E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(2); 2013 > Article
-
Case Study
Extrapelvic Uterus-like Masses Presenting as Colonic Submucosal Tumor: A Case Study and Review of Literature - Ki Yong Na, Gou Young Kim, Kyu Yeoun Won, Hyun-Soo Kim1, Sang Won Kim2, Chi Hoon Lee3, Jae Myung Cha3
-
Korean Journal of Pathology 2013;47(2):177-181.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.2.177
Published online: April 24, 2013
Department of Pathology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
1Aerospace Medical Research Center, Aerospace Medical Center, Republic of Korea Air Force, Cheongwon, Korea.
2Department of Radiology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
3Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
- Corresponding Author: Gou Young Kim, M.D. Department of Pathology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, 892 Dongnam-ro, Gangdong-gu, Seoul 134-727, Korea. Tel: +82-2-440-7551, Fax: +82-2-440-7564, 'pathogen@medimail.co.kr'
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- A uterus-like mass (ULM) is a central cavity lined by endometrial glands and stroma and surrounded by thick-walled smooth muscles. To date, 31 cases of ULM have been reported in the English literature. ULM typically presents as a single mass and is located in the pelvic cavity. We report here a very rare case of multiple extrapelvic ULMs involving the cecum, descending colon, and mesocolon. After extensive literature research, our case appears to be the first case of multiple ULMs found in extrapelvic sites and the first case of ULM in the colon. The present case suggests that ULM should be included in the differential diagnosis of colonic submucosal tumors in female patients with chronic abdominal pain or menstruation-associated symptoms.
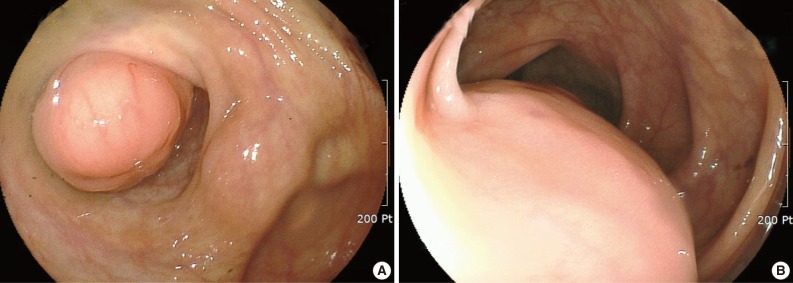
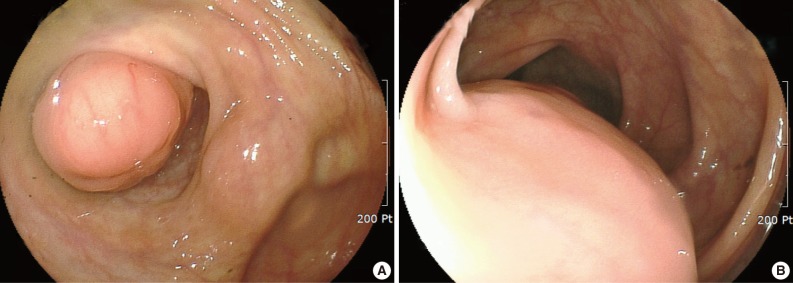
- A 39-year-old woman was admitted to the gynecology department for continuous abdominal pain in the right lower quadrant and which radiated to the right thigh. She denied dyspepsia or bowel habit changes. Her medical history was remarkable for chronic abdominal pain and ovarian endometriosis two years ago, which were managed by total hysterectomy and left salpingo-oophorectomy. Physical examination revealed mild tenderness on the suprapubic area and right lower quadrant. Laboratory data included a white blood cell count of 6,200/mm3, a hemoglobin concentration of 7.8 g/dL, and a platelet count of 397,000/mm3. The work-up for anemia revealed serum iron of 59 µg/dL, total iron-biding capacity of 454 µg/dL, serum ferritin of 70 ng/mL, and transferrin saturation of 12%, which were consistent with iron deficiency anemia. Pelvic ultrasonography revealed a 6×4 cm-sized multilocular cystic mass in the right adnexa. Ovarian endometriosis was suspected, and laparoscopic right salpingo-oophorectomy was performed. The histologic diagnosis was a hemorrhagic corpus luteum. Despite the surgery, her symptoms persisted. Considering the possibility of gastrointestinal bleeding, colonoscopy was performed. Colonoscopy demonstrated a protruding, firm submucosal mass at the appendiceal orifice of the cecum that was covered by intact mucosa (Fig. 1A). In addition, another lesion suggestive of an extrinsic compression rather than a broad based submucosal tumor was noted in the descending colon (Fig. 1B). Contrast-enhanced computed tomography of the abdomen and pelvis showed a small luminal protruding mass with enhancement in the medial wall of the cecum and another lobulating mass with contrast enhancement that contained a small internal area of low attenuation in the descending colon (Fig. 2A, B). The latter lesion was located both inside and outside of the colon and appeared dumbbell-like in shape. In addition, another small enhancing mass containing an area of low attenuation was observed in the descending mesocolon (Fig. 2C). Tumor marker levels, including alpha-fetoprotein, carcinoembryonic antigen, and carbohydrate antigen 19-9, were within normal ranges. With a presumptive diagnosis of gastrointestinal stromal tumor or intestinal endometriosis, laparoscopic exploration was performed, and the three masses were resected by cecectomy and left hemicolectomy.
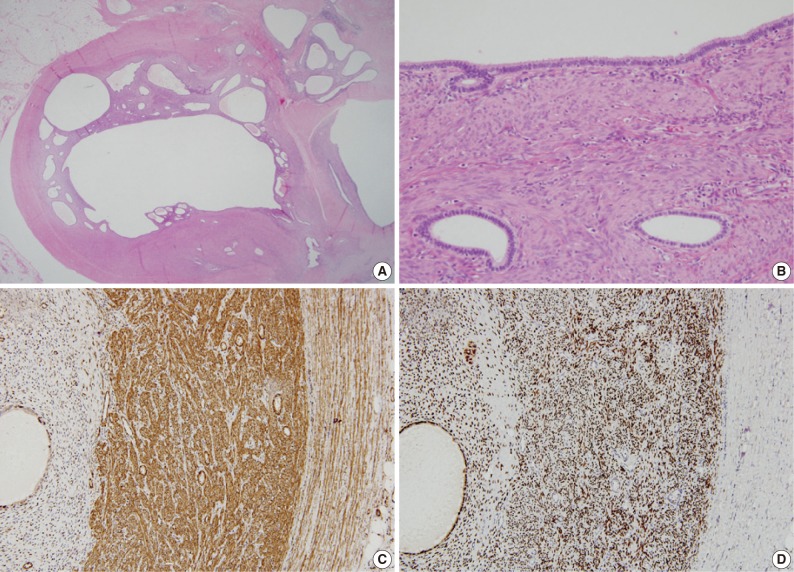
- Grossly, the cut surfaces of these masses showed a central cavity containing serosanguinous fluid, lined by a thick, soft, tan-yellow leiomyomatous wall. Histologically, the central cavity was lined by endometrial glands and stroma, which were surrounded by smooth muscles. In addition, small endometrial glands and stroma were scattered within the masses (Fig. 3A, B). On immunostaining, the endometrial glandular cells within the masses were positive for estrogen receptor (ER; 1:25, Novocastra, Newcastle upon Tyne, UK) and progesterone receptor (PR; 1:200, Novacastra). The endometrial stromal cells were positive for ER, PR, and CD10 (1:500, Novacastra) and focally positive for smooth muscle actin (SMA; 1:4,000, Dako, Glostrup, Denmark). The smooth muscle cells of the masses were positive for ER, PR, and SMA and focally positive for CD10. Colonic smooth muscles adjacent to the masses were negative for ER, PR, and CD10 (Fig. 3C, D). These findings were consistent with a previously-reported case of ULM.2
- The patient was discharged two weeks after surgery without postoperative complication. On follow-up, she reported no pain or shown evidence of anemia for 15 months.
CASE REPORT
- In the first report of ULM, Cozzutto1 suggested the use of the terms 'ULM' or 'metriosis' based on the distinctive morphologic features. Grossly, the lobular architecture and central cavity of the mass resembled that of the uterus. Histologically, the mass had a well-organized endometrium and myometrium. To date, 31 cases of ULM have been reported in the English literature with variable terms such as endomyometriosis4 and ULM with features of an extra-uterine adenomyoma.9
- The clinical features of these cases and the present case are summarized in Table 1. The ages of the patients ranged from 11 to 59 years, with most patients in their 40s and 50s. The ovary was most frequently involved (n=9), followed by the uterus (n=6), uterine ligament (n=4), and pelvic walls (n=3). The most common presenting symptom was abdominal pain (n=18), frequently associated with menstruation-related symptoms. One-third of the patients had endometriosis (n=8) or adenomyosis (n=2).
- In this case report, we describe multiple extrapelvic ULMs involving the cecum, descending colon, and mesocolon. Most ULMs have been reported in the pelvic cavity, except for three cases involving the ileum,10 ileal mesentery,11 and sigmoid mesocolon.12 To the best of our knowledge, ULM of the colonic segment has not yet been reported. Together with the three previous cases of extrapelvic ULMs, the present case supports the notion that ULMs can involve regions outside of the pelvic cavity. Another unique finding of the present case is the multiplicity of the lesions. Twenty-eight of the 31 ULMs presented as a single mass. Three previous cases of multiple ULMs were reported to involve the ovary2,5 and pelvic wall.5 We report for the first time the extrapelvic involvement of ULM, without accompaniment of the usual sites of involvement.
- In this case, a part of the mass was abutting the smooth muscles of the colon. Several histological and immunohistochemical findings distinguish the smooth muscles of the ULM and the colon. As previously mentioned by Cozzutto,1 the smooth muscle components of ULMs are histologically identical to myometrium, which have irregularly arranged muscle fibers, and are different from the inner circular and outer longitudinal smooth muscles of the colon, which have parallel arrangements. In addition, immunostaining demonstrated that the smooth muscles of the ULM were positive for ER and PR, two markers that are not found in colonic smooth muscles.
- Three theories have been suggested regarding the histogenesis of ULMs: 1) the congenital anomaly theory, 2) the heterotopia theory, and 3) the metaplasia theory. The congenital anomaly theory is supported by several reports showing the coexistence of developmental disorders in the lower gastrointestinal tract and the urinary tract in patients with ULMs. Rosai16 suggested that ULMs result from either a Müllerian duct fusion defect or a partial duplication of the Müllerian system. The heterotopias theory was suggested by Peterson et al.,10 who reported an ileal ULM in a patient with multiple anomalies in the lower genital and intestinal tracts, as well as a sacrococcygeal anomaly. In addition, based on reports of ULMs found in the spinal cords of patients with spina bifida, Rougier et al.13 and Sharma et al.6 suggested that heterotopic Müllerian duct tissue within the neural tube can result in ULMs.
- The metaplasia theory has been most widely accepted in reports of patients with ULMs who have no other identifiable malformations. In their report of an ovarian ULM, Cozzutto1 postulated that ovarian endometriosis elicits the transformation of ovarian stromal cells to smooth muscle cells via myofibroblasts. This hypothesis is linked to the observation that smooth muscle metaplasia can be associated with endometriosis. Given the reports showing the various locations of ULMs, peritoneal mesothelial cells and endometrial stromal cells have been speculated to be the sites of origin of the metaplastic cells.14 In the present case, the patient did not have any other anomalies, and therefore the metaplastic theory seems to be the most appropriate. In addition, our findings of multiple endometriotic foci outside of the mass suggest the possibility of smooth muscle metaplasia from pre-existing endometriosis. Our immunohistochemical findings of CD10-positive smooth muscle cells and SMA-positive endometrial stromal cells within the mass may reflect the close association between these cells.
- In conclusion, we have reported the first case of multiple ULMs with extrapelvic involvement in a patient with chronic abdominal pain and iron deficiency anemia. Although ULM is rare, extrapelvic ULM should be considered as a differential diagnosis for colonic submucosal tumors in female patients who have chronic abdominal pain or menstruation-associated symptoms.
DISCUSSION
- 1. Cozzutto C. Uterus-like mass replacing ovary: report of a new entity. Arch Pathol Lab Med 1981; 105: 508–511. PMID: 6895160. PubMed
- 2. Pai SA, Desai SB, Borges AM. Uteruslike masses of the ovary associated with breast cancer and raised serum CA 125. Am J Surg Pathol 1998; 22: 333–337. PMID: 9500775. ArticlePubMed
- 3. Tijani el H, Meryem T, Lamya GA, Abdelouahed J. Giant uterus-like mass of the uterus. Indian J Pathol Microbiol 2010; 53: 793–795. PMID: 21045420. ArticlePubMed
- 4. Matsuzaki S, Murakami T, Sato S, Moriya T, Sasano H, Yajima A. Endomyometriosis arising in the uterosacral ligament: a case report including a literature review and immunohistochemical analysis. Pathol Int 2000; 50: 493–496. PMID: 10886726. ArticlePubMed
- 5. Carinelli S, Motta F, Frontino G, Restelli E, Fedele L. Multiple extrauterine adenomyomas and uterus-like masses: case reports and review of the literature. Fertil Steril 2009; 91: 1956.e9–1956.e11. PMID: 19254794. ArticlePubMed
- 6. Sharma MC, Sarkar C, Jain D, Suri V, Garg A, Vaishya S. Uterus-like mass of müllerian origin in the lumbosacral region causing cord tethering: report of two cases. J Neurosurg Spine 2007; 6: 73–76. PMID: 17233296. PubMed
- 7. Rohlfing MB, Kao KJ, Woodard BH. Endomyometriosis: possible association with leiomyomatosis disseminata and endometriosis. Arch Pathol Lab Med 1981; 105: 556–557. PMID: 6895172. PubMed
- 8. Seki A, Maeshima A, Nakagawa H, et al. A subserosal uterus-like mass presenting after a sliding hernia of the ovary and endometriosis: a rare entity with a discussion of the histogenesis. Fertil Steril 2011; 95: 1788.e15–1788.e19. PMID: 21183171. ArticlePubMed
- 9. Redman R, Wilkinson EJ, Massoll NA. Uterine-like mass with features of an extrauterine adenomyoma presenting 22 years after total abdominal hysterectomy-bilateral salpingo-oophorectomy: a case report and review of the literature. Arch Pathol Lab Med 2005; 129: 1041–1043. PMID: 16048397. ArticlePubMedPDF
- 10. Peterson CJ, Strickler JG, Gonzalez R, Dehner LP. Uterus-like mass of the small intestine: heterotopia or monodermal teratoma? Am J Surg Pathol 1990; 14: 390–394. PMID: 2321701. ArticlePubMed
- 11. Horie Y, Kato M. Uterus-like mass of the small bowel mesentery. Pathol Int 2000; 50: 76–80. PMID: 10692183. ArticlePubMed
- 12. Shin SY, Kim HJ, Kim YW, Lee KY. CT characteristics of a uteruslike mass in the sigmoid mesocolon. Br J Radiol 2011; 84: e1–e3. PMID: 21172956. ArticlePubMed
- 13. Rougier A, Vital C, Caillaud P. Uterus-like mass of the conus medullaris with associated tethered cord. Neurosurgery 1993; 33: 328–331. PMID: 8367059. ArticlePubMed
- 14. Jung WY, Shin BK, Kim I. Uterine adenomyoma with uterus-like features: a report of two cases. Int J Surg Pathol 2002; 10: 163–166. PMID: 12075412. ArticlePubMed
- 15. Pai RR, Sharma L, Pinto PJ, Raghuveer CV. Endomyometriosis. J Indian Med Assoc 1995; 93: 326PMID: 8713255.
- 16. Rosai J. Uteruslike mass replacing ovary. Arch Pathol Lab Med 1982; 106: 364–365. PMID: 6896452. PubMed
References


| Authors | Age/sex | Location | Size (cm) | Clinical presentation | Treatment | Associated conditions |
|---|---|---|---|---|---|---|
| Cozzutto [1] | 32/F | Ovary | 6 | LAP | Mass excision | Unilateral renal agenesis, endometriosis |
| Pai et al. [2] | 38/F | Both ovariesa | 4 and 3 | Incidental finding | BO | Invasive ductal carcinoma |
| 43/F | Ovary | 11.5 | Pelvic mass | Mass excision | None | |
| 39/F | Ovary | 13 | LAP, vaginal spot | TH + UO | Adenomyosis | |
| Tijani et al. [3] | 35/F | Uterus | 21 | LAP, dysmenorrhea | Mass excision | None |
| Matsuzaki et al. [4] | 29/F | Uterosacral ligament | 7.5 | LAP, dysmenorrhea | Mass excision | None |
| Carinelli et al. [5] | 46/F | Pelvic wall and mesenterya | Up to 10 | LAP, constipation | Partial colectomy | Endometriosis, leiomyomatous nodules |
| 39/F | Ovary and pelvic walla | Up to 3.5 | LAP, dysmenorrhea | Mass excision | Endometriosis, leiomyomatous nodules | |
| Sharma et al. [6] | 33/F | Conus medullaris | 3 | Lower back mass | Mass excision | Spnia bifida, subcutaneous lipoma, tethered cord |
| 24/F | Conus medullaris | NA | Lower back pain | Mass excision | Tethered cord | |
| Rohlfing et al. [7] | 35/F | Obturator lymph node | 4.5 | Lymph node enlargement | TH + mass excision | Squamous cell carcinoma of cervix |
| Seki et al. [8] | 44/F | Inguinal soft tissue | 3.8 | LAP | Mass excision | Endometriosis |
| Redman et al. [9] | 50/F | Vagina | 8 | LAP, dysuria | Mass excision | Ureteral stricture |
| Peterson et al. [10] | 12/F | Ileum | 2.5 | Incidental finding | Segmental resection | Lower intestinal and urinary tract anomaly |
| Horie and Kato [11] | 59/F | Ileal mesentery | 14 | Abdominal mass | Mass excision | None |
| Shin et al. [12] | 31/F | Sigmoid mesocolon | 3 | LAP | Partial colectomy | None |
| Rougier et al. [13] | 18/F | Conus medullaris | 2.5 | Paresthesia | Mass excision | Spina bifida |
| Jung et al. [14] | 43/F | Uterus | 3 | Menorrhagia, dysmenorrhea | TH | Adenomyosis |
| 52/F | Uterus | 8 | Vulvar itching | TH+USO | Endometriosis | |
| Pai et al. [15] | 25/F | Broad ligament | 20 | Abdominal mass | Mass excision | None |
| Present case | 39/F | Cecum, colon, and mesocolona | 5 | LAP, anemia | Partial colectomy | Endometriosis |
Figure & Data
References
Citations
- Extrauterine adenomyoma: A case report and systematic review of the literature
Matteo Giorgi, Luca Labanca, Gabriele Centini, Lucia Lazzeri, Francesco Giuseppe Martire, Ester Sorrentino, Virginia Mancini, Diego Raimondo, Antonio Raffone, Daniele Neola, Anna Chiara Aru, Nassir Habib, Paolo Casadio, Renato Seracchioli, Errico Zupi
International Journal of Gynecology & Obstetrics.2024; 164(3): 869. CrossRef - Extrapelvic “Uterus Like Mass” Following Laparoscopic Morcellation Hysterectomy - a Consequence of Iatrogenic Implantation?
Neha Bakshi, Shashi Dhawan
International Journal of Surgical Pathology.2023; 31(5): 791. CrossRef - Extrauterine adenomyoma of the lesser omentum: A case report and review of the literature
Yanlin Chen, Liangyong Deng, Jingbo Zhao, Tianwen Luo, Zhong Zuo
Medicine.2022; 101(36): e30240. CrossRef - Pelvic Pain and Adnexal Mass: Be Aware of Accessory and Cavitated Uterine Mass
Pooya Iranpour, Sara Haseli, Pedram Keshavarz, Amirreza Dehghanian, Neda Khalili, Michael S. Firstenberg
Case Reports in Medicine.2021; 2021: 1. CrossRef - Endomyometriosis of the Rectum With Disseminated Peritoneal Leiomyomatosis 8 Years After Laparoscopic Myomectomy: A Case Report
Giorgio La Greca, Cristina Colarossi, Paolo Di Mattia, Cecilia Gozzo, Marco De Zuanni, Eliana Piombino, Lorenzo Memeo
Frontiers in Surgery.2021;[Epub] CrossRef - Imaging Manifestations of Accessory Cavitated Uterine Mass—A Rare Mullerian Anomaly
Tharani Putta, Reetu John, Betty Simon, Kirthi Sathyakumar, Anuradha Chandramohan, Anu Eapen
Indian Journal of Radiology and Imaging.2021; 31(03): 545. CrossRef - A rare case of ovarian adenomyoma mimicking primary invasive ovarian cancer with a contralateral serous borderline ovarian tumor: A case report and review of the literature
Viola Liberale, Alessandra Surace, Lorenzo Daniele, Luca Liban Mariani
Heliyon.2020; 6(7): e04406. CrossRef - Extrauterine adenomyoma located in the inguinal region: a case report of a 44-year-old woman
Winesh Ramphal, Chloé M L Peters, Luthy S M Alcalá, Dennis van Hamont, Paul D Gobardhan
Journal of Surgical Case Reports.2020;[Epub] CrossRef - Accessory and Cavitated Uterine Mass: Is It a Müllerian-Duct Anomaly?
Vani Malhotra, Sonia Dahiya, Smiti Nanda, Meenakshi Chauhan, Vandana Bhuria
Journal of Gynecologic Surgery.2020; 36(6): 350. CrossRef - Uterus-like mass in the right broad ligament
Lei Liu, Hui Yang, Shu-Peng Zhang
Medicine.2019; 98(38): e17246. CrossRef - Extrauterine adenomyoma: a review of the literature
P.G. Paul, Gunjan Gulati, Hemant Shintre, Sumina Mannur, George Paul, Santwan Mehta
European Journal of Obstetrics & Gynecology and Reproductive Biology.2018; 228: 130. CrossRef - Uterus-like mass
Jian He, Jie Xu, Hong-Yan Zhou
Medicine.2016; 95(39): e4961. CrossRef - Endometrioid Adenocarcinoma in an Extrauterine Adenomyoma
Michael A. Ulm, David B. Robins, Edwin M. Thorpe, Mark E. Reed
Obstetrics & Gynecology.2014; 124(2): 445. CrossRef - Endomyometriosis (“Uterus - like mass”) in an XY Male
Raul S. González, Cindy L. Vnencak-Jones, Chanjuan Shi, Oluwole Fadare
International Journal of Surgical Pathology.2014; 22(5): 421. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-