E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 46(1); 2012 > Article
-
Case Report
Hyaline Vascular Castleman Disease Involving Renal Parenchyma and a Lymph Node: A Case Report - Ji Hyun Kwon, Soo Kee Min1, Mi Kyung Shin2, Yong Seong Lee3, Young-Goo Lee3, Young Hyeh Ko4
-
Korean Journal of Pathology 2012;46(1):79-82.
DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.1.79
Published online: February 23, 2012
Department of Pathology, Hallym University Kangdong Sacred Heart Hospital, Seoul, Korea.
1Department of Pathology, Hallym University Sacred Heart Hospital, Anyang, Korea.
2Department of Pathology, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea.
3Department of Urology, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea.
4Department of Pathology, Samsung Medical Center, Sungkyungkwan University School of Medicine, Seoul, Korea.
- Corresponding Author: Soo Kee Min, M.D. Department of Pathology, Hallym University Sacred Heart Hospital, 896 Pyeongchon-dong, Dongan-gu, Anyang 431-070, Korea. Tel: +82-31-380-3938, Fax: +82-31-380-3936, 'tgmsk@hallym.ac.kr'
© 2012 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- Castleman disease is a rare lymphoproliferative lesion that is predominantly found in the mediastinum. Retroperitoneal and pararenal localizations are very rare. We describe a 36-year-old man with a hyaline vascular type of Castleman disease involving renal parenchyma and a paraaortic lymph node. Most reported renal Castleman disease was plasma cell type with systemic symptoms. Herein, we report the first Korean case of the hyaline vascular type of Castleman disease involving the renal parenchyma and the paraaortic lymph node simultaneously.
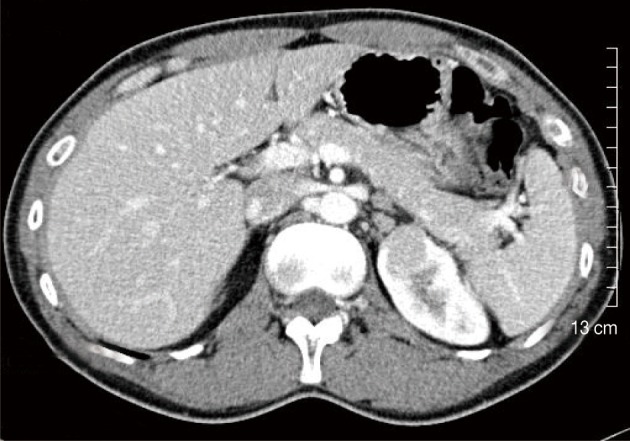
- A 36-year-old man was hospitalized due to abdominal discomfort with fatigue. His family history states that his mother died of liver cirrhosis associated with the hepatitis B virus (HBV). Physical examination indicated no abnormal findings. All laboratory findings were normal, but serum hepatitis B surface antigen, hepatitis B e antigen, and HBV DNA were positive. The human immunodeficiency virus (HIV) antibody tests were all negative. The abdominal computed tomography did not show any abnormality in the liver, but a 2.4 cm sized enhancing renal mass in the left upper pole was incidentally found. An enlarged lymph node was seen in the left paraaortic area (Fig. 1). A whole body isotope scan to assess for metastasis did not show any abnormal uptake.
- The renal mass and the enlarged lymph node were excised by robotic-assisted laparoscopic partial nephrectomy based on the preoperative impression of renal cell carcinoma, renal oncocytoma, or adenoma. Microscopic pathologic examination was performed intraoperatively, and lymphoproliferative lesion with negative margins was demonstrated by a frozen section.
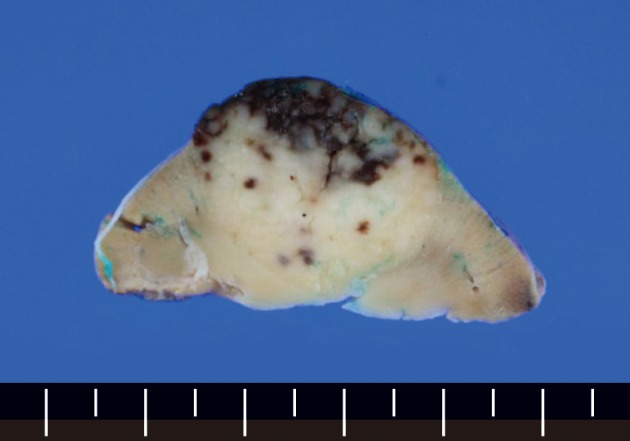
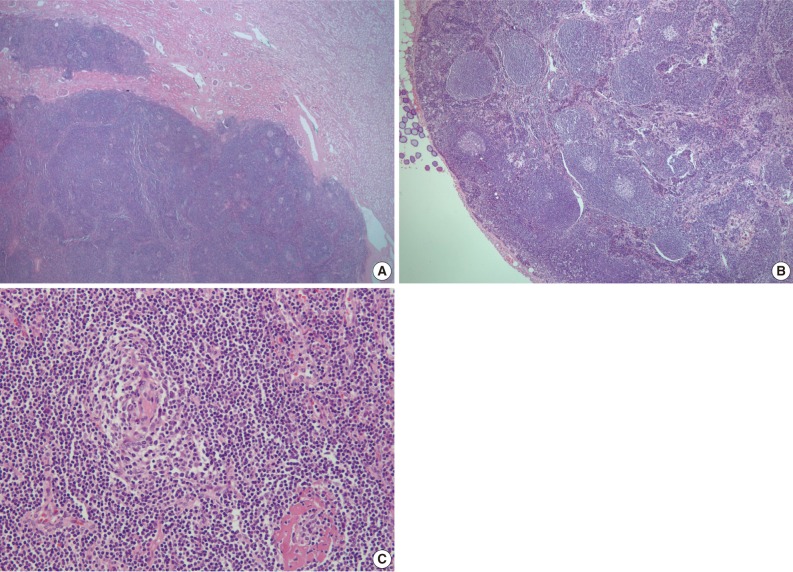
- The wedge resected specimen was 5×3×2.5 cm in size and 20 g in weight. The cut surface showed a well demarcated, white tan and solid mass measuring 2.2×1.8 cm in the renal parenchyma (Fig. 2). The paraaortic lymph node was 1 cm in its greatest dimension. The histopathological examination revealed the features of the HVCD. There were many lymphoid follicles with hyalinized germinal centers and broad mantle zones. Blood vessels were prominent in the germinal centers and the interfollicular areas. These findings were seen in the renal cortex, medulla, and the paraaortic lymph node (Fig. 3).
- Both renal tissue and lymph node tested negative for human herpsevirus 8 (HHV-8) and Epstein-Barr virus infection. The levels of interleukin 6 (IL-6) and erythrocyte sedimentation rate (ESR) were not assessed.
CASE REPORT
- CD is an unusual non-neoplastic lymphoproliferative disorder which was first described as a disease entity in 1956.1 It has been called angiofollicular lymphoid hyperplasia, giant lymph node hyperplasia and angiomatous lymphoid hyperplasia in the past.5 The cause is undetermined but is most likely related to abnormal follicular dendritic cells.
- CD arises primarily in the mediastinum, and about 70% of the reported cases tend to be of mediastinal origin, followed by lymph nodes in the abdomen, neck, and other sites.3 Retroperitoneal and pararenal localizations are very rare and CD of the kidney is extremely rare.4 To the best of our knowledge, fewer than 5 cases of CD involving the kidney that are of the localized HV type have been published in the English and Japanese literature.4,6,7 From the 1980s to 2010s, CD has been reported in Korea for more than 80 times. Of these, fewer than 15 occurred in the retroperitoneal area and only 2 in the kidney. All renal cases of CD were PC type.8,9 Our case is a HVCD involving renal parenchyma and a paraaortic lymph node simultaneously.
- CD has been generally subclassified based on histologic features into HV, PC, and mixed type. More recently, a plasmablastic variant has been described as a fourth subtype.3 However, its clinical significance is determined by another classification of extent that is localized or multicentric.5
- Nearly all cases of HV type (about 80%) and a minority of PC types (about 20%) are localized, which implies that the disorder affects a single anatomic site or a single group of lymph nodes. A localized HV type usually occurs in young people and is asymptomatic and associated with a benign clinical course. It is characterized by giant lymphoid follicles with small, regressively transformed hyalinized germinal centers and interfollicular vascular proliferation. Localized PC type usually affects mediastinal or intra-abdominal lymph nodes. This type has sheets of mature plasma cells in the interfollicular area and associated symptoms and laboratory abnormalities, such as anemia, fever, weight loss, night sweats, hypergammaglobulinemia, hypoalbuminemia and elevated ESR. Following excision of the mass, the abnormalities disappear, and the patients tend to do well overall.3
- By contrast, multicentric CD (MCD) is a systemic disease with lesions of two or more separate anatomic sites.3 MCD was first proposed in 1983 by Frizzera et al.10 Recently, MCD has been defined as "a systemic disease with multiple peripheral lymphadenopathy or multiorgan involvement."10 However, another recent studies suggested that MCD is often composed of several disease entities, including idiopathic MCD and secondary MCD due to HIV infection, autoimmune disease-associated lymphadenopathy, POEMS (polyneuropathy, organomegaly, endocrinopathy, anasarca, M-proteins and skin lesions) syndrome, and non-Hodgkin lymphomas.11
- Multicentric forms usually have histologic features of the PC type and only rarely of the HV type. Systemic symptoms tend to be more severe than those in localized PC type. The deregulated overproduction of IL-6 is responsible for symptoms. The levels of IL-6 appear to correlate with the systemic inflammatory manifestations.3 Recent reports suggested that HHV-8 has a viral homologue of human IL-6 in its genomic DNA, and HHV-8 infection stimulates B lymphocytes to induce IL-6 production. Moreover, other exogenous or endogenous factors may induce IL-6 secretion from B lymphocytes in HHV-8 negative CD.12 Nearly all HIV-positive patients and about half of HIV-negative patients with MCD have evidence of HHV-8 infection.3 However, Suda et al.13 reported that HHV-8 appears to be unrelated to the etiology of idiopathic MCD in Japan. Idiopathic MCD in Japan usually exhibits a chronic disease course, and appears to be related to a negative outcome for HHV-8 infection.
- As above, MCD lacks a clear definition to date and there are various applications. In this regard, although our case had no significant systemic symptoms, we think it can be considered as MCD, at least from an anatomic point of view.
- In summary, we report a very rare case of the multicentric HVCD involving the renal parenchyma and the paraaortic lymph node at the same time. The patient presented with a renal mass without evidence of HHV-8 infection and systemic symptoms. A few cases of multicentric HVCD have been reported before,14,15 but the renal location with involvement of regional lymph node has not been reported before in Korea.
DISCUSSION
- 1. Castleman B, Iverson L, Menendez VP. Localized mediastinal lymphnode hyperplasia resembling thymoma. Cancer 1956; 9: 822–830. PMID: 13356266. ArticlePubMed
- 2. Cokelaere K, Debiec-Rychter M, De Wolf-Peeters C, Hagemeijer A, Sciot R. Hyaline vascular Castleman's disease with HMGIC rearrangement in follicular dendritic cells: molecular evidence of mesenchymal tumorigenesis. Am J Surg Pathol 2002; 26: 662–669. PMID: 11979097. ArticlePubMed
- 3. Hsi ED. Hematopathology. 2007; Philadelphia: Churchill Livingstone Elsevier.
- 4. Hatano K, Fujita S, Tsujimoto Y, et al. Rare case of the hyaline vascular type of Castleman's disease of the kidney. Int J Urol 2007; 14: 1098–1100. PMID: 18036051. ArticlePubMed
- 5. Peterson BA, Frizzera G. Multicentric Castleman's disease. Semin Oncol 1993; 20: 636–647. PMID: 8296200. PubMed
- 6. Kaneko T, Ogushi T, Asakage Y, Kitamura T. Hyaline vascular type of Castleman's disease confined to the kidney. Nihon Hinyokika Gakkai Zasshi 2008; 99: 597–600. PMID: 18536310. ArticlePubMed
- 7. Mah NA, Peretsman SJ, Teigland CM, Banks PM. Castleman disease of the hyaline-vascular type confined to the kidney. Am J Clin Pathol 2007; 127: 465–468. PMID: 17276946. ArticlePubMed
- 8. Ryu JH, Oh JW, Kim KH, et al. Castleman disease misdiagnosed as a neoplasm of the kidney. Korean J Urol 2009; 50: 413–416. Article
- 9. Won JE, Jeong SJ, Cho JH, et al. A case of Castleman's disease with kidney involvement. Korean J Nephrol 2007; 26: 767–771.
- 10. Frizzera G, Banks PM, Massarelli G, Rosai J. A systemic lymphoproliferative disorder with morphologic features of Castleman's disease: pathological findings in 15 patients. Am J Surg Pathol 1983; 7: 211–231. PMID: 6837832. ArticlePubMed
- 11. Kojima M, Nakamura N, Tsukamoto N, et al. Clinical implications of idiopathic multicentric castleman disease among Japanese: a report of 28 cases. Int J Surg Pathol 2008; 16: 391–398. PMID: 18499694. ArticlePubMed
- 12. Yoshizaki K, Matsuda T, Nishimoto N, et al. Pathogenic significance of interleukin-6 (IL-6/BSF-2) in Castleman's disease. Blood 1989; 74: 1360–1367. PMID: 2788466. ArticlePubMedPDF
- 13. Suda T, Katano H, Delsol G, et al. HHV-8 infection status of AIDS-unrelated and AIDS-associated multicentric Castleman's disease. Pathol Int 2001; 51: 671–679. PMID: 11696169. ArticlePubMed
- 14. Park JB, Hwang JH, Kim H, et al. Castleman disease presenting with jaundice: a case with the multicentric hyaline vascular variant. Korean J Intern Med 2007; 22: 113–117. PMID: 17616028. ArticlePubMedPMC
- 15. Kim JE, Kim CJ, Park IA, et al. Clinicopathologic study of Castleman's disease in Korea. J Korean Med Sci 2000; 15: 393–398. PMID: 10983686. ArticlePubMedPMC
References
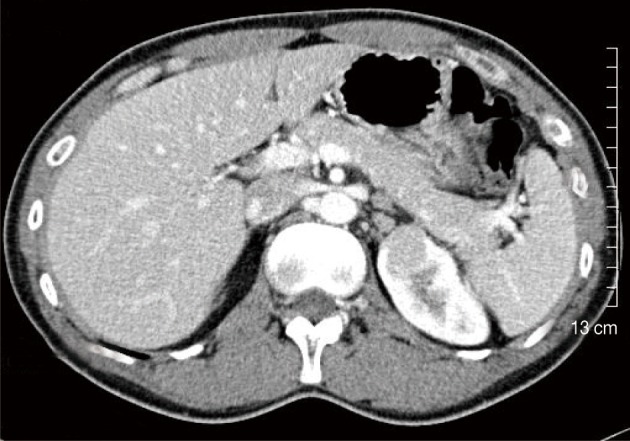
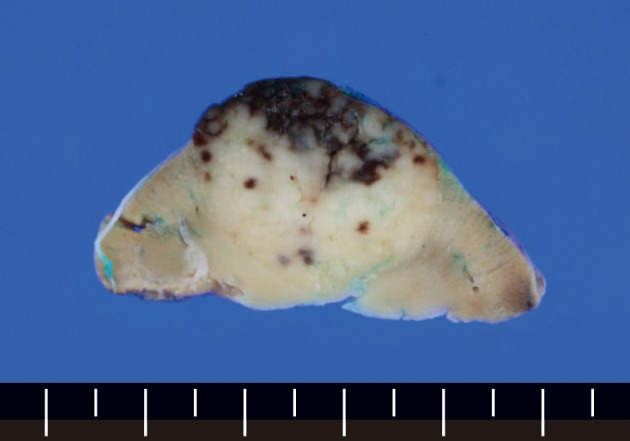
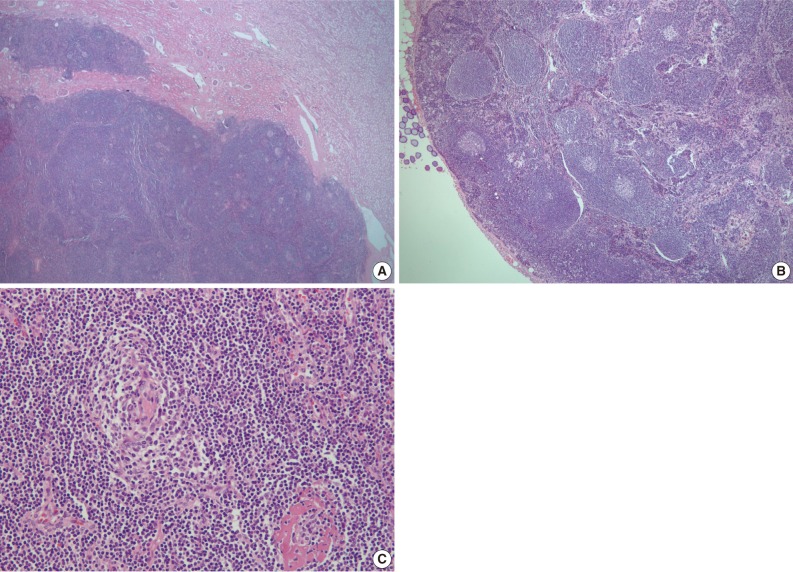
Figure & Data
References
Citations
- Castleman Disease of the Kidney in Computed Tomography Urography
Kai Wang, Fengjuan Xing, Heng Ma, Wenjuan Li
Current Medical Imaging Formerly Current Medical Imaging Reviews.2022; 18(1): 74. CrossRef - Primary hyaline vascular Castleman disease of the kidney: case report and literature review
Yunzhu Li, Haixia Zhao, Bingyin Su, Chan Yang, Shurong Li, Wanlei Fu
Diagnostic Pathology.2019;[Epub] CrossRef - Castleman’s Disease of the Kidney Mimicking Renal Cell Carcinoma on FDG PET/CT
Yang Wang, Aisheng Dong, Bo Yang, Jianping Lu
Clinical Nuclear Medicine.2018; 43(5): e160. CrossRef - Unicentric hyaline vascular type of castleman disease of the renal hilum with diagnostic dilemma: A case report and review of literature
AmitKumar Adhya, ManasRanjan Pradhan
Oncology Journal of India.2018; 2(4): 96. CrossRef
 PubReader
PubReader Cite this Article
Cite this Article