 E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 47(2); 2013 > Article
-
Original Article
Prognostic Significance of BCL9 Expression in Hepatocellular Carcinoma - Jiyeon Hyeon, Soomin Ahn, Jae Jun Lee, Dae Hyun Song, Cheol-Keun Park
-
Korean Journal of Pathology 2013;47(2):130-136.
DOI: https://doi.org/10.4132/KoreanJPathol.2013.47.2.130
Published online: April 24, 2013
Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- Corresponding Author: Cheol-Keun Park, M.D. Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 135-710, Korea. Tel: +82-2-3410-2766, Fax: +82-2-3410-6396, 'ckpark@skku.edu'
• Received: January 2, 2013 • Revised: February 5, 2013 • Accepted: February 20, 2013
© 2013 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- BCL9 enhances β-catenin-mediated transcriptional activity regardless of the mutational status of the Wnt signaling components and increases the cell proliferation, migration, invasion, and metastatic potential of tumor cells. The goal of this study was to elucidate the prognostic significance of BCL9 protein expression in hepatocellular carcinoma (HCC) patients.
-
Methods
- We evaluated BCL9 protein expression by immunohistochemistry in tumor tissue from 288 primary HCC patients who underwent curative hepatectomy. The impact of BCL9 expression on the survival of the patients was analyzed. The median follow-up period was 97.1 months.
-
Results
- Nuclear BCL9 protein expression was observed in 74 (25.7%) of the 288 HCCs. BCL9 expression was significantly associated with younger age (p=0.038), higher Edmondson grade (p=0.001), microvascular invasion (p=0.013), and intrahepatic metastasis (p=0.017). Based on univariate analyses, BCL9 expression showed an unfavorable influence on both disease-free survival (DFS, p=0.012) and disease-specific survival (DSS, p=0.032). Multivariate analyses revealed that higher Barcelona Clinic Liver Cancer stage was an independent predictor of both shorter DFS (p<0.001) and shorter DSS (p<0.001). BCL9 expression tended to be an independent predictor of shorter DFS (p=0.078).
-
Conclusions
- BCL9 protein expression might be a marker of shorter DFS in HCC patients after curative hepatectomy.
- Patients and tissue samples
- Primary HCC tissues were collected from 288 patients who were treated with curative hepatectomy at Samsung Medical Center, Seoul, Korea from July 2000 to May 2006 (237 males and 51 females). We defined curative resection as complete resection of all tumor nodules with clear microscopic resection margins and no residual tumors as indicated by a computed tomography scan one month after surgery. The diagnosis was confirmed by histologic examination in all patients. The Institutional Review Board of Samsung Medical Center approved this study. The patients' ages ranged from 17 to 76 years with an average of 52.6. Two hundred and eighteen (75.7%) patients were infected with hepatitis B and 30 (10.4%) with hepatitis C. No viral marker was recognized in 40 (13.9%) patients. None of the patients had received preoperative chemotherapy, transarterial chemoembolization, or radiofrequency ablation. Tumor differentiation was graded histologically according to the criteria of Edmondson and Steiner.13 Microvascular invasion was considered present when at least one or more endothelial cells or the tunica media of the vessel surrounded a neoplastic cell group. Intrahepatic metastasis and multicentric occurrence were defined according to the previously reported criteria.14 Briefly, intrahepatic metastasis is defined as: 1) portal vein tumor thrombi or cancer lesions that have putatively proliferated from a tumor thrombus, 2) groups of cancer lesions that are most abundant adjacent to the largest main lesion and decrease in number with distance from the main lesion, or 3) small solitary cancer lesions located adjacent to the largest main lesion and of the same histological type that are definitely smaller than the main tumor and differentiated to the same degree or less differentiated than the main lesion. Multicentric occurrence is defined as: 1) adenomatous hyperplasia or early HCCs that preserve the existing liver architecture, 2) well differentiated HCCs found at the edge of moderately or poorly differentiated cancer tissues, or 3) multiple HCC lesions that cannot be classified as metastasis based on the above criteria. Tumor stage was determined according to both the American Joint Committee on Cancer (AJCC)15 and the Barcelona Clinic Liver Cancer (BCLC) staging classification.16
- Patients were followed by monitoring serum α-fetoprotein levels and three phase dynamic computed tomography scans every three months after surgery. Magnetic resonance imaging was used in order to confirm tumor recurrence in suspected cases. The median follow-up period was 97.1 months (range, 40 to 126 months). Disease-free survival (DFS) was defined from the date of resection until the detection of tumor recurrence. We chose HCC-related mortality (disease-specific death) as the clinical endpoint for survival analysis, defined by Hoshida et al.17 as: 1) tumor occupying more than 80% of the liver, 2) portal venous tumor thrombus proximal to the second bifurcation, 3) obstructive jaundice due to the tumor, 4) distant metastases, or 5) variceal hemorrhage with portal venous tumor thrombus proximal to the first bifurcation. Disease-specific survival (DSS) was defined from the date of resection to HCC-related death. Tumor recurrence was detected in 189 (65.6%) patients and 99 (34.4%) patients died of HCC. Thirty of the 129 deaths in this study were due to non-HCC causes.
- Tissues with dysplastic nodule (DN), which is a precancerous lesion of HCC (n=28), were included and DNs were subdivided into low-grade DN and high-grade DN according to the guideline of the International Working Party.18
- Histologic sections were examined by two pathologists and representative tumor regions free from necrosis or hemorrhage were marked in formalin-fixed paraffin-embedded blocks. Two 2.0 mm-diameter tissue cores were punched from the marked areas of each block and arranged in recipient paraffin blocks. Two cores of normal liver tissue from 12 patients with metastatic colonic carcinoma of the liver were included in each array block.
- Immunohistochemical analysis
- Immunohistochemical staining was performed as described elsewhere.19 Antigen retrieval was performed with 0.01 mol/L citrate buffer (pH 6.0) for 30 minutes in a pressure cooker. The sections were incubated overnight at 4℃ with the rabbit polyclonal antibody to BCL9 (ab37305, 1:100, Abcam Inc., Cambridge, MA, USA). The positive control (human colon carcinoma) showed intense nuclear BCL9 expression in cancer cells while no immunoreactivity was observed in the tissue sections used as negative controls, in which the primary antibody was replaced by preimmune rabbit serum. In order to validate the concordance between the tissue microarrays and whole tumor sections, we also detected BCL9 expression for 40 corresponding whole tumor sections randomly chosen from the 288 cases.
- Immunohistochemical staining was assessed by two independent pathologists (C.K.Park and J.Hyeon) without knowledge of the patients' characteristics and any discrepancies were resolved by consensus. The sections were scored by combining the proportion and intensity of the stained tumor cells as reported previously.9 The proportion of stained tumor cells was determined semi-quantitatively and each sample was scored on a scale of 0-3 (0, <5%; 1, 5-30%; 2, 31-60%; 3, 61-100%). The staining intensity was classified as 0 (negative), 1 (weak), 2 (moderate), and 3 (strong). The immunoreactive score of each tumor was calculated by multiplication of the scores of the proportion of stained cells and the staining intensity. Duplicate tissue cores for each tumor showed high levels of homogeneity for both the proportion of stained cells and the staining intensity. When there were differences between the duplicate tissue cores, the higher score was taken as the total score.
- Statistical analysis
- Statistical analyses were performed using SPSS software (SPSS Inc., Chicago, IL, USA). The chi-square test and Fisher's exact test were used for comparison of the variables. Cumulative survival time was calculated by the Kaplan-Meier method and compared by the log-rank test. Univariate and multivariate analyses were based on the Cox proportional hazards regression model. p-values less than 0.05 were considered statistically significant.
MATERIALS AND METHODS
- BCL9 protein expression in HCC
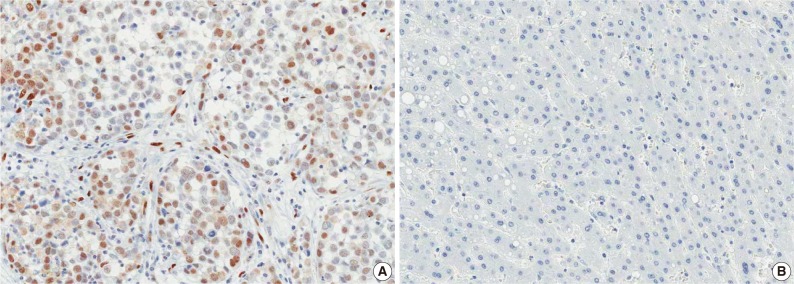
- BCL9 was detected on the cytoplasm in 3-10% of the normal hepatocytes with weak or moderate staining intensity. In HCC, immunoreactivity for BCL9 was observed in the nuclei of tumor cells with or without cytoplasmic expression. We regarded BCL9 as positive when the total score for nuclear immunoreactivity was 1-9. BCL9 protein expression was observed in 74 (25.7%) of the 288 HCCs (Fig. 1A). BCL9 expression was significantly associated with younger age (p=0.038), higher Edmondson grade (p=0.001), microvascular invasion (p=0.013), and intrahepatic metastasis (p=0.017) (Table 1). None of the 28 DNs showed nuclear immunoreactivity for BCL9 (Fig. 1B).
- Tumor recurrence was significantly associated with larger tumor size (p=0.011), higher Edmondson grade (p=0.029), microvascular invasion (p=0.001), major portal vein invasion (p=0.038), intrahepatic metastasis (p<0.001), higher AJCC T stage (p<0.001), higher BCLC stage (p=0.004), higher α-fetoprotein level (p=0.002), viral etiology (p=0.004), and liver cirrhosis (p=0.009) (Table 1).
- Survival analysis
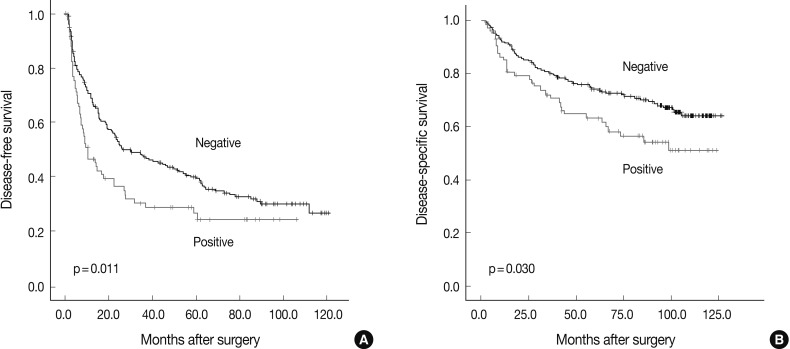
- The DFS and DSS rates for the 288 HCC patients were 42.7% and 78.2% at three years, 36.3% and 71.4% at five years, 30.1% and 67.1% at seven years, and 27.9% and 60.8% at nine years, respectively. Based on univariate analyses, larger tumor size, Edmondson grade III, microvascular invasion, major portal vein invasion, intrahepatic metastasis, higher AJCC T stage, higher BCLC stage, lower albumin level, and higher α-fetoprotein level showed unfavorable influence on both DFS and DSS. Viral etiology and liver cirrhosis showed unfavorable influence on DFS. BCL9 expression showed an unfavorable influence on both DFS (p=0.012) and DSS (p=0.032) (Table 2). The five-year DFS rate of the BCL9-positive group was significantly lower than that of the BCL9-negative group (24.2% vs 39.2%) (Fig. 2A). The median DFS of the BCL9-positive group and the BCL9-negative group were 9.9 and 23.8 months, respectively. The five-year DSS rate of the BCL9-positive group was significantly lower than that of the BCL9-negative group (61.7% vs 73.6%) (Fig. 2B). The median DSS of the BCL9-positive group and the BCL9-negative group were 63.1 and 86.5 months, respectively.
- Since tumor size, vascular invasion, intrahepatic metastasis, AJCC stage, and serum albumin level were associated with BCLC stage, we did not perform multiple analyses with these indices in order to avoid potential bias. An evaluation of the significant weight of the serum α-fetoprotein level was not performed due to missing data (n=277). Based on multivariate analyses, higher BCLC stage (p<0.001), viral etiology (p=0.022), and liver cirrhosis (p=0.011) were independent predictors of shorter DFS. BCL9 expression tended to be an independent predictor of shorter DFS (p=0.078). BCL9-positive patients were more likely to suffer from recurrence than BCL9-negative patients (hazard ratio=1.351, 95% confidence interval 0.967-1.888). Higher BCLC stage (p<0.001) was an independent predictor of shorter DSS. However, BCL9 expression was not an independent predictor of DSS (p=0.115) (Table 3).
RESULTS
- BCL9 is required for Wnt signal transduction at the level of nuclear β-catenin and to exert its function by physically linking pygopus to β-catenin.5 Kramps et al.5 reported that wild-type cells expressed BCL9/legless protein in the nuclei and the nuclear localization of the BCL9/legless appeared to be essential for its signaling activity. Recent reports showed that nuclear BCL9 staining was absent in human normal colon mucosa, but elevated in human colorectal cancer.8,9 In this study, nuclear immunoreactivity for BCL9 was not observed in normal liver or DN tissues. BCL9 protein expression might not be an early event in HCC carcinogenesis. Recent studies have shown that the BCL9-2 protein was significantly up-regulated in human colon adenomas compared with normal colon mucosa,9 which suggests that the deregulation of BCL9 occurs during early stages of colonic carcinogenesis. In colorectal cancer patients, almost all cases showed high BCL9-2 protein expression and it was not correlated with overall survival, indicating that BCL9-2 is not a predictor for advanced tumor stages in colorectal cancer.9
- In the current study, we applied tissue microarrays in order to evaluate the prognostic significance of BCL9 protein expression in a large cohort of HCC patients and demonstrated that BCL9 expression was correlated with higher Edmondson grade, microvascular invasion, and intrahepatic metastasis, which suggest the involvement of BCL9 in the pathogenesis of HCC. Tumor recurrence was remarkably associated (p<0.005) with microvascular invasion, intrahepatic metastasis, higher AJCC T stage, higher BCLC stage, higher α-fetoprotein level, and viral etiology. In addition, HCC with BCL9 expression had a lower five-year DFS rate than HCC without BCL9 expression and BCL9 expression tended to be an independent predictor of shorter DFS. HCC with BCL9 expression had a lower five-year DSS rate than HCC without BCL9 expression. These findings indicate that BCL9 is a potential new marker of shorter DFS in HCC after curative resection and the results could help clinicians identify patients at high risk of recurrence.
- This study demonstrates, for the first time, that BCL9 protein expression in HCC tissues might be a marker of shorter DFS in HCC after curative hepatectomy in a large number of HCC patients with long-term follow-up. Patients identified as being at high risk of recurrence should be followed closely. Further study is needed in order to examine the mechanism of the actions regarding BCL9 protein expression in HCC prognosis.
DISCUSSION
- 1. Poon RT. Prevention of recurrence after resection of hepatocellular carcinoma: a daunting challenge. Hepatology 2011; 54: 757–759. PMID: 21793027. ArticlePubMed
- 2. Llovet JM, Schwartz M, Mazzaferro V. Resection and liver transplantation for hepatocellular carcinoma. Semin Liver Dis 2005; 25: 181–200. PMID: 15918147. ArticlePubMed
- 3. Qin LX, Tang ZY. Recent progress in predictive biomarkers for metastatic recurrence of human hepatocellular carcinoma: a review of the literature. J Cancer Res Clin Oncol 2004; 130: 497–513. PMID: 15205947. ArticlePubMed
- 4. Willis TG, Zalcberg IR, Coignet LJ, et al. Molecular cloning of translocation t(1;14)(q21;q32) defines a novel gene (BCL9) at chromosome 1q21. Blood 1998; 91: 1873–1881. PMID: 9490669. ArticlePubMedPDF
- 5. Kramps T, Peter O, Brunner E, et al. Wnt/wingless signaling requires BCL9/legless-mediated recruitment of pygopus to the nuclear beta-catenin-TCF complex. Cell 2002; 109: 47–60. PMID: 11955446. ArticlePubMed
- 6. Polakis P. Wnt signaling and cancer. Genes Dev 2000; 14: 1837–1851. PMID: 10921899. ArticlePubMed
- 7. Morin PJ, Sparks AB, Korinek V, et al. Activation of beta-catenin-Tcf signaling in colon cancer by mutations in beta-catenin or APC. Science 1997; 275: 1787–1790. PMID: 9065402. ArticlePubMed
- 8. Mani M, Carrasco DE, Zhang Y, et al. BCL9 promotes tumor progression by conferring enhanced proliferative, metastatic, and angiogenic properties to cancer cells. Cancer Res 2009; 69: 7577–7586. PMID: 19738061. ArticlePubMedPMC
- 9. Brembeck FH, Wiese M, Zatula N, et al. BCL9-2 promotes early stages of intestinal tumor progression. Gastroenterology 2011; 141: 1359–1370. PMID: 21703997. ArticlePubMed
- 10. Kim TM, Yim SH, Shin SH, et al. Clinical implication of recurrent copy number alterations in hepatocellular carcinoma and putative oncogenes in recurrent gains on 1q. Int J Cancer 2008; 123: 2808–2815. PMID: 18803288. ArticlePubMedPMC
- 11. Moinzadeh P, Breuhahn K, Stützer H, Schirmacher P. Chromosome alterations in human hepatocellular carcinomas correlate with aetiology and histological grade: results of an explorative CGH meta-analysis. Br J Cancer 2005; 92: 935–941. PMID: 15756261. ArticlePubMedPMC
- 12. Wong N, Lai P, Lee SW, et al. Assessment of genetic changes in hepatocellular carcinoma by comparative genomic hybridization analysis: relationship to disease stage, tumor size, and cirrhosis. Am J Pathol 1999; 154: 37–43. PMID: 9916916. ArticlePubMedPMC
- 13. Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer 1954; 7: 462–503. PMID: 13160935. ArticlePubMed
- 14. Liver Cancer Study Group of Japan. General rules for the clinical and pathological study of primary liver cancer. 2003; 2nd ed. Tokyo: Kanehara, 38.
- 15. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A 3rd. AJCC cancer staging manual. 2010; 7th ed. Chicago: Springer.
- 16. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis 1999; 19: 329–338. PMID: 10518312. ArticlePubMed
- 17. Hoshida Y, Villanueva A, Kobayashi M, et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N Engl J Med 2008; 359: 1995–2004. PMID: 18923165. ArticlePubMedPMC
- 18. International Working Party. Terminology of nodular hepatocellular lesions. Hepatology 1995; 22: 983–993. PMID: 7657307. ArticlePubMed
- 19. Kim SH, Ahn S, Park CK. Smad3 and its phosphoisoforms are prognostic predictors of hepatocellular carcinoma after curative hepatectomy. Hepatobiliary Pancreat Dis Int 2012; 11: 51–59. PMID: 22251470. ArticlePubMed
References
Fig. 1Immunostaining of BCL9 showing nuclear expression in hepatocellular carcinoma (A) and no nuclear expression in dysplastic nodule (B) (horseradish peroxidase stain).
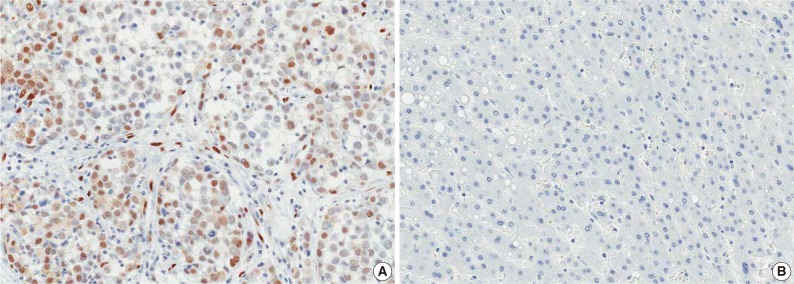
Fig. 2Kaplan-Meier survival curves showing disease-free survival (A) and disease-specific survival (B) for BCL9 expression in 288 hepatocellular carcinomas.
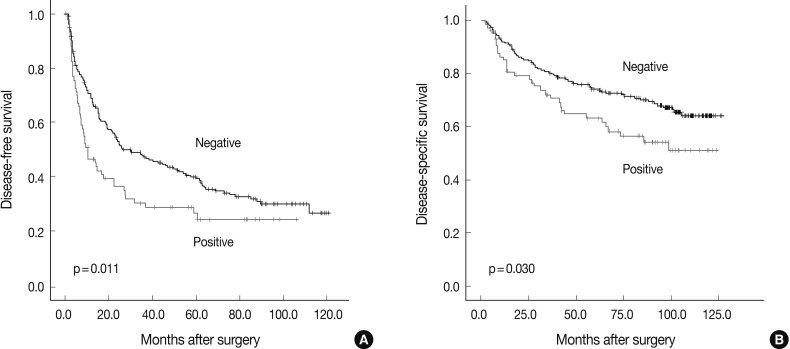
Table 1.Correlation of BCL9 expression and tumor recurrence with clinicopathologic features in 288 hepatocellular carcinomas
Table 2.Univariate analyses of disease-free survival and disease-specific survival in 288 hepatocellular carcinomas
Table 3.Multivariate analyses of disease-free survival and disease-specific survival in 288 hepatocellular carcinomas
Figure & Data
References
Citations
Citations to this article as recorded by 
- The Wnt-dependent and Wnt-independent functions of BCL9 in development, tumorigenesis, and immunity: Implications in therapeutic opportunities
Minjie Wu, Heng Dong, Chao Xu, Mengqing Sun, Haojin Gao, Fangtian Bu, Jianxiang Chen
Genes & Diseases.2024; 11(2): 701. CrossRef - The role of BCL9 genetic variation as a biomarker for hepatitis C-related hepatocellular carcinoma in Egyptian patients
Eman Abd El Razek Abbas, Ahmed Barakat Barakat, Mohamed Hassany, Samar Samir Youssef
Journal of Genetic Engineering and Biotechnology.2022; 20(1): 4. CrossRef - Molecular Targets and Signaling Pathways of microRNA-122 in Hepatocellular Carcinoma
Kwang-Hoon Chun
Pharmaceutics.2022; 14(7): 1380. CrossRef - Wnt/β-Catenin Signalling and Its Cofactor BCL9L Have an Oncogenic Effect in Bladder Cancer Cells
Roland Kotolloshi, Mieczyslaw Gajda, Marc-Oliver Grimm, Daniel Steinbach
International Journal of Molecular Sciences.2022; 23(10): 5319. CrossRef - Bcl9 Depletion Modulates Endothelial Cell in Tumor Immune Microenvironment in Colorectal Cancer Tumor
Zhuang Wei, Mei Feng, Zhongen Wu, Shuru Shen, Di Zhu
Frontiers in Oncology.2021;[Epub] CrossRef - Wnt Signaling Pathway Is among the Drivers of Liver Metastasis
Ivana Samaržija
Livers.2021; 1(4): 180. CrossRef - Nuclear Expression of Pygo2 Correlates with Poorly Differentiated State Involving c-Myc, PCNA and Bcl9 in Myanmar Hepatocellular Carcinoma
Myo Win Htun, Yasuaki Shibata, Kyaw Soe, Takehiko Koji
ACTA HISTOCHEMICA ET CYTOCHEMICA.2021; 54(6): 195. CrossRef - Wnt status-dependent oncogenic role of BCL9 and BCL9L in hepatocellular carcinoma
Nicole Huge, Maria Sandbothe, Anna K. Schröder, Amelie Stalke, Marlies Eilers, Vera Schäffer, Brigitte Schlegelberger, Thomas Illig, Beate Vajen, Britta Skawran
Hepatology International.2020; 14(3): 373. CrossRef - Structure and function of Pygo in organ development dependent and independent Wnt signalling
Yan Shi, Xiushan Wu, Shuoji Zhu, Huanlei Huang, Jian Zhuang, Haiyun Yuan, Wuzhou Yuan, Ping Zhu
Biochemical Society Transactions.2020; 48(4): 1781. CrossRef - BCL9/BCL9L in hepatocellular carcinoma: will it or Wnt it be the next therapeutic target?
Akshata Moghe, Satdarshan P. Monga
Hepatology International.2020; 14(4): 460. CrossRef - Loss of BCL9/9l suppresses Wnt driven tumourigenesis in models that recapitulate human cancer
David M. Gay, Rachel A. Ridgway, Miryam Müller, Michael C. Hodder, Ann Hedley, William Clark, Joshua D. Leach, Rene Jackstadt, Colin Nixon, David J. Huels, Andrew D. Campbell, Thomas G. Bird, Owen J. Sansom
Nature Communications.2019;[Epub] CrossRef - Immunohistochemical Mapping of Bcl9 Using Two Antibodies that Recognize Different Epitopes Is Useful to Characterize Juvenile Development of Hepatocellular Carcinoma in Myanmar
Myat Thu Soe, Yasuaki Shibata, Myo Win Htun, Kuniko Abe, Kyaw Soe, Nay Win Than, Thann Lwin, Myat Phone Kyaw, Takehiko Koji
ACTA HISTOCHEMICA ET CYTOCHEMICA.2019; 52(1): 9. CrossRef - Low BCL9 expression inhibited ovarian epithelial malignant tumor progression by decreasing proliferation, migration, and increasing apoptosis to cancer cells
Jing Wang, Mingjun Zheng, Liancheng Zhu, Lu Deng, Xiao Li, Linging Gao, Caixia Wang, Huimin Wang, Juanjuan Liu, Bei Lin
Cancer Cell International.2019;[Epub] CrossRef - SOX7 Suppresses Wnt Signaling by Disrupting β-Catenin/BCL9 Interaction
Rong Fan, HaiYan He, Wang Yao, YanFeng Zhu, XunJie Zhou, MingTai Gui, Jing Lu, Hao Xi, ZhongLong Deng, Min Fan
DNA and Cell Biology.2018; 37(2): 126. CrossRef - Hypoxia activates Wnt/β-catenin signaling by regulating the expression of BCL9 in human hepatocellular carcinoma
Wei Xu, Wang Zhou, Mo Cheng, Jing Wang, Zhian Liu, Shaohui He, Xiangji Luo, Wending Huang, Tianrui Chen, Wangjun Yan, Jianru Xiao
Scientific Reports.2017;[Epub] CrossRef - Hepatocellular carcinoma biology predicts survival outcome after liver transplantation in the USA
Mohamed Abd El-Fattah
Indian Journal of Gastroenterology.2017; 36(2): 117. CrossRef - miR-30a acts as a tumor suppressor by double-targeting COX-2 and BCL9 in H. pylori gastric cancer models
Xuan Liu, Qing Ji, Chengcheng Zhang, Xiaowei Liu, Yanna Liu, Ningning Liu, Hua Sui, Lihong Zhou, Songpo Wang, Qi Li
Scientific Reports.2017;[Epub] CrossRef - BCL9, a coactivator for Wnt/β-catenin transcription, is targeted by miR-30c and is associated with prostate cancer progression
XIAO-HUI LING, ZHI-YUN CHEN, HONG-WEI LUO, ZE-ZHEN LIU, YING-KE LIANG, GUAN-XING CHEN, FU-NENG JIANG, WEI-DE ZHONG
Oncology Letters.2016; 11(3): 2001. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
- Related articles

