY, Kim C, Kim MJ, et al. Signet ring cell carcinoma of the extrahepatic bile duct. Gut Liver 2010; 4: 402–406. PMID: 20981222. ArticlePubMedPMC
- 8. Li L, Chen QH, Sullivan JD, Breuer FU. Signet-ring cell carcinoma of the ampulla of Vater. Ann Clin Lab Sci 2004; 34: 471–475. PMID: 15648791. PubMed
- 9. Yamauchi K, Ozeki Y, Sumi Y, Yamada T, Koyama H. A case of signet ring cell carcinoma of the gallbladder with anomalous pancreaticobiliary ductal union. Nihon Shokakibyo Gakkai Zasshi 2000; 97: 204–208. PMID: 10707592. PubMed
- 10. Dawson PJ, Connolly MM. Influence of site of origin and mucin production on survival in ampullary carcinoma. Ann Surg 1989; 210: 173–179. PMID: 2757420. ArticlePubMedPMC
References
Fig. 1Abdominal computed tomography and cholangiogram. (A) Coronal image of abdominal computed tomography shows complete obstruction of the bile duct due to the thickening of the bile duct wall (arrow). (B) Endoscopic retrograde cholangiogram shows complete obstruction at the distal common bile duct.
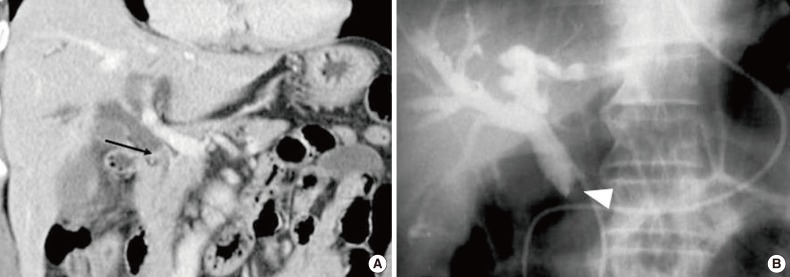
Fig. 2Macroscopic and microscopic findings of the tumor at the distal common bile duct. (A) An ulcerofungating tumor identified at the distal common bile duct (arrow). (B) Carcinoma invaded into the capsule of the pancreas. At high-power field, microscopic examination of the tumor reveal a signet-ring cell carcinoma comprising more than 50% of the tumor tissue (C), and a few perineural invasion are present (D, arrow).
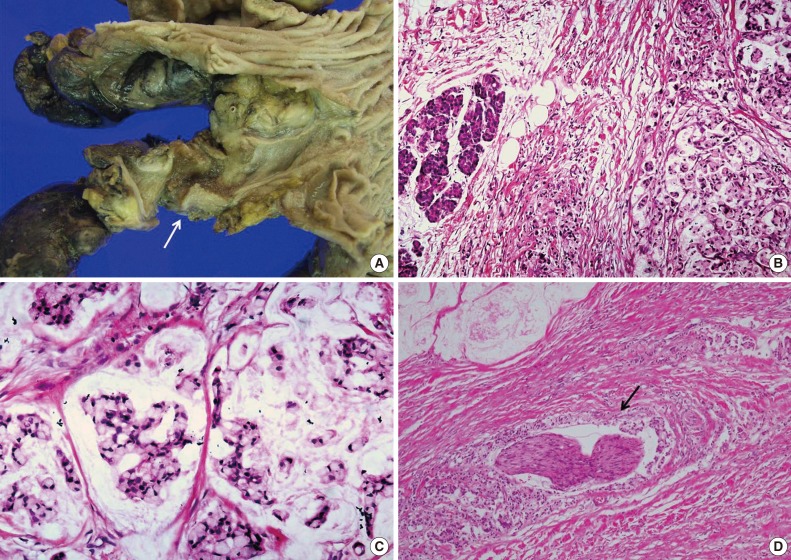
Table 1.Summary of four cases of signet-ring cell carcinoma of the extrahepatic bile duct
| Case No. | Age/Sex | Race | Chief complaint | CT findings | Treatment | Notable microscopic findings | Pathologic staging | Follow-up | Reference |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 78/F | Japanese | Not described | Bile duct thickening and stenosis | Not described (biopsy and scratch only) | Not described | No described | Not described | Hiraki et al. [5] (2007) |
| 2 | 23/M | Japanese | Jaundice | Bile duct stricture, proximal bile duct dilatation | PPPD | Portal vein wall invasion | T4N1M0 | No recurrence, for 6 mo | Ogata et al. [6] (2010) |
| 3 | 55/M | Korean | Jaundice, pruritus | Hypervascular mass | PPPD with chemoradiotherapy | Neural invasion, mucin pool formation | T3N1M0 | No recurrence, for 2 yr | Lee et al. [7] (2010) |
| 4 | 63/M | Korean | Epigastric pain, jaundice | Bile duct thickening and narrowing, proximal bile duct dilatation | PPPD | Neural invasion, lymphatic emboli | T3N0M0 | Expired, 15 mo later | Present case |
Figure & Data
References
Citations
Citations to this article as recorded by 
- Rare histotypes of epithelial biliary tract tumors: A literature review
Elena Sapuppo, Oronzo Brunetti, Dalila Tessitore, Giovanni Brandi, Nicola Di Giovanni, Guido Fadda, Claudio Luchini, Maurizio Martini, Davide Quaresmini, Antonio Russo, Mariacarmela Santarpia, Aldo Scarpa, Mario Scartozzi, Giovanni Tuccari, Tindara Franch
Critical Reviews in Oncology/Hematology.2023; 181: 103892. CrossRef - Primary signet-ring cell carcinoma of the extrahepatic bile duct: A case report
Chao-Bang Xie, Yang Wu, Feng Li, Kai-Fei Zhao, Rong-Shu Shi, Qiong Huang, Jin Ao, Di Ke
World Journal of Gastrointestinal Oncology.2022; 14(7): 1356. CrossRef - Duodenal Stenosis Due to Carcinoma of the Lower Bile Duct: A Case Report
Takumi Maki, Atsushi Irisawa, Kenji Notohara, Goro Shibukawa, Ai Sato, Akane Yamabe, Yoshitsugu Yoshida, Shogo Yamamoto, Nobutoshi Soeta, Takuro Saito
Clinical Medicine Insights: Case Reports.2020; 13: 117954762091945. CrossRef - Rapidly Progressing Primary Extrahepatic Bile Duct Signet-Ring Cell Carcinoma in a Caucasian Woman
Jessemae L. Welsh, Omar Jaber, Marina Ivanovic, Frederick C. Johlin, Rami G. El Abiad, Gerald H. Clamon, Mark C. Smith, Carlos H. F. Chan
Journal of Gastrointestinal Cancer.2018; 49(1): 63. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-