 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 57(4); 2023 > Article
-
Case Study
Metastatic choroidal melanoma in the breast: a case report and review of the literature -
Loay Abudalu,1
 , Vinisha Malhotra1, Nabila Nasir2, Sami Titi1
, Vinisha Malhotra1, Nabila Nasir2, Sami Titi1 -
Journal of Pathology and Translational Medicine 2023;57(4):238-241.
DOI: https://doi.org/10.4132/jptm.2023.06.07
Published online: July 11, 2023
1Diagnostics and Pharmacy Group, Northern Care Alliance NHS Group, Oldham Care Organization, Cellular Pathology Department, Oldham, UK
2Department of Surgery, North Manchester General Hospital Manchester, Manchester University NHS Foundation Trust, Manchester, UK
- Corresponding Author: Loay Abudalu, MD, MSc, Northern Care Alliance NHS Group, Oldham Care Organization, Cellular Pathology Department, Rochdale Road, Oldham, Ol1 2JH, UK Tel: +44-1616561878, E-mail: 'Loay.Abudalu@nca.nhs.uk'
© 2023The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,411 Views
- 98 Download
Abstract
- The breast is an unusual site for metastases, accounting for less than 2% of malignant breast lesions but include those from malignant melanomas, carcinomas, sarcomas, and lymphomas from various organs. We diagnosed a very rare case of metastatic choroidal melanoma for a 67-year-old female who presented with a right breast lump and who had been previously diagnosed with choroidal melanoma-monosomy 3 in 2017. To the best of our knowledge, only five such cases have been published so far, with one in a male patient.
- A 67-year-old female presented in 2017 with reduced vision in the left eye. A transscleral biopsy was performed, and a diagnosis of choroidal melanoma-monosomy 3 was made. The patient was treated by Ruthenium plaque brachytherapy, which was later complicated by retinal detachment. Almost a year later in follow-up, the patient underwent a computerized tomography scan of the thorax, abdomen, and pelvis and was found to have multiple lung and liver metastatic deposits. Unfortunately, the patient was lost to follow-up at this stage.
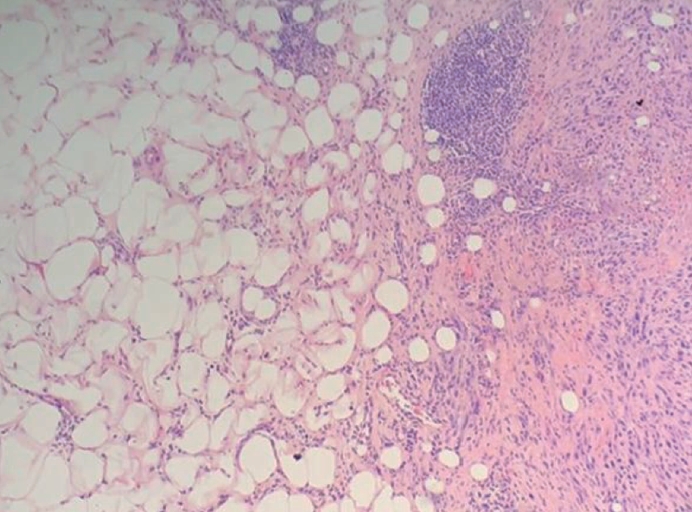
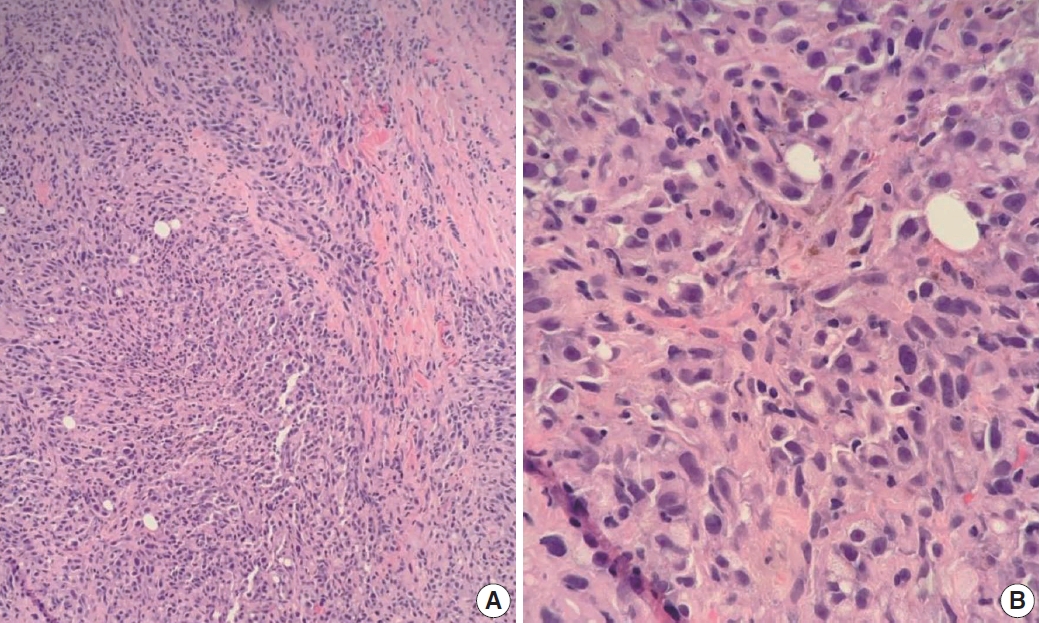
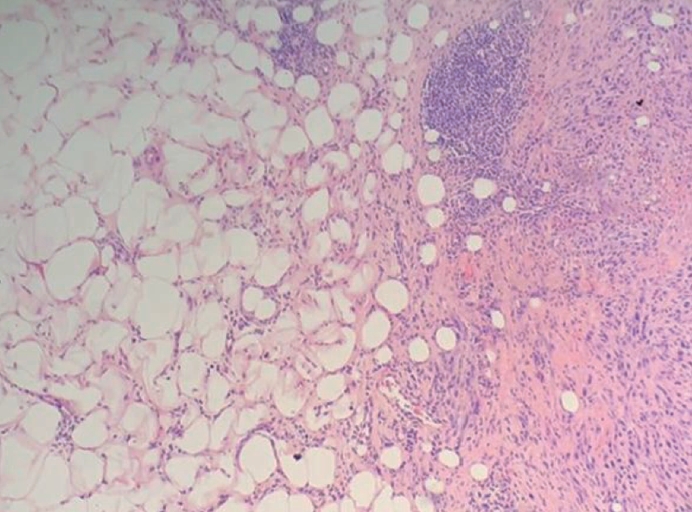
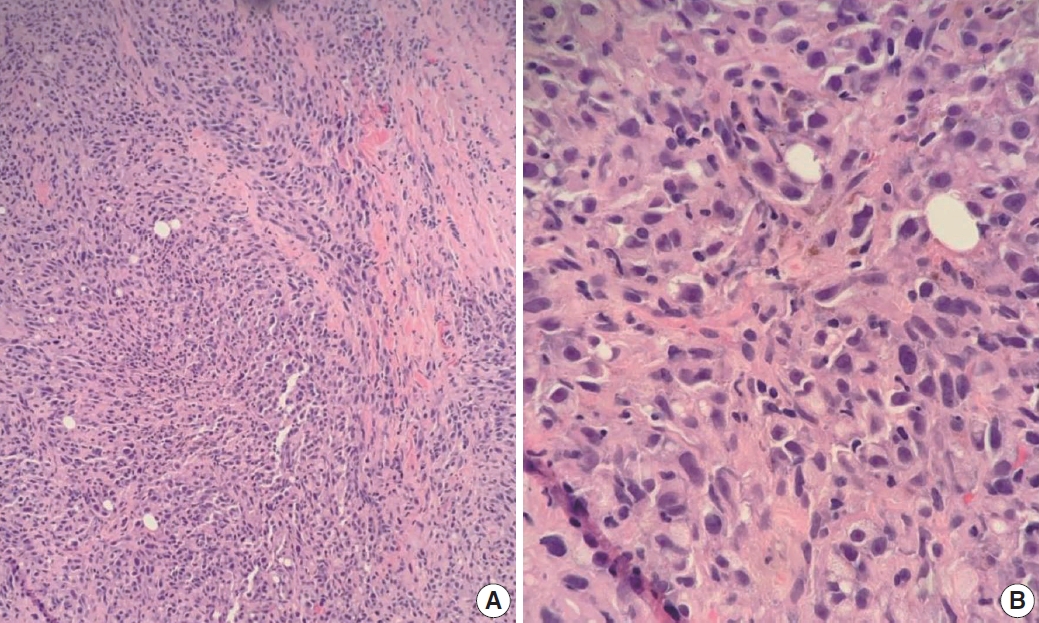
- In 2021, the patient presented with right breast lump, and ultrasound of the right breast revealed an irregular hyperechoic mass measuring 21×18×19 mm at the 12 o’clock position with features suggestive of a malignant lesion (Fig. 1). A needle core biopsy was performed and revealed an invasive tumor with some spindle cell differentiation and areas of necrosis, as shown in Figs. 2 and 3. No normal breast tissue was seen in the biopsy sample received. A provisional diagnosis of invasive ductal carcinoma with spindle cell differentiation was made, and further immunohistochemistry was requested to confirm the breast primary. The tumor cells were weakly positive for hormone receptors estrogen receptor and progesterone receptor and negative for human epidermal growth factor receptor 2.
- The case was discussed at a multidisciplinary team (MDT) meeting where more clinical information was provided. It was here revealed that the patient had a previous history of choroidal melanoma, and further immunohistochemistry was therefore performed to rule out a metastatic tumor.
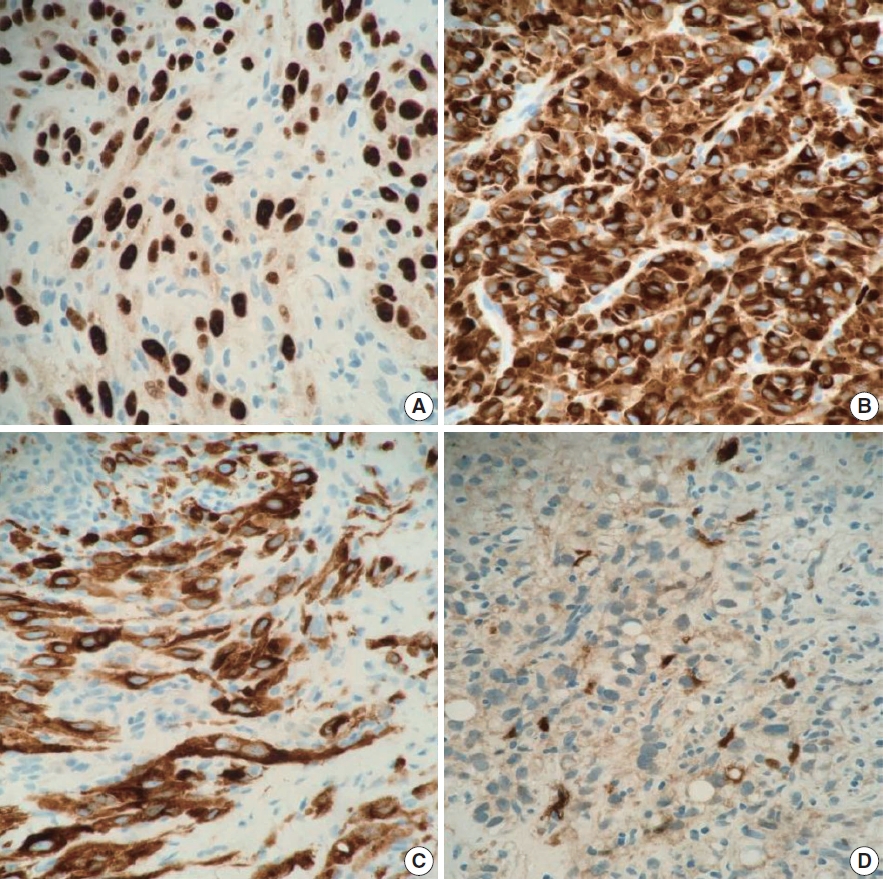
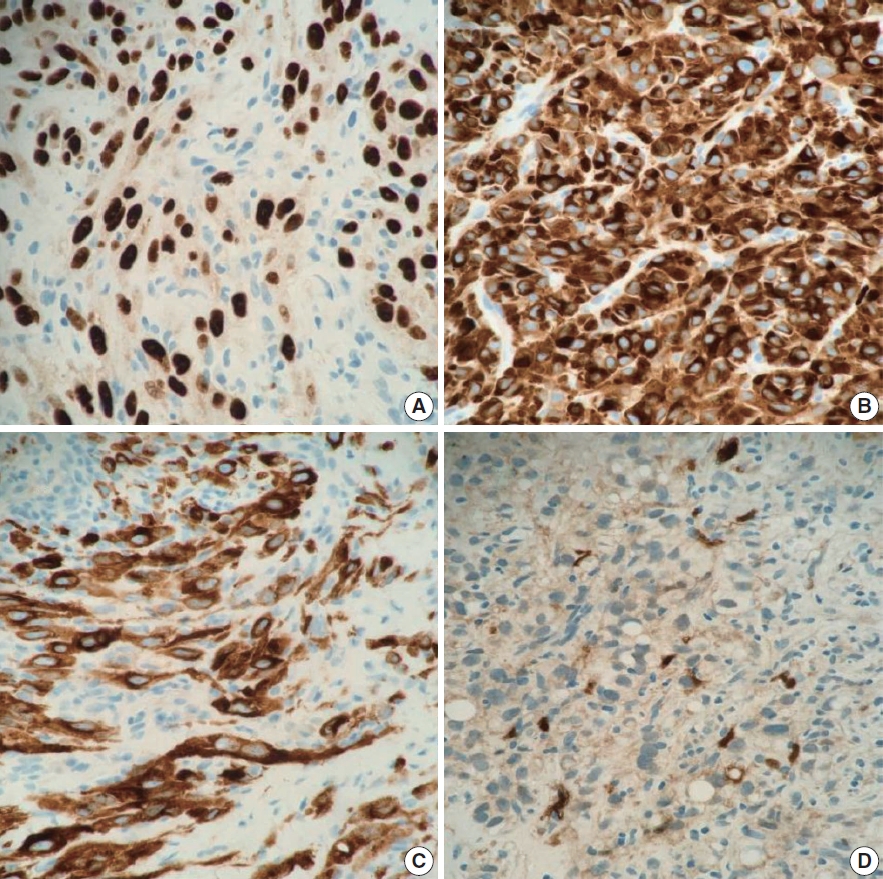
- As shown in Fig. 4, the tumor cells showed positive reaction for SOX10 (patchy), Melan-A, human melanoma black 45, and S100 (focal) and negative reaction for CK-AE1/AE3, CK5/6, CK-MNF16, thyroid transcription factor 1, CD31, p63, CD34, smooth muscle actin, desmin, and BCL2 immunostains. The overall findings were in keeping with metastatic malignant melanoma. BRAF codon 600 mutation testing was performed, and no mutation was identified. Later, head magnetic resonance imaging showed left posterior meningeal metastasis and a small enhancing lesion in the right occipital lobe, which were likely to be intracranial metastasis. The patient was referred to a specialist tumor center but refused further treatment.
CASE REPORT
- Metastatic tumors of the breast are rare, but metastatic malignant melanomas comprise approximately 38.5% of metastatic tumors [5]. The histological features of the metastatic neoplasms may be non-specific or deceiving, particularly in cases of metastatic carcinoma and melanoma. The morphological diversity of melanomas and their presence at unusual sites make diagnosis even more difficult. Even with a history of non-mammary cancer, a breast lesion is most likely to represent a primary breast cancer [6]. Breast metastasis is generally a sign of disseminated disease, and systematic screening is needed to identify metastatic deposits elsewhere.
- Malignant melanomas can be divided into primary or secondary. Primary malignant melanoma of the breast (PMMB) is a rare disease, accounting for 3%–5% of all melanomas and for less than 0.5% of malignant breast tumors. So far, 187 cases of PMMB have been reported in the literature [7].
- A study by Zhou et al. [8] found that five out of nine cases of metastatic melanoma in the breast were misdiagnosed as primary poorly differentiated invasive breast carcinoma. Of these cases, four had a history of melanoma, one had none, and this history was not known to the reporting histopathologist in all five cases. In our case, a provisional diagnosis of primary breast tumor was made due to a lack of clinical information about the patient’s history of choroidal melanoma and the rarity of metastatic tumors in the breast.
- The first case of breast metastasis from choroidal melanoma was reported by Chopra and Chandar in 1972 [9]. To the best of our knowledge, only five cases [9-13] have been published since, with one presenting in a male patient [11]. Most of the cases report breast metastasis as the first sign of metastatic disease, appearing between 50 and 60 months. In the present case, the patient presented with metastatic disease in the liver within 12 months and breast metastasis at 50 months, as in Table 1.
- As per the literature, monosomy 3 is commonly found in most cases of uveal melanomas that metastasize to the liver [13], as seen in the current case. Breast metastasis from choroidal melanoma is extremely rare. Nevertheless, clinicians should be aware of this form of metastasis when treating patients with suspicious breast lesions and a history of choroidal melanoma. This case also emphasizes the importance of relevant clinical information being available to the reporting pathologist and further supports the vital role of MDT meetings and discussions in providing high quality patient care and avoiding erroneous diagnoses.
DISCUSSION
-
Ethics Statement
No patient consent was needed for publication as patient details were completely anonymised (neither the patient nor anyone else could identify the published information).
-
Availability of Data and Material
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
-
Code Availability
Not applicable.
-
Author Contributions
Conceptualization: LA, ST. Data curation: LA, VM, ST. Formal analysis: LA, VM, ST. Investigation: LA, VM, NN, ST. Methodology: LA, VM, ST. Project administration: LA. Resources: LA. Supervision: LA, VM, ST. Validation: LA, VM, ST. Visualization: LA, VM, ST. Writing—original draft: LA, VM, ST. Writing—review & editing: LA, VM, NN, ST. Approval of final manuscript: all authors.
-
Conflicts of Interest
The authors declare that they have no potential conflicts of interest.
-
Funding Statement
No funding to declare.
Notes

| Case | Year of publication | Sex | Age (yr) | First presentation of metastasis | Time interval between primary and breast metastasis in months | |
|---|---|---|---|---|---|---|
| 1 | Our case | 2022 | Female | 67 | Liver | 50 |
| 2 | Zhou et al. [8] | 2022 | 7 cases/no details | |||
| 3 | Taran-Munteanu et al. [5] | 2016 | Female | 61 | Breast | 50 |
| 4 | Demirci et al. [10] | 2001 | Female | 48 | Breast | 37 |
| 5 | McCormick and Rennie [12] | 2001 | Female | 50 | Breast | 60 |
| 6 | Esposito et al. [11] | 1994 | Male | 72 | Breast | - |
| 7 | Chopra and Chandar [9] | 1972 | Female | 33 | Liver and spine bilateral breast | 96 |
- 1. Lee AH, Hodi Z, Soomro I, et al. Histological clues to the diagnosis of metastasis to the breast from extramammary malignancies. Histopathology 2020; 77: 303–13. ArticlePubMedPDF
- 2. Krantz BA, Dave N, Komatsubara KM, Marr BP, Carvajal RD. Uveal melanoma: epidemiology, etiology, and treatment of primary disease. Clin Ophthalmol 2017; 11: 279–89. ArticlePubMedPMCPDF
- 3. Nathan P, Cohen V, Coupland S, et al. Uveal melanoma UK national guidelines. Eur J Cancer 2015; 51: 2404–12. ArticlePubMed
- 4. Sato T. Locoregional management of hepatic metastasis from primary uveal melanoma. Semin Oncol 2010; 37: 127–38. ArticlePubMed
- 5. Taran-Munteanu L, Hartkopf A, Eigentler TK, Vogel U, Brucker S, Taran FA. A case of choroidal melanoma metastatic to the breast. Geburtshilfe Frauenheilkd 2016; 76: 579–81. ArticlePubMedPMC
- 6. DeLair DF, Corben AD, Catalano JP, Vallejo CE, Brogi E, Tan LK. Non-mammary metastases to the breast and axilla: a study of 85 cases. Mod Pathol 2013; 26: 343–9. ArticlePubMedPDF
- 7. Drueppel D, Schultheis B, Solass W, Ergonenc H, Tempfer CB. Primary malignant melanoma of the breast: case report and review of the literature. Anticancer Res 2015; 35: 1709–13. PubMed
- 8. Zhou P, Chang N, Abraham SC, et al. Metastatic nonhematopoietic neoplasms to the breast: a study of 238 cases. Hum Pathol 2022; 125: 59–67. ArticlePubMed
- 9. Chopra JS, Chandar K. Bilateral breast metastases from malignant melanoma of the eye. Aust N Z J Surg 1972; 42: 183–5. ArticlePubMed
- 10. Demirci H, Shields CL, Shields JA, Eagle RC Jr, Honavar SG. Bilateral breast metastases from choroidal melanoma. Am J Ophthalmol 2001; 131: 521–3. ArticlePubMed
- 11. Esposito A, Gentile D, Ghidotti I, Allegri M. A rare case of metastasis of choroidal melanoma in male breast: mammographic and ultrasonographic diagnosis. Radiol Med 1994; 88: 487–8. PubMed
- 12. McCormick A, Rennie I. Bilateral breast metastases from choroidal melanoma. Am J Ophthalmol 2001; 132: 951–2. ArticlePubMed
- 13. McCarthy C, Kalirai H, Lake SL, Dodson A, Damato BE, Coupland SE. Insights into genetic alterations of liver metastases from uveal melanoma. Pigment Cell Melanoma Res 2016; 29: 60–7. ArticlePubMed
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

- Related articles
-
- Intravascular NK/T-cell lymphoma: a case report and literature review
- Hepatic carcinoma expressing inhibin: case report of a proposed novel entity and review of the literature
- Juxtacortical chondromyxoid fibroma in the small bones: two cases with unusual location and a literature review
- Hepatoid thymic carcinoma: a case report of a rare subtype of thymic carcinoma
- Renal intravascular large B cell lymphoma: the first case report in Korea and a review of the literature

