E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 54(4); 2020 > Article
-
Original Article
Highly prevalent BRAF V600E and low-frequency TERT promoter mutations underlie papillary thyroid carcinoma in Koreans -
Sue Youn Kim1
 , Taeeun Kim2, Kwangsoon Kim3, Ja Seong Bae3, Jeong Soo Kim3, Chan Kwon Jung,1,4
, Taeeun Kim2, Kwangsoon Kim3, Ja Seong Bae3, Jeong Soo Kim3, Chan Kwon Jung,1,4 -
Journal of Pathology and Translational Medicine 2020;54(4):310-317.
DOI: https://doi.org/10.4132/jptm.2020.05.12
Published online: June 15, 2020
1Department of Hospital Pathology, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Molecular Pathology Unit, Pathology Laboratory, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Department of Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea
4Cancer Research Institute, College of Medicine, The Catholic University of Korea, Seoul, Korea
- Corresponding Author: Chan Kwon Jung, MD, PhD, Department of Pathology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea Tel: +82-2-2258-1622, Fax: +82-2-2258-1627, E-mail: 'ckjung@catholic.ac.kr'
© 2020 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- The presence of telomerase reverse transcriptase (TERT) promoter mutations have been associated with a poor prognosis in patients with papillary thyroid carcinomas (PTC). The frequency of TERT promoter mutations varies widely depending on the population and the nature of the study.
-
Methods
- Data were prospectively collected in 724 consecutive patients who underwent thyroidectomy for PTC from 2018 to 2019. Molecular testing for BRAF V600E and TERT promoter mutations was performed in all cases.
-
Results
- TERT promoter alterations in two hotspots (C228T and C250T) and C216T were found in 16 (2.2%) and 4 (0.6%) of all PTCs, respectively. The hotspot mutations were significantly associated with older age at diagnosis, larger tumor size, extrathyroidal extension, higher pathologic T category, lateral lymph node metastasis, and higher American Thyroid Association recurrence risk. The patients with C216T variant were younger and had a lower American Thyroid Association recurrence risk than those with hotspot mutations. Concurrent BRAF V600E was found in 19 of 20 cases with TERT promoter mutations. Of 518 microcarcinomas measuring ≤1.0 cm in size, hotspot mutations and C216T variants were detected in five (1.0%) and three (0.6%) cases, respectively.
-
Conclusions
- Our study indicates a low frequency of TERT promoter mutations in Korean patients with PTC and supports previous findings that TERT promoter mutations are more common in older patients with unfavorable clinicopathologic features and BRAF V600E. TERT promoter mutations in patients with microcarcinoma are uncommon and may have a limited role in risk stratification. The C216T variant seems to have no clinicopathologic effect on PTC.
- Patients
- We reviewed the prospectively collected data from 724 consecutive patients who underwent thyroidectomy for PTC and molecular testing at Seoul St. Mary’s Hospital of the Catholic University of Korea from 2018 to 2019. Molecular tests for BRAF and TERT promoter mutations were performed in all patients who agreed to allow molecular analysis of their surgical specimens. In cases of multifocal PTCs, the largest tumor was defined as the primary lesion and was chosen for evaluation. The histologic variants of PTC were classified following the diagnostic criteria and terminology of the World Health Organization [7]. The tall cell variant was defined using 30% of tall cell area as a criterion. The PTCs were further classified as classic PTC with tall cell features if it harbored between 10%–30% tall cells and as classic PTC if it contained less than 10% of tall cell area and any well-formed papillae. Cancer staging was done using the 8th edition of the American Joint Committee on Cancer (AJCC) staging system [20]. Minimal extrathyroidal extension was defined as extrathyroidal invasion that was restricted to the perithyroidal soft tissues detected only on microscopic examination (including microscopic strap muscle invasion). When strap muscle invasion was found on preoperative imaging and/or at the time of surgery, the case was considered as gross extrathyroidal extension. Risk stratification of patients for tumor recurrence was done using the 2015 American Thyroid Association (ATA) guidelines [21].
- Mutational analyses for TERT promoter and BRAF V600E mutations
- Genomic DNA was extracted from 10 μm-thick formalin-fixed paraffin-embedded (FFPE) tissue blocks using a Maxwell 16 FFPE Tissue LEV Purification Kit (Promega, Fitchburg, WI, USA). Tumor areas were manually dissected with a scalpel under a microscope.
- The TERT promoter was amplified using the nested polymerase chain reaction (PCR) method. The first-round 235-bp PCR amplicon was amplified using forward 5'-AGTGGATTCGCGGGCACAGA-3' and reverse 5'-CAGCGCTGCCTGAA ACTC-3' primers. Then, the second-round 163-bp PCR amplicon was amplified using forward 5'-GTCCTGCCCCTTCACCTT3' and reverse 5'-CAGCGCTGCCTGAAACTC-3' primers. Bidirectional Sanger sequencing was performed in both directions using the same primers that were used for the second-round PCR. BRAF V600E mutation was analyzed using the real-time PCR clamping technology of PNAClampTM BRAF kit (Panagene, Daejeon, Korea) [22]. Each test had a positive control of mutation-holding human genomic DNA and a negative control of distilled water.
- Statistical analysis
- Categorical variables were analyzed using the Pearson’s chi-square, Fisher exact test, or linear-by-linear association when appropriate. Continuous variables were compared using the Student’s t-test or Mann-Whitney test when appropriate. The statistical significance threshold was defined as a p-value less than 0.05. All statistical analyses were done using SPSS Statistics program, ver. 21.0 (IBM Corp., Armonk, NY, USA).
MATERIALS AND METHODS
- Demographic and clinicopathologic characteristics
- Table 1 summarizes the baseline clinicopathologic characteristics of the 724 patients with PTC. The median age of the patients at the time of diagnosis was 46 years (interquartile range [IQR], 36 to 56 years). The female to male ratio was 2.7:1. The median tumor size was 0.7 cm (IQR, 0.5 to 1.1 cm). The proportion of microcarcinomas (≤1.0 cm in size) was 71.5% (518/724). Lobectomy was done in 504 (69.6%) and total thyroidectomy in 191 patients (26.4%). The numbers of patients with minimal and gross extrathyroidal extension were 405 (55.9%) and 41 (5.7%), respectively. Cervical lymph node metastases were found in 409 patients (56.5%).
- Frequency of TERT promoter and BRAF V600E mutations
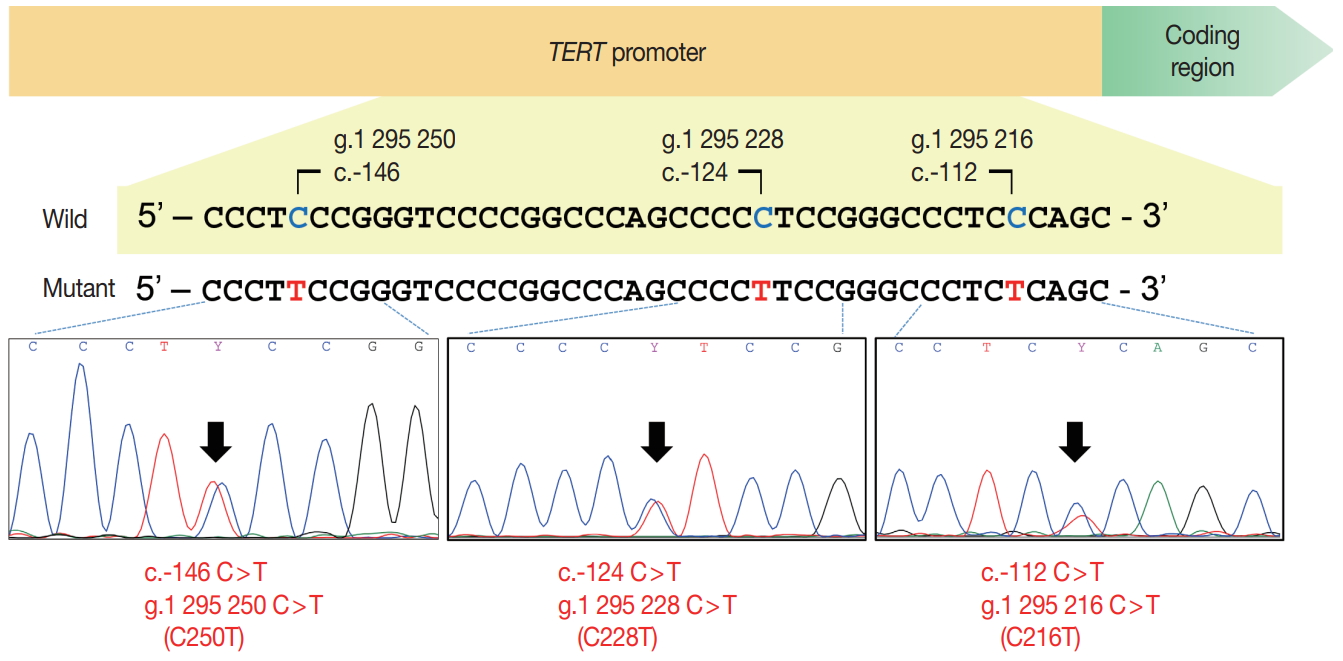
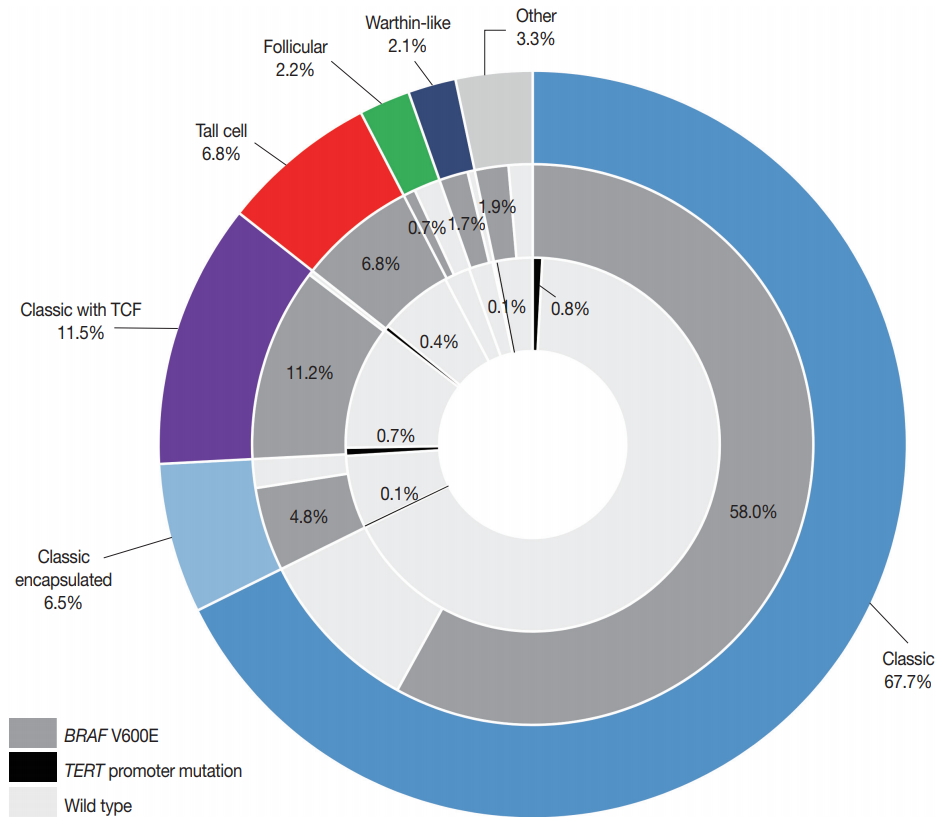
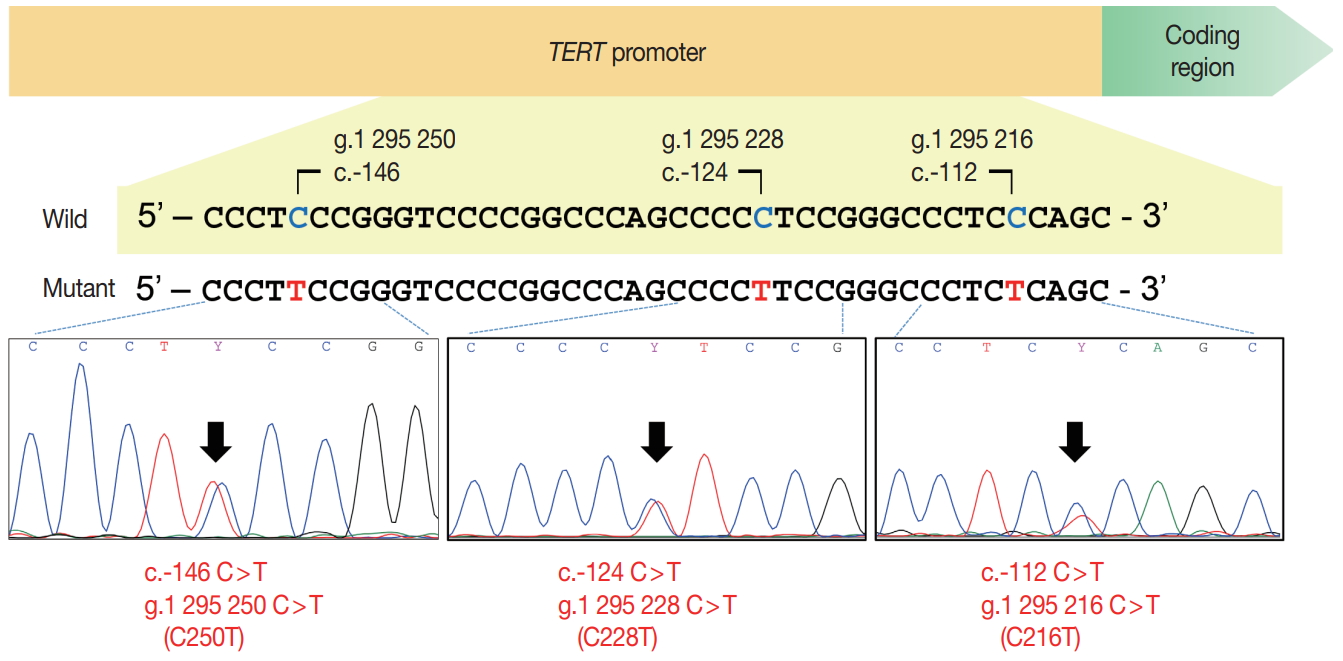
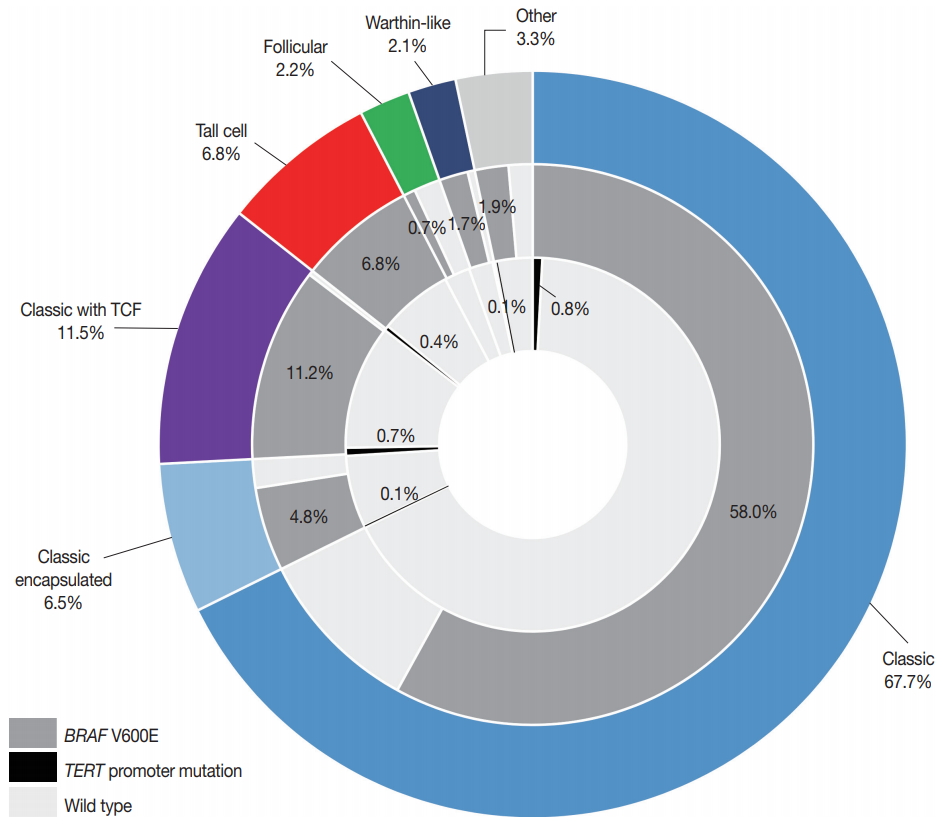
- Hotspot-point mutations (C228T and C250T) in the TERT promoter were found in 16 (2.2%) patients: 14 with C228T and two with C250T (Table 2, Fig. 1). Four cases had the TERT promoter variant of g.1 295 216 C>T (c.–112C>T) (hereafter C216T) (Fig. 1). The BRAF V600E mutation was found in 616 (85.1%) patients. Of 20 PTCs with TERT promoter aberrations, 19 had coexisting BRAF V600E (Table 3, Fig. 2). Fig. 2 summarizes the distribution of histologic variants of PTC and mutational profiles according to the variants. There was no correlation between TERT promoter mutations and histologic variants.
- Clinicopathologic features of patients with TERT promoter mutation
- Hotspot mutations in the TERT promoter were significantly associated with age ≥55 years (p<.001), tumor size >1.0 cm (p=.001), extrathyroidal extension (p=.032), lateral lymph node metastasis (p=.041), and higher ATA recurrence risk (p<.001) (Table 2). Compared with patients with hotspot mutations, those with C216T variant were younger (p=.032) and had a lower rate of high ATA recurrence risk (p=.014). There were no significant differences in the clinicopathologic features between the patients with wild-type TERT promoter mutations and those with C216T variant of the TERT promoter (Table 2). Table 3 shows the detailed clinicopathologic features of the patients with a TERT promoter mutation.
RESULTS
- The strength of this study stems from the prospectively collected data encompassing all consecutive patients treated for PTC with thyroid surgery. In our study, almost three-quarters of patients with PTC underwent thyroid surgery before the age of 55 years (73.3%) and had microcarcinomas (71.5%). Gross extrathyroidal extension was found in only 41 patients (5.7%). No case developed synchronous distant metastasis. Therefore, it stands to reason that the vast majority (86.0%) of patients with PTC were assigned to stage I by the 8th edition of the AJCC staging system. Although BRAF V600E mutations were highly prevalent in our study cohort, the frequency of hotspot mutations in the TERT promoter was 2.2%, which is far lower than that reported in previous studies for PTC (pooled mean prevalence of 11.3%) [14,23]. These results indicate that most PTC tumors in the current study should have indolent behavior.
- In our study, additional benefits were gained by including microcarcinomas in the molecular analysis. Hotspot mutations of the TERT promoter were found in five of 518 papillary microcarcinomas (1.0%). Minimal extrathyroidal extension, found in three of the five patients with hotspot mutations, did not affect the pathologic T category. Patient age ranged from 39 to 84 years. Although the frequency of TERT promoter mutations is lower than that of previous studies, these findings are in line with a previous Italian study showing no correlation with unfavorable outcomes [24]. The Italian study showed that TERT promoter mutations were found in 4.7% of papillary microcarcinomas and were not associated with poor clinical features [24]. As active surveillance is one of the treatment options for low-risk papillary microcarcinomas, the identification of TERT promoter mutations may facilitate decision-making on appropriate candidates for active surveillance [21,25]. One Japanese study reported that no TERT promoter mutations were found in 25 patients selected from 1,252 patients with low-risk papillary microcarcinoma who were managed with active surveillance [25]. These results, however, need to be validated in further larger studies.
- Since most studies reported only pathogenic hotspot mutations, little is known about the prevalence and functional role of the TERT promoter C216T variant in human cancers. The C216T variant was found in four cases of our study cohort and has been previously reported in two lung adenocarcinomas [26] and one esophageal squamous cell carcinoma [27]. In our study, all four patients with the C216T were younger (range, 29 to 55 years) than those with hotspot mutations and had no unfavorable clinicopathologic features. Therefore, we suggest that the TERT promoter C216T variant may be a non-pathogenic DNA polymorphism in PTC.
- Many studies have shown synergistic effects of concurrent BRAF V600E and TERT promoter mutations on the poor prognosis and mortality risk of patients with PTC [8,11,17-19,23]. The C228T and C250T mutations of the TERT promoter generate an 11-bp binding motif (5'-CCCCTTCCGGG-3') for E-twentysix (ETS) transcription factors [13]. Mitogen-activated protein kinase pathway activation by the BRAF V600E mutation upregulates ETS transcription factors, which results in increased TERT mRNA expression by the binding of the mutated TERT promoter to ETS [28]. In our study, all 14 patients with the TERT promoter C228T mutation had a concurrent BRAF V600E mutation. In Korean patients with PTC and a high prevalence of the BRAF V600E, further studies are needed to validate the prognostic utility of risk stratification of patients with PTC by combining BRAF V600E and TERT promoter mutations.
- In summary, this study demonstrated that the TERT promoter mutation frequency was 2.2% in prospectively collected patients, and the presently reported frequency is lower than that reported in previous studies. TERT promoter mutations were more common in older patients with unfavorable clinicopathologic features and a BRAF V600E mutation. Although they were observed less frequently than in those with larger tumors, TERT promoter mutations also occurred in patients with microcarcinoma and low-risk clinicopathologic features. The C216T variant was found in 0.6% of all PTCs and may be a non-pathogenic DNA polymorphism.
DISCUSSION
-
Ethics Statement
This study was approved by the Institutional Review Board of Seoul St. Mary’s Hospital, the Catholic University of Korea (KC16SISI0709). Informed consent was obtained from each patient.
-
Author contributions
Conceptualization: CKJ. Data curation: SYK, TK, KK, JSB, JSK, CKJ. Formal analysis: SYK, TK, CKJ. Funding acquisition: CKJ. Investigation: SYK, TK, CKJ. Methodology: SYK, TK, CKJ. Project administration: SYK, CKJ. Resources: SYK, KK, JSB, JSK, CKJ. Software: SYK, CKJ. Supervision: CKJ. Validation: KK, JSB, JSK, CKJ. Visualization: SYK, KK, JSB, JSK, CKJ. Writing—original draft: SYK, CKJ. Writing—review & editing: SYK, TK, KK, JSB, JSK, CKJ. Approval of final manuscript: all authors.
-
Conflicts of Interest
C.K.J. is the editor-in-chief of the Journal of Pathology and Translational Medicine and was not involved in the editorial evaluation or decision to publish this article. All remaining authors declare that they have no potential conflicts of interest.
-
Funding
This study was supported by a grant (2017R1D1A1B03029597) from the Basic Science Research Program through the National Research Foundation of Korea.
Notes
| Characteristic | No. (%) (n = 724) |
|---|---|
| Age at diagnosis (yr) | 45.9 ± 13.0 |
| < 55 | 531 (73.3) |
| ≥ 55 | 193 (26.7) |
| Sex | |
| Female | 528 (72.9) |
| Male | 196 (27.1) |
| Tumor size (cm) | |
| ≤ 1.0 | 518 (71.5) |
| > 1.0 | 206 (28.5) |
| Surgical procedure | |
| Lobectomy | 504 (69.6) |
| Total thyroidectomy | 191 (26.4) |
| Isthmusectomy | 29 (4.0) |
| Histologic types | |
| Classic | 490 (67.7) |
| Classic with tall cell features | 83 (11.5) |
| Classic encapsulated | 46 (6.4) |
| Tall cell variant | 49 (6.8) |
| Warthin-like variant | 15 (2.1) |
| Infiltrative follicular variant | 10 (1.4) |
| Invasive encapsulated follicular variant | 6 (0.8) |
| Diffuse sclerosing variant | 8 (1.1) |
| Oncocytic variant | 8 (1.1) |
| Solid variant | 5 (0.7) |
| Hobnail variant | 3 (0.4) |
| Cribriform-morular variant | 1 (0.1) |
| Extrathyroidal extensiona | |
| Absent | 278 (38.4) |
| Minimal (microscopic) | 405 (55.9) |
| Gross (strap muscle invasion, pT3b) | 30 (4.1) |
| Gross (tracheal, esophageal or recurrent laryngeal nerve invasion, pT4a) | 11 (1.5) |
| Pathologic T categorya | |
| pT1 | 651 (89.9) |
| pT2 | 30 (4.1) |
| pT3 | 32 (4.4) |
| pT4 | 11 (1.5) |
| Lymph node metastasisa | |
| Absent (pN0) | 315 (43.5) |
| Central lymph node (pN1a) | 346 (47.8) |
| Lateral lymph node (pN1b) | 63 (8.7) |
| ATA recurrence risk | |
| Low risk | 241 (33.3) |
| Intermediate risk | 358 (49.4) |
| High risk | 125 (17.3) |
| AJCC cancer staginga | |
| Stage I | 623 (86.0) |
| Stage II | 98 (13.5) |
| Stage III | 3 (0.4) |
| Stage IV | 0 |
| BRAF V600E mutation | |
| Absent | 108 (14.9) |
| Present | 616 (85.1) |
| TERT promoter mutation | |
| Wild | 704 (97.2) |
| C228T mutation | 14 (1.9) |
| C250T mutation | 2 (0.3) |
| C216T variant | 4 (0.6) |
| Variable |
TERT promoter alteration, n (%) |
p-value |
||||
|---|---|---|---|---|---|---|
| Wild-type (A) | C228T, C250T (B) | C216T (C) | A vs. B | B vs. C | A vs. C | |
| Age at diagnosis (yr) | < .001 | .032 | > .99 | |||
| < 55 | 526 (99.1) | 2 (0.4) | 3 (0.6) | |||
| ≥ 55 | 178 (92.2) | 14 (7.3) | 1 (0.5) | |||
| Sex | .776 | .587 | .295 | |||
| Female | 515 (97.5) | 11 (2.1) | 2 (0.4) | |||
| Male | 189 (96.4) | 5 (2.6) | 2 (1.0) | |||
| Tumor size (cm) | .001 | .255 | > .99 | |||
| ≤ 1.0 | 510 (98.5) | 5 (1.0) | 3 (0.6) | |||
| > 1.0 | 194 (94.2) | 11 (5.3) | 1 (0.5) | |||
| Histologic variant | .313 | .214 | .405 | |||
| Classica | 603 (97.4) | 12 (1.9) | 4 (0.6) | |||
| Classic with TCF | 78 (94.0) | 5 (6.0) | 0 | |||
| Tall cell variant | 46 (93.9) | 3 (6.1) | 0 | |||
| Follicular variantb | 16 (100) | 0 | 0 | |||
| Otherc | 39 (97.5) | 1 (2.5) | 0 | |||
| Extrathyroidal extension | .032 | .162 | .645 | |||
| Absent | 274 (98.6) | 2 (0.7) | 2 (0.7) | |||
| Presentd | 430 (96.4) | 14 (3.1) | 2 (0.4) | |||
| Pathologic T category | < .001 | .267 | > .99 | |||
| pT1-2 | 667 (97.9) | 10 (1.5) | 4 (0.6) | |||
| pT3-4 | 37 (86.0) | 6 (14.0) | 0 | |||
| Pathologic N category | .297 | .619 | .322 | |||
| pN0 | 304 (96.2) | 9 (2.8) | 3 (0.9) | |||
| pN1 | 400 (98.0) | 7 (1.7) | 1 (0.2) | |||
| Lateral lymph node metastasis | .041 | > .99 | .294 | |||
| Absent | 646 (97.7) | 12 (1.8) | 3 (0.5) | |||
| Present | 58 (92.1) | 4 (6.3) | 1 (1.6) | |||
| ATA recurrence risk | < .001 | .014 | .344 | |||
| Low risk | 237 (98.3) | 2 (0.8) | 2 (0.8) | |||
| Intermediate risk | 354 (98.9) | 2 (0.6) | 2 (0.6) | |||
| High risk | 113 (90.4) | 12 (9.6) | 0 | |||
| AJCC cancer staging, 8th edition | .065 | > .99 | > .99 | |||
| Stage I/II | 702 (97.4) | 15 (2.1) | 4 (0.6) | |||
| Stage III/IV | 2 (66.7) | 1 (33.3) | 0 | |||
| BRAF V600E mutation | .489 | > .99 | > .99 | |||
| Absent | 107 (99.1) | 1 (0.9) | 0 | |||
| Present | 597 (96.9) | 15 (2.4) | 4 (0.6) | |||
TERT, telomerase reverse transcriptase; TCF, tall cell features; ATA, American Thyroid Association; AJCC, American Joint Committee on Cancer.
a Classic papillary thyroid carcinoma (PTC) included classic PTC (n = 490), classic PTC with tall cell features (n = 83) and encapsulated classic PTC (n = 46);
b Follicular variant included infiltrative follicular variant (n = 10) and invasive encapsulated follicular variant (n = 6);
c Other variants included 15 Warthin-like variant, 8 diffuse sclerosing variant, 8 oncocytic variant, 5 solid variant, 3 hobnail variant, and 1 cribriform-morular variant;
d Included both microscopic and gross extrathyroidal extension.
- 1. Vaccarella S, Franceschi S, Bray F, Wild CP, Plummer M, Dal Maso L. Worldwide thyroid-cancer epidemic? The increasing impact of overdiagnosis. N Engl J Med 2016; 375: 614–7. ArticlePubMed
- 2. Ahn HS, Kim HJ, Kim KH, et al. Thyroid cancer screening in South Korea increases detection of papillary cancers with no impact on other subtypes or thyroid cancer mortality. Thyroid 2016; 26: 1535–40. ArticlePubMed
- 3. Ahn HS, Kim HJ, Welch HG. Korea's thyroid-cancer “epidemic”: screening and overdiagnosis. N Engl J Med 2014; 371: 1765–7. ArticlePubMed
- 4. Jung KW, Won YJ, Kong HJ, Lee ES. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2016. Cancer Res Treat 2019; 51: 417–30. ArticlePubMedPMCPDF
- 5. Park S, Oh CM, Cho H, et al. Association between screening and the thyroid cancer “epidemic” in South Korea: evidence from a nationwide study. BMJ 2016; 355: i5745.ArticlePubMedPMC
- 6. Jeon MJ, Kim WG, Kim TH, et al. Disease-specific mortality of differentiated thyroid cancer patients in Korea: a multicenter cohort study. Endocrinol Metab (Seoul) 2017; 32: 434–41. ArticlePubMedPMC
- 7. Lloyd RV, Osamura RY, Klöppel G, Rosai J. WHO classification of tumours of endocrine organs. 4th ed. Lyon: International Agency for Research on Cancer (IARC), 2017; 65–91.
- 8. Liu R, Bishop J, Zhu G, Zhang T, Ladenson PW, Xing M. Mortality risk stratification by combining BRAF V600E and TERT promoter mutations in papillary thyroid cancer: genetic duet of BRAF and TERT promoter mutations in thyroid cancer mortality. JAMA Oncol 2017; 3: 202–8. ArticlePubMed
- 9. Kim TH, Kim YE, Ahn S, et al. TERT promoter mutations and long-term survival in patients with thyroid cancer. Endocr Relat Cancer 2016; 23: 813–23. ArticlePubMed
- 10. Liu X, Qu S, Liu R, et al. TERT promoter mutations and their association with BRAF V600E mutation and aggressive clinicopathological characteristics of thyroid cancer. J Clin Endocrinol Metab 2014; 99: E1130–6. ArticlePubMedPMCPDF
- 11. Melo M, da Rocha AG, Vinagre J, et al. TERT promoter mutations are a major indicator of poor outcome in differentiated thyroid carcinomas. J Clin Endocrinol Metab 2014; 99: E754–65. ArticlePubMedPMCPDF
- 12. Horn S, Figl A, Rachakonda PS, et al. TERT promoter mutations in familial and sporadic melanoma. Science 2013; 339: 959–61. ArticlePubMed
- 13. Huang FW, Hodis E, Xu MJ, Kryukov GV, Chin L, Garraway LA. Highly recurrent TERT promoter mutations in human melanoma. Science 2013; 339: 957–9. ArticlePubMedPMC
- 14. Bae JS, Kim Y, Jeon S, et al. Clinical utility of TERT promoter mutations and ALK rearrangement in thyroid cancer patients with a high prevalence of the BRAF V600E mutation. Diagn Pathol 2016; 11: 21.ArticlePubMedPMC
- 15. Xing M, Liu R, Liu X, et al. BRAF V600E and TERT promoter mutations cooperatively identify the most aggressive papillary thyroid cancer with highest recurrence. J Clin Oncol 2014; 32: 2718–26. ArticlePubMedPMC
- 16. Jung CK, Kim Y, Jeon S, Jo K, Lee S, Bae JS. Clinical utility of EZH1 mutations in the diagnosis of follicular-patterned thyroid tumors. Hum Pathol 2018; 81: 9–17. ArticlePubMed
- 17. Landa I, Ganly I, Chan TA, et al. Frequent somatic TERT promoter mutations in thyroid cancer: higher prevalence in advanced forms of the disease. J Clin Endocrinol Metab 2013; 98: E1562–6. ArticlePubMedPMCPDF
- 18. Liu X, Bishop J, Shan Y, et al. Highly prevalent TERT promoter mutations in aggressive thyroid cancers. Endocr Relat Cancer 2013; 20: 603–10. ArticlePubMedPMC
- 19. Song YS, Lim JA, Choi H, et al. Prognostic effects of TERT promoter mutations are enhanced by coexistence with BRAF or RAS mutations and strengthen the risk prediction by the ATA or TNM staging system in differentiated thyroid cancer patients. Cancer 2016; 122: 1370–9. ArticlePubMed
- 20. Amin MB, Edge S, Greene F, et al. AJCC cancer staging manual. 8th ed. New York: Springer, 2017; 873–90.
- 21. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016; 26: 1–133. ArticlePubMedPMC
- 22. Jeong D, Jeong Y, Lee S, et al. Detection of BRAF(V600E) mutations in papillary thyroid carcinomas by peptide nucleic acid clamp real-time PCR: a comparison with direct sequencing. Korean J Pathol 2012; 46: 61–7. ArticlePubMedPMCPDF
- 23. Yang J, Gong Y, Yan S, Chen H, Qin S, Gong R. Association between TERT promoter mutations and clinical behaviors in differentiated thyroid carcinoma: a systematic review and meta-analysis. Endocrine 2020; 67: 44–57. ArticlePubMedPDF
- 24. de Biase D, Gandolfi G, Ragazzi M, et al. TERT promoter mutations in papillary thyroid microcarcinomas. Thyroid 2015; 25: 1013–9. ArticlePubMed
- 25. Yabuta T, Matsuse M, Hirokawa M, Yamashita S, Mitsutake N, Miyauchi A. TERT promoter mutations were not found in papillary thyroid microcarcinomas that showed disease progression on active surveillance. Thyroid 2017; 27: 1206–7. ArticlePubMed
- 26. Ma X, Gong R, Wang R, et al. Recurrent TERT promoter mutations in non-small cell lung cancers. Lung Cancer 2014; 86: 369–73. ArticlePubMed
- 27. Zhao Y, Gao Y, Chen Z, Hu X, Zhou F, He J. Low frequency of TERT promoter somatic mutation in 313 sporadic esophageal squamous cell carcinomas. Int J Cancer 2014; 134: 493–4. ArticlePubMed
- 28. Song YS, Yoo SK, Kim HH, et al. Interaction of BRAF-induced ETS factors with mutant TERT promoter in papillary thyroid cancer. Endocr Relat Cancer 2019; 26: 629–41. ArticlePubMed
References
Figure & Data
References
Citations
- Active surveillance for adult low-risk papillary thyroid microcarcinoma—a review focused on the 30-year experience of Kuma Hospital—
Yasuhiro Ito, Akira Miyauchi, Makoto Fujishima, Masashi Yamamoto, Takahiro Sasaki
Endocrine Journal.2024; 71(1): 7. CrossRef - Diagnostic utilities of washout CYFRA 21-1 combined with washout thyroglobulin for metastatic lymph nodes in thyroid cancer: a prospective study
Joonseon Park, Solji An, Kwangsoon Kim, Jeong Soo Kim, Chan Kwon Jung, Ja Seong Bae
Scientific Reports.2024;[Epub] CrossRef - 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules
Young Joo Park, Eun Kyung Lee, Young Shin Song, Soo Hwan Kang, Bon Seok Koo, Sun Wook Kim, Dong Gyu Na, Seung-Kuk Baek, So Won Oh, Min Kyoung Lee, Sang-Woo Lee, Young Ah Lee, Yong Sang Lee, Ji Ye Lee, Dong-Jun Lim, Leehi Joo, Yuh-Seog Jung, Chan Kwon Jung
International Journal of Thyroidology.2023; 16(1): 1. CrossRef - Incidence and risk factors for occult lesions in low-risk papillary thyroid microcarcinoma patients with tumor characteristics appropriate for thermal ablation: A retrospective study
Langping Jin, Kaijun Zhu, Changliang Xu, Jiaying Lu, Liming Huang
Medicine.2023; 102(38): e34938. CrossRef - Identification of NIFTP-Specific mRNA Markers for Reliable Molecular Diagnosis of Thyroid Tumors
So-Yeon Lee, Jong-Lyul Park, Kwangsoon Kim, Ja Seong Bae, Jae-Yoon Kim, Seon-Young Kim, Chan Kwon Jung
Endocrine Pathology.2023; 34(3): 311. CrossRef - Risk factors and predictive model for recurrence in papillary thyroid carcinoma: a single-center retrospective cohort study based on 955 cases
Yin Li, Jiahe Tian, Ke Jiang, Zhongyu Wang, Songbo Gao, Keyang Wei, Ankui Yang, Qiuli Li
Frontiers in Endocrinology.2023;[Epub] CrossRef - BRAFV600E Positivity-Dependent Effect of Age on Papillary Thyroid Cancer Recurrence Risk
Joonseon Park, Solji An, Kwangsoon Kim, Ja Seong Bae, Jeong Soo Kim
Cancers.2023; 15(22): 5395. CrossRef - BRAFV600E mutation test on fine‐needle aspiration specimens of thyroid nodules: Clinical correlations for 4600 patients
Huang Chen, Aiping Song, Ye Wang, Yifan He, Jie Tong, Jinxi Di, Chun Li, Zhongren Zhou, Xiaopin Cai, Dingrong Zhong, Jiping Da
Cancer Medicine.2022; 11(1): 40. CrossRef - Clinicopathological indicators for TERT promoter mutation in papillary thyroid carcinoma
Hee Young Na, Hyeong Won Yu, Woochul Kim, Jae Hoon Moon, Chang Ho Ahn, Sang Il Choi, Yeo Koon Kim, June Young Choi, So Yeon Park
Clinical Endocrinology.2022; 97(1): 106. CrossRef - A Systematic Review and Meta-analysis on the Occurrence of Biomarker Mutation in Colorectal Cancer among the Asian Population
Hafeez Afolabi, Salzihan Md Salleh, Zaidi Zakaria, Ch’ng Ewe Seng, Siti Norasikin Binti Mohd Nafil, Ahmad Aizat Bin Abdul Aziz, Yusuf Wada, Ahmad Irekeola, Syed Sameer Aga
BioMed Research International.2022; 2022: 1. CrossRef - A Significance of Concomitant BRAFV600E and TERT Mutations in Polish Patients with Papillary Thyroid Microcarcinoma: A Retrospective Cohort Study Based on 430 Cases
Artur Kuchareczko, Janusz Kopczyński, Artur Kowalik, Kinga Hińcza-Nowak, Agnieszka Walczyk, Iwona Pałyga, Tomasz Trybek, Monika Szymonek, Danuta Gąsior-Perczak, Klaudia Gadawska-Juszczyk, Estera Mikina, Izabela Płachta, Agnieszka Suligowska, Agnieszka Płu
Thyroid.2022; 32(11): 1372. CrossRef - Machine learning for identifying benign and malignant of thyroid tumors: A retrospective study of 2,423 patients
Yuan-yuan Guo, Zhi-jie Li, Chao Du, Jun Gong, Pu Liao, Jia-xing Zhang, Cong Shao
Frontiers in Public Health.2022;[Epub] CrossRef - TERT Promoter and BRAF V600E Mutations in Papillary Thyroid Cancer: A Single-Institution Experience in Korea
Min Jhi Kim, Jin Kyong Kim, Gi Jeong Kim, Sang-Wook Kang, Jandee Lee, Jong Ju Jeong, Woong Youn Chung, Daham Kim, Kee-Hyun Nam
Cancers.2022; 14(19): 4928. CrossRef - Frequency of TERT Promoter Mutations in Real-World Analysis of 2,092 Thyroid Carcinoma Patients (Endocrinol Metab 2022;37:652-63, Heera Yang et al.)
Sue Youn Kim, Chan Kwon Jung
Endocrinology and Metabolism.2022; 37(6): 947. CrossRef - Frequency of TERT Promoter Mutations in Real-World Analysis of 2,092 Thyroid Carcinoma Patients (Endocrinol Metab 2022;37:652-63, Heera Yang et al.)
Hyunju Park, Jae Hoon Chung
Endocrinology and Metabolism.2022; 37(6): 949. CrossRef - Molecular Pathology of Non-familial Follicular Epithelial–Derived Thyroid Cancer in Adults: From RAS/BRAF-like Tumor Designations to Molecular Risk Stratification
Paula Soares, Antónia Afonso Póvoa, Miguel Melo, João Vinagre, Valdemar Máximo, Catarina Eloy, José Manuel Cameselle-Teijeiro, Manuel Sobrinho-Simões
Endocrine Pathology.2021; 32(1): 44. CrossRef - Clinicopathological Characteristics and Recurrence-Free Survival of Rare Variants of Papillary Thyroid Carcinomas in Korea: A Retrospective Study
Mijin Kim, Sun Wook Cho, Young Joo Park, Hwa Young Ahn, Hee Sung Kim, Yong Joon Suh, Dughyun Choi, Bu Kyung Kim, Go Eun Yang, Il-Seok Park, Ka Hee Yi, Chan Kwon Jung, Bo Hyun Kim
Endocrinology and Metabolism.2021; 36(3): 619. CrossRef - Clinical Application of TERT Promoter Mutations in Urothelial Carcinoma
Yujiro Hayashi, Kazutoshi Fujita, George J. Netto, Norio Nonomura
Frontiers in Oncology.2021;[Epub] CrossRef - MicroRNA Profile for Diagnostic and Prognostic Biomarkers in Thyroid Cancer
Jong-Lyul Park, Seon-Kyu Kim, Sora Jeon, Chan-Kwon Jung, Yong-Sung Kim
Cancers.2021; 13(4): 632. CrossRef - Prospective Analysis of TERT Promoter Mutations in Papillary Thyroid Carcinoma at a Single Institution
Yun-Suk Choi, Seong-Woon Choi, Jin-Wook Yi
Journal of Clinical Medicine.2021; 10(10): 2179. CrossRef - Significance of telomerase reverse-transcriptase promoter mutations in differentiated thyroid cancer
Hung-Fei Lai, Chi-Yu Kuo, Shih-Ping Cheng
Formosan Journal of Surgery.2021; 54(5): 171. CrossRef - Early Diagnosis of Low-Risk Papillary Thyroid Cancer Results Rather in Overtreatment Than a Better Survival
Jolanta Krajewska, Aleksandra Kukulska, Malgorzata Oczko-Wojciechowska, Agnieszka Kotecka-Blicharz, Katarzyna Drosik-Rutowicz, Malgorzata Haras-Gil, Barbara Jarzab, Daria Handkiewicz-Junak
Frontiers in Endocrinology.2020;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-