E-submission
E-submission
Articles
- Page Path
- HOME > J Pathol Transl Med > Volume 46(3); 2012 > Article
-
Case Report
Papillary Carcinoma of Thyroid Metastatic to AdenocarcinomaIn Situ of Lung: Report of an Unusual Case - Kyoung Min Kim, Yo Na Kim, Hyun Hee Chu, Heung Yong Jin1, Min Ho Kim2, Myoung Ja Chung
-
Korean Journal of Pathology 2012;46(3):282-286.
DOI: https://doi.org/10.4132/KoreanJPathol.2012.46.3.282
Published online: June 22, 2012
Department of Pathology, Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea.
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea.
2Department of Thoracic and Cardiovascular Surgery, Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea.
- Corresponding Author: Myoung Ja Chung, M.D. Department of Pathology, Chonbuk National University Medical School, 567 Baekje-daero, Deokjin-gu, Jeonju 561-756, Korea. Tel: +82-63-270-3072, Fax: +82-63-270-3135, 'mjchung@jbnu.ac.kr'
© 2012 The Korean Society of Pathologists/The Korean Society for Cytopathology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
- The tumor-to-tumor metastasis is a rare event. The lung tumors are the most common donor tumors in tumor-to-tumor metastasis, but are exceedingly rare as a recipient. Here, we report a case of papillary thyroid carcinoma (PTC) metastasizing to adenocarcinoma in situ (AIS, formerly bronchioloalveolar carcinoma) of the lung in a 44-year-old woman who underwent total thyroidectomy for PTC 8 years ago. To the best of our knowledge, the present case is the first case reporting on PTC metastasized to AIS. A review of the relevant literature is presented.
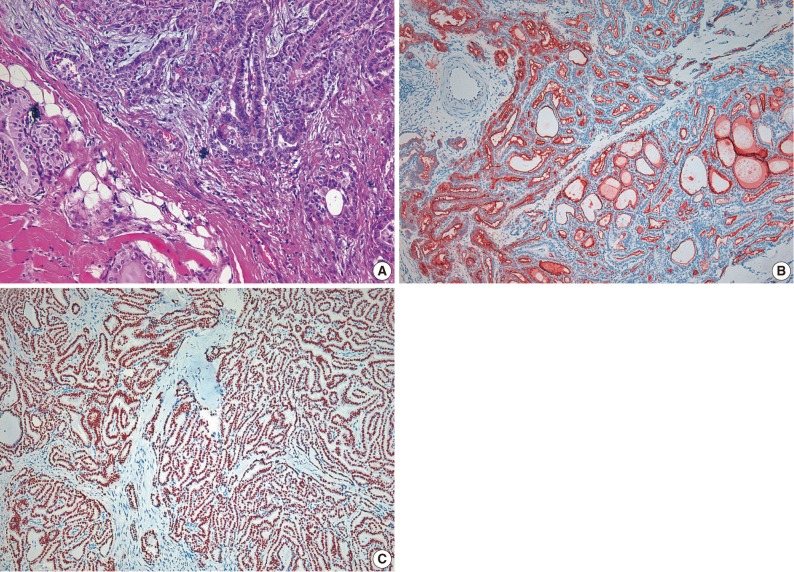
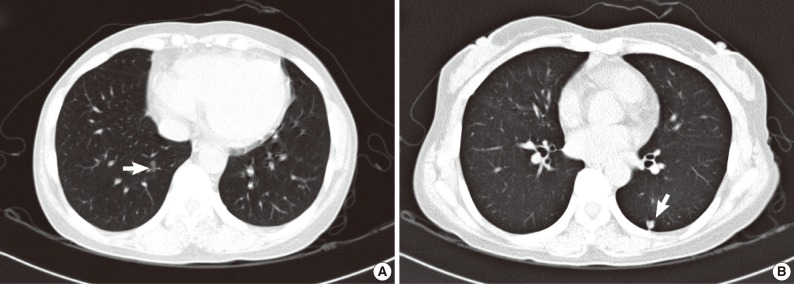
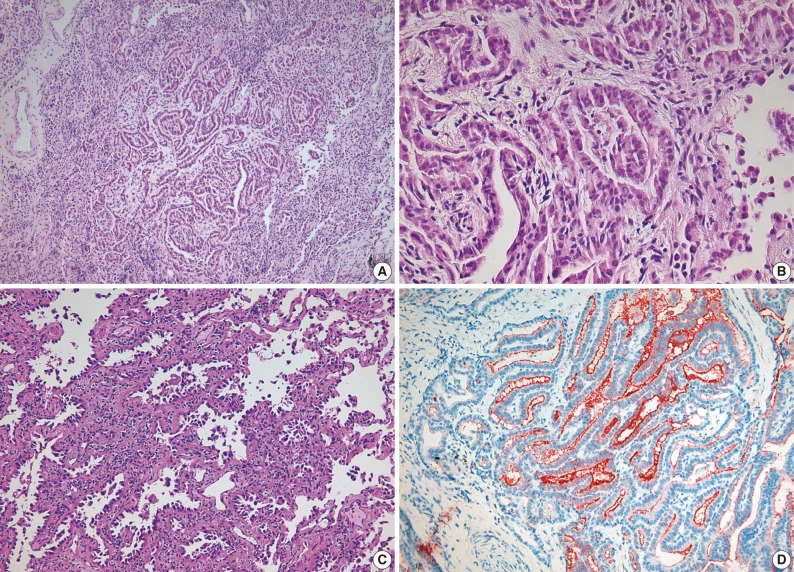
- A 44-year-old woman was admitted to the hospital for evaluation of pulmonary nodule detected on computed tomography (CT). She had a history of total thyroidectomy for PTC, which was performed 8 years ago. The primary PTC measured 2.4×1.3 cm in dimension with invasion into adjacent muscle and had metastasized to several regional lymph nodes (pT4N1) (Fig. 1). After total thyroidectomy the patient had taken neck and chest CT scan at an interval of one year. The PTC recurred in the cervical lymph node after 2 years of total thyroidectomy. There was no evidence of lung metastasis. A follow-up CT scan taken after postoperative 6 years demonstrated the presence of two nodules in both the lower lobes of lungs. Both the nodules were 0.6 cm in the longest diameter. At the 2 years follow-up CT scan after detection of the pulmonary nodules, there was a slight increase in the size of right lobe nodule from 0.6 to 0.8 cm (Fig. 2). Consequently, the patient underwent wedge resections of both lobes. The resected right lower lobe measured 5.8×3.3 cm in dimension and it contained a small nodule measuring 0.8×0.5 cm in dimension. Microscopically, the main part of the nodule showed typical histologic features of nonmucinous AIS. Single layer of cuboidal cells grew along the thick-ened alveolar walls in a lepidic pattern. There was no stromal or vascular invasion. Within the AIS area, there was a 0.2×0.1 cm sized lesion, which exhibited papillary structures with typical nuclear features of PTC. The papillary carcinoma was composed of enlarged cells with clear nuclei and occasional intranuclear inclusions (Fig. 3). In addition, multiple microscopic foci of metastatic PTC were also observed in the surrounding normal lung tissue. Immunohistochemical staining for thyroid transcription factor-1 (TTF-1) and thyroglobulin was performed on both thyroid and lung tumor. Immunohistochemically, PTC of the thyroid gland was positive for both thyroglobulin and TTF-1. The tumor cells of the AIS of the lung showed immunoreactivity for TTF-1 antibody but were negative for thyroglobulin. The tumor cells in the papillary carcinoma in the AIS displayed diffuse positivity for thyroglobulin (Fig. 3). These findings were consistent with AIS involved with metastatic PTC. The nodule in the left lung was identified to be chondroid harmatoma. After 11 months of lung resection, no newly developed lesion was observed in the lung. The patient remains still alive.
CASE REPORT
- We report herein an unusual occurrence of PTC metastasizing to AIS of the lung. The lung is one of the most frequent site of metastasis in the case of extrathoracic cancers. This phenomenon can be explained in terms of presence of certain features like: 1) they continuosly receive the entire right-sided cardiac output with every heartbeat; 2) they are the first capillary plexus met by cells after most of the lymphatic drainage enters the venous system; and 3) they consist of delicate membranes that may be beneficial for initially drawing on nearby oxygenated air for early sustenance.8 However, lung carcinoma is one of the rarest recipients for tumor-to-tumor metastasis. RCC is the most common recipient tumor in tumor-to-tumor metastasis.5 The reason for the relatively high incidence of RCC as a recipient for tumor-to-tumor metastases remains unclear. However, two major mechanisms have been considered to account for the possible explanations for this observed behavior. One is the rich regular network of thin-walled blood vessels of RCC, which renders them more accessible to metastatic tumor cells in the circulating blood, and the other is the high lipid and glycogen content in RCC, which may provide a nutrient-rich microenvironment for the growth of metastatic tumor cells.9,10 Based on the above explanations, presence of different vascular structures between normal lung and lung cancer may be the possible reason for the different potential as a site of metastasis. Unlike normal lung, lung cancer doesn't contain a rich network of small thin-walled blood vessels. The other possible explanation which we considered was that lung cancer is rapidly growing tumor therefore it cannot provide a suitable environment for the acceptance of metastasis. Regarding the reason for the relatively high incidence of lung cancer as a donor in tumor-to-tumor metastasis, Horie and Nomura11 proposed that the rich vascularity of lung carcinoma in association with the probable shedding of tumor cells during respiratory movement might increase the frequency of invasion into the pulmonary vein and subsequently into the general circulation. The tumor emboli from lung cancer have a better chance to reach all the body organs through the left-sided cardiac output than cancers of the other organs.
- Despite the incidence of multiple primary malignant tumors being between 4.2 to 8%, the occurrence of tumor-to-tumor metastasis is extremely rare. Regarding the reason for the rarity of these occurrences, Rabson et al.2 suggested that neoplasms produce substances, which are locally antagonistic to the other new growth. Kikuchi et al.12 considered the biological differences between cancer cells and normal ones and experimentally confirmed the antigenic difference between their membranous structures.5 Furthermore, the nutritional requirement of a rapidly growing tumor may be extensive to the point where a nutritive competitive cellular growth ensues.13,14
- It is still unexplained whether tumor-to-tumor metastasis is merely of a chance occurrence or is a selective growth within the recipient tumor. Our case showed that the metastatic PTC foci were not limited to the AIS and multiple microscopic foci of PTC were observed in the surrounding normal lung tissue. Tumors that have metastasized to the other tumors are generally widely disseminated in the other regions of the body. Till date, no specific type of tumor with a predilection to metastasize to other tumors has been identified. Together, we suggest that our case of tumor-to-tumor metastasis is an incidental condition rather than a specific selective growth.
- Such a combination of tumor-to-tumor metastasis (PTC within AIS) should be differentiated from primary mixed adenocarcinoma, which is composed of AIS and papillary adenocarcinoma of lung. Awareness about this phenomenon of tumor-to-tumor metastasis and proper immunohistochemical staining such as thyroglobulin are important for correct diagnosis.
- Disease-specific survival of PTC patients with distant metastases at 5 and 10 years was reported to be 65 and 45%, respectively.15 However, if the distant metastases was confined to the lung with small-sized nodule, it showed relatively favorable outcomes.15
- In summary, we report a rare case of tumor-to-tumor metastasis to AIS of the lung. We believe that rich network of thin-walled blood vessels, good circulation, and less aggressiveness of recipient tumor than donor tumor may be the associated conditions in recipient tumor in tumor-to-tumor metastasis.
DISCUSSION
- 1. Ross JS, Leitner DW. Carcinoid with carcinoma: a case of tumor-to-tumor metastasis. Arch Pathol Lab Med 1981; 105: 558–559. PMID: 6895174. PubMed
- 2. Rabson SM, Stier PL, Baumgartner JC, Rosenbaum D. Metastasis of cancer to cancer. Am J Clin Pathol 1954; 24: 572–579. PMID: 13158286. PubMed
- 3. Singh EO, Benson RC Jr, Wold LE. Cancer-to-cancer metastasis. J Urol 1984; 132: 340–342. PMID: 6737593. PubMed
- 4. Campbell LV Jr, Gilbert E, Chamberlain CR Jr, Watne AL. Metastases of cancer to cancer. Cancer 1968; 22: 635–643. PMID: 5673241. ArticlePubMed
- 5. Petraki C, Vaslamatzis M, Argyrakos T, et al. Tumor to tumor metastasis: report of two cases and review of the literature. Int J Surg Pathol 2003; 11: 127–135. PMID: 12754635. ArticlePubMed
- 6. Roscoe KJ, Raja S, Tronic B, Dou Y. Single F-18 fluorodeoxyglucose positron emission tomography hypermetabolic focus containing metastatic papillary thyroid cancer within a primary scarring adenocarcinoma lung cancer. Clin Nucl Med 2006; 31: 359–360. PMID: 16714903. ArticlePubMed
- 7. Nonomura A, Mizukami Y, Shimizu J, Watanabe Y, Kamimura R, Takashima T. Two patients with metastasis of cancer to other neoplasm: a thyroid carcinoma metastatic to a lung carcinoma and a gastric carcinoma metastatic to a thyroid adenoma. Endocr Pathol 1994; 5: 233–239. Article
- 8. Dail DH. In : Tomashefski JF Jr, Cagle PT, Farver CF, Fraire AE, eds. Metastases to and from the lung. Dail and Hammar's pulmonary pathology. 2008; 3rd ed. New York: Springer, 735–766. Article
- 9. Dobbing J. Cancer to cancer. Guys Hosp Rep 1958; 107: 60–65. PMID: 13524722. PubMed
- 10. Ortega P Jr, Li IY, Shimkin M. Metastasis of neoplasms to other neoplasms. Ann West Med Surg 1951; 5: 601–609. PMID: 14857652. PubMed
- 11. Horie N, Nomura Y. Synchronous triple cancers with cancer to cancer metastasis. Jpn J Cancer Clin 1977; 23: 557–560.
- 12. Kikuchi K, Tsuji Y, Itakura K, Katagiri H. A case of metastases of gastric cancer to hypernephroma and its metastatic foci. Acta Pathol Jpn 1964; 14: 103–110. PMID: 14196551. Article
- 13. Gore I, Barr R. Metastasis of cancer to cancer. AMA Arch Pathol 1958; 66: 293–298. PMID: 13570810. PubMed
- 14. Maloney JD, Immergut M. The kidney as host in cancer-to-cancer metastasis. J Urol 1967; 98: 657–660. PMID: 6080044. PubMed
- 15. Sugitani I, Fujimoto Y, Yamamoto N. Papillary thyroid carcinoma with distant metastases: survival predictors and the importance of local control. Surgery 2008; 143: 35–42. PMID: 18154931. ArticlePubMed
References
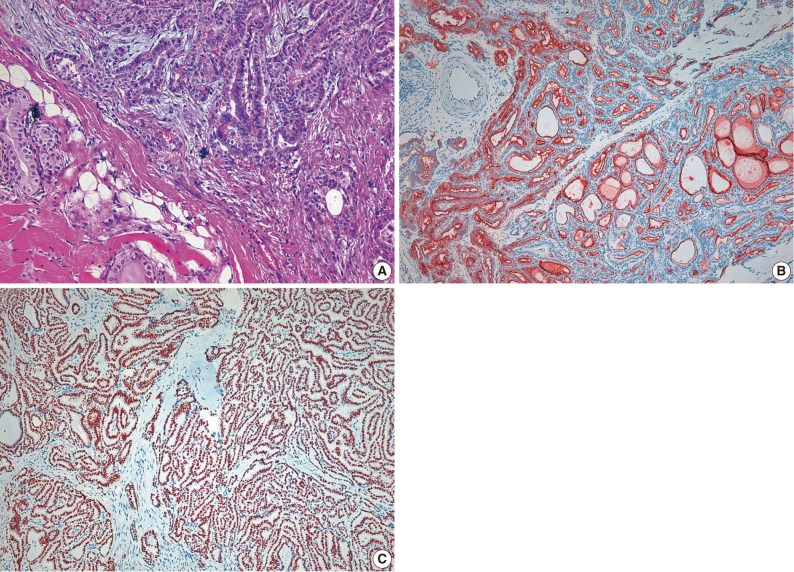
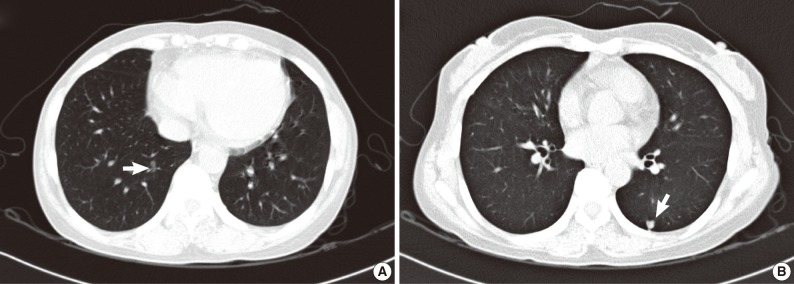
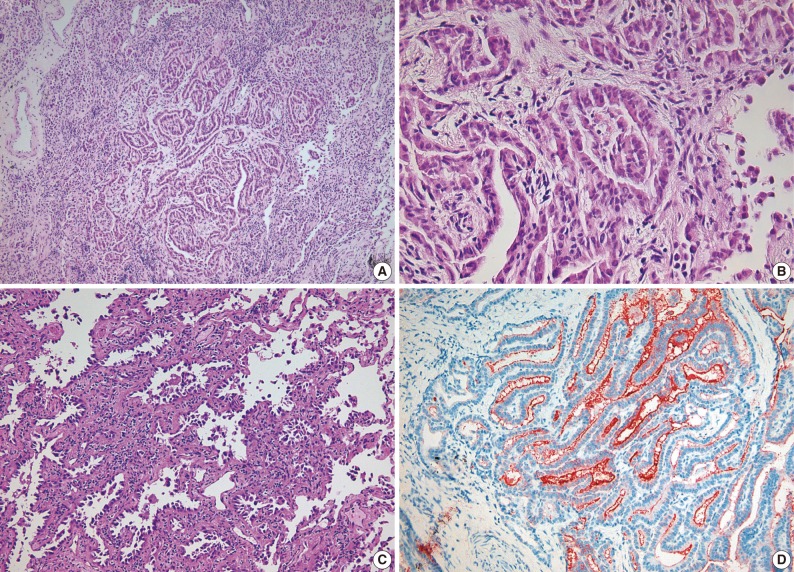
Figure & Data
References
Citations
- A case of colorectal cancer with intratumoral metastasis to primary lung cancer
Yasushi Cho, Mitsuhito Kaji, Shunsuke Nomura, Yusuke Motohashi, Masaaki Sato, Motoya Takeuchi
The Journal of the Japanese Association for Chest Surgery.2021; 35(5): 576. CrossRef - Tumor-to-tumor metastasis: metastatic invasive lobular carcinoma of the breast within adenocarcinoma of the lung
Myoung Jae Kang, Ae Ri An, Myoung Ja Chung, Kyoung Min Kim
Journal of Pathology and Translational Medicine.2020; 54(2): 188. CrossRef - Metastatic Renal Cell Neoplasm Within a Papillary Thyroid
Carcinoma as Incidental Finding in an Asymptomatic Patient: a Case Report
Maria-Rosa Bella-Cueto, Mireia Pascua-Solé, Albert Cano-Palomares, M. Àngels Cabezuelo-Hernandez, Maria-Rosa Escoda-Giralt, Santiago Barcons-Vilaplana, Paula Serret-Miralles, Carmen Caral-Vanaclocha, Xavier Guirao-Garriga, Joan Prats-Lopez, Meritxell Meda
SN Comprehensive Clinical Medicine.2020; 2(7): 978. CrossRef - A Rare Case of Tumor-to-Tumor Metastasis of Thyroid Papillary Carcinoma within a Pulmonary Adenocarcinoma
Taebum Lee, Yoon Jin Cha, Sangjeong Ahn, Joungho Han, Young Mog Shim
Journal of Pathology and Translational Medicine.2015; 49(1): 78. CrossRef - Tumour-to-tumour metastasis from papillary thyroid carcinoma withBRAFmutation to lung adenocarcinoma withEGFRmutation: the utility of mutation-specific antibodies
Yuki Katsuya, Akihiko Yoshida, Shun-ichi Watanabe, Koji Tsuta
Histopathology.2015; 67(2): 262. CrossRef - Pulmonary metastasis of a papillary thyroid carcinoma and primary lung adenocarcinoma: two coincident carcinomas at the same location
Liyan Xue, Zhonghua Luan, Ying Liu, Shuangmei Zou, Jun Jiang, Ning Wu, Ning Lu, Dongmei Lin
Diagnostic Pathology.2013;[Epub] CrossRef
 PubReader
PubReader Cite this Article
Cite this Article